
Abstract
Background:
The aim of this study was to evaluate the efficacy and toxicity of robotic CyberKnife (Accuray Incorporated, Sunnyvale, California)-based stereotactic body radiation therapy (SBRT) in patients with recurrent or metastatic abdominopelvic tumors.
Methods and Materials:
A total of 69 patients treated between May 2008 and January 2011 were evaluated retrospectively. Indication for SBRT was persistent disease in 3 (4%) patients, local recurrence in 29 (42%) patients, regional recurrence in 13 (19%) patients, and oligometastatic disease in 24 (35%) patients. Forty-two (61%) patients were previously irradiated to the same region and 27 (39%) patients were treated for the first time. The median age was 59 years (range, 24-86 years). There were 31 (45%) male and 38 (55%) female patients. The median total dose was 30 Gy (range, 15-60 Gy) delivered with a median 3 fractions (range, 2-5 fractions). The tumor response to treatment was assessed by computed tomography, magnetic resonance imaging, or positron emission tomography.
Results:
At the 12-month (range, 2-44 months) median follow-up, local control was 65% and median overall survival (OS) was 20 months. A larger gross tumor volume (≥ 67 cm3) was significantly correlated with worse 1-year OS (81% vs 48%, P = .03). The patients with local recurrence occurring <11 months had a significantly shorter 1-year local control rate than patients with ≥11 months (31% vs 91%, P < .001). Grade 3-4 acute and late toxicities were seen in 7% and 15% of patients, respectively. The patients with previous radiotherapy history had significantly higher rate of acute toxicity (19% vs 0%, P = .019). Late toxicity was significantly higher in pelvic tumors than in abdominal tumors (3% vs 28%, P = .004).
Conclusion:
The SBRT seems to be feasible and resulted in good treatment outcomes in patients with recurrent or metastatic abdominopelvic tumors.
Introduction
Stereotactic body radiation therapy (SBRT) is an effective and minimally invasive delivery of ablative or high-dose radiation for extracranial tumors. 1 This technique provides precisely directed, high-dose radiation to the target volumes while minimizing radiation dose to the surrounding normal tissues. It was first performed in patients with primary lung cancer and hepatocellular carcinoma. 2 As experience with SBRT in the treatment of prostate and pancreatic cancer increases, application of this therapeutic modality for abdominopelvic tumors is evolving rapidly. 3,4
The liver and the adrenal gland are the main site of metastasis for many primary cancers. 5,6 SBRT also can be performed in patients with unresectable liver and adrenal gland metastasis. 7 -12 Recently, SBRT has gained importance in the treatment of oligometastases. Several nonrandomized studies have demonstrated that SBRT is a safe and effective technique for treating oligometastatic disease, with a local control rate of approximately 80%. 13 -15
Another clinical application of SBRT is the treatment of recurrent abdominopelvic tumors. 16 Therapeutic options are often limited in case of recurrence after both primary surgery and radiotherapy (RT). The safe reirradiation of patients with conventional RT is difficult due to the risk of normal tissue toxicity. Thus, SBRT has become an important therapeutic option. Although clinical experience and the number of studies are limited to date, SBRT reirradiation has shown promising results with high rates of local tumor control and low rates of toxicity. 16,17
These findings suggest that aggressive local therapy with SBRT might be feasible particularly in patients with extracranial oligometastases or recurrent disease. Against this background, the purpose of this study was to evaluate the efficacy and toxicity of robotic CyberKnife (Accuray Incorporated, Sunnyvale, California)-based SBRT in patients with recurrent or metastatic abdominopelvic tumors. We also aimed to determine whether any prognostic factor could predict the outcome.
Materials and Methods
Patients
The medical charts of 69 patients treated with robotic SBRT for recurrent or metastatic disease between May 2008 and January 2011 in our department were retrospectively evaluated. This retrospective study was approved by the institutional ethics committee, and informed consent was obtained from each patient prior to treatment.
