
Abstract
Stereotactic radiosurgery provides conformal treatment of intracranial lesions, but when multiple lesions are treated, cumulative dose to structures such as the hippocampi may be increased. We analyzed hippocampal dose for patients treated with radiosurgery for multiple brain metastases. We then investigated a means to minimize hippocampal dose. We randomly selected 8 patients treated with single-session, frame-based radiosurgery for 6 to 12 intracranial metastases. Standard planning was employed to deliver 16 to 20 Gy to each lesion without hippocampal avoidance. Each case was replanned using the software’s dynamic shaping function to minimize direct beam hippocampal irradiation, while maintaining conformality and target coverage. With standard planning, the maximum hippocampal dose varied from 0.8 to 9.0 Gy but was >3 Gy only when a lesion was <10 mm from the hippocampus. There was no clear correlation between hippocampal dose and the number or the total volume of lesions. Replanning with direct beam avoidance decreased the mean hippocampal dose by an average of 35% but increased treatment time by a mean of 20%. Sparing was most pronounced when the closest lesion was in close proximity to the hippocampus. This is the first study reporting hippocampal dose for multilesion intracranial radiosurgery. It illustrates that when multiple intracranial targets are treated with radiosurgery, substantial hippocampal dose can result. Active beam shielding and optimization can lower hippocampal dose, especially with lesions <10 mm from the hippocampus. These results raise the prospect that the risk of neurocognitive side effects may be further decreased with a hippocampal-sparing approach.
Introduction
Among patients with cancer, an estimated 9% to 17% develop brain metastases. 1 When several intracranial metastases occur, radiation therapy options include whole brain radiation and stereotactic radiosurgery, either alone or in combination. Although whole brain radiation can be effective in controlling microscopic disease not yet apparent on imaging, it can lead to permanent cognitive deficits and decreased quality of life. 2,6
Several investigations with dosimetric and animal models have implicated dose to the hippocampi as an important contributing factor to the cognitive deficits following whole brain radiation. 3,4 Although the precise threshold doses for the associated structures are not currently known in humans, multiple studies have implicated irradiation of the hippocampus in cognitive deficits after radiation therapy for nasopharyngeal, maxillary, skull base, and pituitary tumors. 5,7 –9 Furthermore, initial results for the RTOG 0933 phase II clinical trial suggest that hippocampal-sparing whole brain radiation results in less of a cognitive decline, reinforcing the likely importance of decreasing hippocampal dose. 10
Stereotactic radiosurgery is able to achieve a sharp dose gradient surrounding a target, which can potentially minimize near range and distal scattering dose to normal structures, such as the hippocampi. However, when larger numbers of brain metastases are treated in a single radiosurgery session, a large number of beams are often involved, covering wide solid angles. Concern then arises that the cumulative dose to the hippocampi could increase substantially. This then increases the concern for subsequent cognitive side effects.
In order to study the cumulative hippocampal dose with radiosurgery for multiple brain metastases, we first performed a dosimetric study of a simulated case treated for 12 intracranial metastases with Gamma Knife Perfexion (Elekta, Stockholm). In a simulated treatment planning study, we determined the dose to the hippocampi first when all 12 lesions were treated and then when a random subset of 9, 6, or 3 lesions was treated. We then studied the effect of active beam shielding on minimizing hippocampal dose in each case. Finally, we validated the results using 7 additional patients. Our study aims to (1) provide insight into the level of hippocampal dose that can be achieved with the state-of-the-art radiosurgical treatment of multiple brain metastases and (2) illustrate the rationale and the effect of proactive beam shaping on hippocampal dose.
Methods
For the initial simulated study, all 12 intracranial metastases were contoured on a planning computed tomography (medical comorbidities precluded magnetic resonance imaging). The subgranular zones of the right and left hippocampi were contoured according to RTOG 0933 guidelines (available on www.rtog.org). The contours followed the grey matter at the medial aspect of the lateral ventricles, from the lateral horns anteriorly to the atria posteriorly.
Planning was performed with the Leksell Gamma Plan (LGP, version 10.1) for treatment with a Gamma Knife Perfexion. For the initial sample patient, all 12 lesions were planned for single-session treatment. Twelve Gy was prescribed to cover >99% of each lesion in a conformal manner. We then repeated the analysis for a random subset of 9, 6, or 3 lesions planned for a single session. The lesions were arrayed so that they were not closely clustered. The mean, maximum, and minimum dose to the hippocampi were calculated by the LGP volume analysis tool. Treatment times were also calculated by the software, using a reference dose rate of 3.357 Gy/min. For plans with hippocampal avoidance, the dynamic shaping function was used to avoid direct beam irradiation, with adjustments made as necessary to maintain a similar target coverage and conformality as the original treatment plan.
To validate the general conclusions with the sample patient, 7 additional patients were randomly selected. Each was recently treated at our institution with Gamma Knife radiosurgery in a single session for 6 to 12 intracranial metastases, without any specific attempt to spare the hippocampi. Their original treatment plans were used, delivering between 16 and 19 Gy to each lesion, prescribed to the 50% to 90% isodose line, with dose dependent on lesion size. The hippocampi were contoured according to the RTOG 0933 guidelines, and dose was calculated in the same manner as the original treatment plan using the LGP tool. Each case was replanned with hippocampal avoidance using the dynamic shaping function of the LGP, as mentioned earlier. Treatment length was compared using a paired t test (Microsoft Excel).
Results
The initial sample patient had 12 brain metastases scattered throughout the parenchyma, with lesion characteristics described in Table 1. The lesions ranged in size from 0.05 to 0.97 cm3, with the closest distance between the lesion and the hippocampal surface ranging from 0.8 to 7.7 mm.
Lesion Location and Characteristics for an Initial Sample Patient.a

aThe targets used for each subset analysis are also indicated.
To determine the effect of multiple metastasis treatment on hippocampal dose, treatment planning was completed to deliver 20 Gy to each lesion in a single fraction, first without special attention to hippocampal dose. As shown in Table 2, when all 12 lesions were treated, the maximum dose was 4.6 Gy to the left hippocampus and 4.5 Gy to the right. The mean dose was 2.3 Gy to the left hippocampus and 2.9 Gy to the right.
Hippocampal Dose and Treatment Times for A Sample Patient, Using Different Subsets of Lesions With or Without Proactive Beam Shaping.

aMean, minimum, and maximum doses are shown for the right and left hippocampi. All doses are in Gy. Treatment time in minutes is also shown.
To determine the effect when smaller numbers of metastases are treated, we calculated the hippocampal dose when a subset of 9, 6, or 3 lesions is treated. The lesions included in each plan are indicated in Table 1. As shown in Table 2, when fewer lesions are treated, there is a corresponding decrease in maximum, mean, and minimum hippocampal dose.
A sample plan for 1 lesion with active beam shaping, compared to the original plan, is shown in Figure 1. When dynamic shaping is employed, the maximum hippocampal dose is decreased in all cases, by at least 40% (Table 2). However, the decreased hippocampal dose comes at the cost of a longer treatment time, which was increased by nearly 50% in the 12-lesion plan, from 158 to 234 minutes.
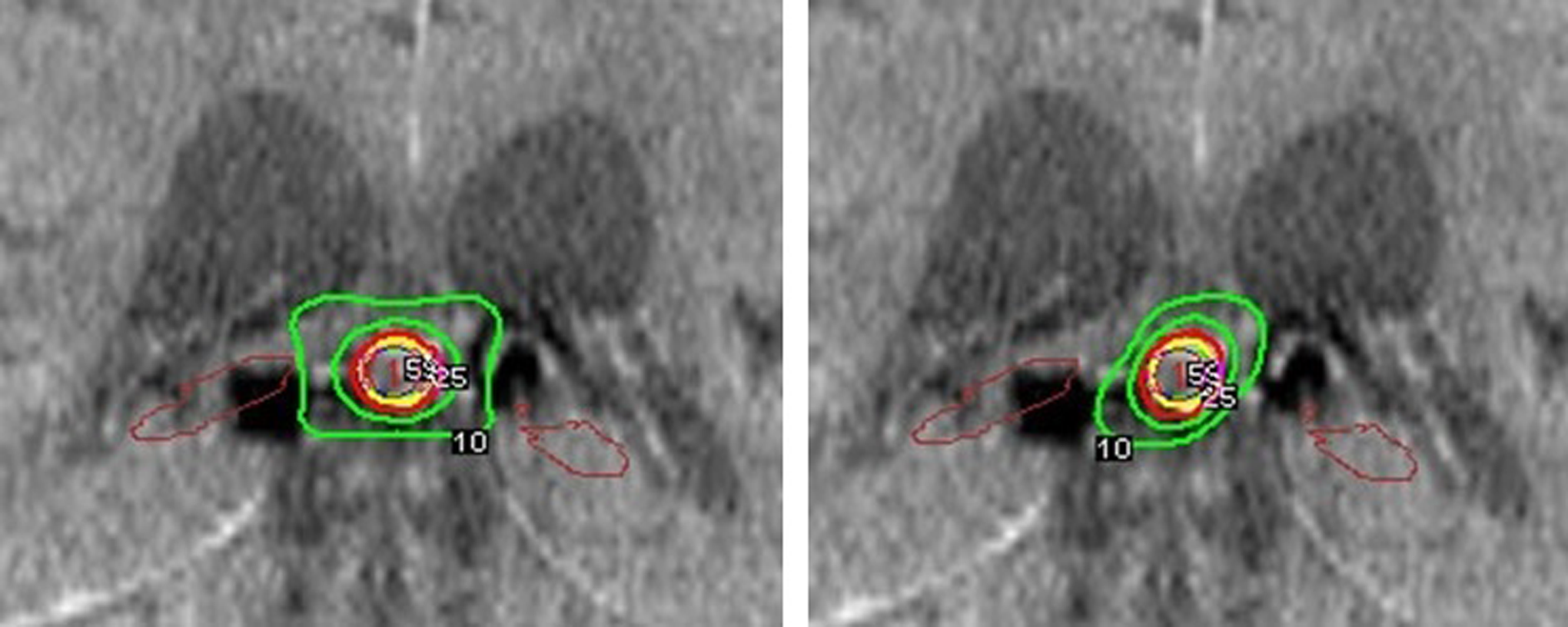
Sample plan for 1 lesion planned for Gamma Knife radiosurgery without (left) or with (right) proactive beam shaping. Shown is the contoured target (yellow) and 3 isodose lines (red: prescription, green: 25%, green: 10%) [Color version of the figure available online].
To determine the generalizability of the findings from the initial patient, we analyzed hippocampal dose for 7 additional radiosurgery patients, whose characteristics are shown in Table 3. As shown in Table 3, the mean hippocampal dose ranged from 0.4 to 1.6 Gy for these cases. The highest maximum hippocampal dose was 9 Gy in a patient with a lesion of 3.2 mm from the right hippocampus. Another patient with a lesion 7.5 mm from the left hippocampus received a maximum hippocampal dose of 4 Gy.
Lesion and Plan Characteristics for 7 Additional Patients Planned With or Without Proactive Beam Shaping.

aMean, minimum, and maximum doses are listed for the right and left hippocampi. All doses are in Gy. Treatment time in minutes is also shown.
The result of active beam shielding for each case is shown in Table 3. For the patient with a lesion 3.2 mm from the right hippocampus, use of dynamic shaping decreased the maximum right hippocampus dose from 9 to 6.2 Gy, with a decrease in mean dose from 1.9 to 0.9 Gy. The shaped plan had a 22-minute increase in treatment time. Dynamic shaping had the least effect on hippocampus dose for the patient with 8 lesions that were all >26 mm from the hippocampus. The mean and maximum dose was decreased by at most 0.1 Gy, with a 5-minute increase in treatment time. Overall, hippocampal sparing led to a mean decrease of 35% in hippocampal mean dose, although the magnitude varied widely, ranging from a 77% decrease to no change.
Overall, for every lesion treated, the right and left hippocampi received a mean dose of 0.117 and 0.107 Gy, respectively, without hippocampal avoidance. When hippocampal sparing was used, the mean hippocampal dose per treated lesion decreased to 0.06 Gy for the right and 0.058 Gy for the left. The treatment time with dynamic shaping differed significantly (P = .003) with hippocampal sparing, with a mean increase of 20%.
Discussion
This study examines the dose to the hippocampi during typical treatments of multiple brain metastases with frame-based radiosurgery, as well as the effect of a simple hippocampal avoidance technique that can be readily implemented in the clinic. Our results suggest that proactive hippocampal avoidance is justifiable for the purpose of minimizing hippocampal dose in radiosurgery for multiple brain metastases.
At present, dose limits for the human hippocampi have not yet been elucidated, making it difficult to weigh the cost of a hippocampal-sparing approach against the potential benefits. However, the initial results from the phase II RTOG 0933 trial suggest that constraining hippocampal dose to a D100% of 10 Gy in 10 fractions leads to improved neurocognitive outcomes compared to historical controls receiving 30 Gy in 10 fractions without hippocampal sparing. 10 Furthermore, studies in mice suggest that as little as 2 Gy can result in histologic changes in the hippocampi. 3
Our study illustrates that treatment of multiple lesions in a single session of Gamma Knife radiosurgery can lead to a mean dose on the order of 3 Gy, with a maximum dose of up to 9 Gy. However, avoidance of direct beam irradiation can decrease the hippocampal dose by an average of 35%, while maintaining conformality and target coverage. The level of sparing is most pronounced when targets are located nearer to the hippocampi, especially within 10 mm. The main cost for hippocampal sparing is an increased treatment time, with a mean increase of 20% in this group of patients.
Our study suggests that cases with lesions in close proximity to the hippocampi—especially <10 mm—would derive the greatest benefit from a hippocampal-sparing approach. However, when lesions are not adjacent to the hippocampi, our results suggest that the dose to the hippocampi is generally on the order of 1 Gy or less, even when large numbers or large volumes of lesions are treated with Gamma Knife radiosurgery. Whether such a result holds for other radiosurgical modalities such as CyberKnife or Linac-based systems remains to be investigated. The results presented here can serve as a benchmark for such an investigation.
Conclusions
In summary, this study suggests that with the treatment of multiple brain metastases with single-session radiosurgery, the cumulative dose to the hippocampi should be carefully assessed during the treatment planning process. Avoidance of direct beam irradiation can be used to decrease hippocampal dose, especially when lesions are within 10 mm of the hippocampi.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr Barani received research grant support from BrainLab, Elekta, and the NIH. Dr Sneed received an honorarium from Elekta to attend a meeting.