Treatment Planning and Delivery
All patients were evaluated by diagnostic imaging studies prior to SBRT. SBRT was delivered with the CyberKnife (Accuray Incorporated), an image-guided frameless stereotactic robotic radiosurgery system. A Radiologist implanted at least 3 gold fiducial markers within and around the tumor under computerized tomography (CT) guidance in 35 (51%) patients. Seven to 10 days following fiducial implantation, treatment-planning CT images with intravenous contrast were obtained. All patients were immobilized in the supine position. The delineation of the gross tumor volume (GTV) and the organs at risk were carried out on the planning CT and fused with the pretreatment CT or magnetic resonance imaging (MRI) images. In most cases, the clinical target volume (CTV) was equal to the GTV. Planning target volume (PTV) was determined by adding a 5 mm margin around the CTV. Treatment plans were generated on Multiplan treatment planning system (version 2.2.0, Accuray Incorporated) and ray-tracing algorithm was used.
Fraction dose and total dose were determined by tumor type, previous radiation history, and target proximity to critical structures. The prescription dose was delivered to the PTV. Minimum dose of target volume and maximum dose of organs at risk were defined. Dose constraints for critical structures were established based on data from Grimm et al. 18 Before each fraction, patients were premedicated with dexamethasone, antiemetic, and H2 receptor antagonist intravenously. Patients were treated on consecutive weekdays or every other day according to the treatment characteristics.
Follow-Up and Toxicity
The tumor response to treatment was assessed by CT, MRI, or positron emission tomography/CT 3 months after the completion of SBRT using the Response Evaluation Criteria in Solid Tumors. 19 Accordingly, disappearance of tumor was considered as “complete response”; > 30% decrease in the sum of the longest diameter of the tumor was considered as “partial response”; > 20% increase in tumor size was considered as “progressive disease”; and ≤ 30% decrease to ≤ 20% increase in tumor size was considered as “stable disease.” Acute and late radiation-induced toxicities were evaluated according to the toxicity criteria of the Radiation Therapy Oncology Group/European Organization for Research and Treatment of Cancer. 20 Any toxicity occurring within 3 months of the treatment was considered acute toxicity, and late toxicity was reported if it appeared more than 3 months after the end of the SBRT.
Relation between toxicity and total radiation dose was evaluated using biological effective dose (BED) calculation. We used a standard formula of BED calculation (BED = nd [1 + d/α/β]). The BED10 Gy and BED2 Gy values of SBRT were calculated accordingly. In patients who underwent previous external beam RT or SBRT, cumulative BED was calculated that was the sum of the BED of the initial irradiation course and the BED of the reirradiation course. All patients were followed up and examined in the sixth week and then every 3 months during the first 2 years, every 6 months during the next 3 years, and annually thereafter. Complete physical examination, laboratory tests, and diagnostic imaging studies were done at the follow-up visits. Follow-up information was obtained from the department charts, any hospital notes, referring doctors, general directorate of population and citizenship affairs, and as a last resort, from patients and/or next of kin.
Statistics
All statistical analysis was conducted using the Statistical Package for the Social Sciences version 18.0 (Chicago, Illinois). All time-related events (failure or death) were calculated from the end of the robotic SBRT to the last follow-up or death. Local control was defined as freedom from local progression during follow-up. Local control and survival analyses were carried out using the Kaplan-Meier method. The impacts of the patient and treatment variables on local control and overall survival (OS) were assessed using the log rank test. Sex, age (< 60 vs ≥ 60 years), primary tumor site, SBRT site (abdomen vs pelvis), reason for SBRT, previous RT history (yes vs no), BED2 Gy (< 158 vs ≥ 158 Gy), BED10 Gy (< 60 vs ≥ 60 Gy), treatment schedule (consecutive days vs every other day), number of fraction (1-3 vs 4-5), time of recurrence (≤11 months vs > 11 months), and tumor volume (< 67 vs ≥ 67 cm3) were included for analysis. The Cox proportional hazards test was used for multivariate analysis. Correlation between toxicity/survival and clinical/treatment parameters was determined using the Fisher exact chi-square test for categorical variables and the Mann Whitney U test for numerical variables. All analysis used the conventional P < .05 level of significance.
Results
Patient and Treatment Characteristics
Patient and treatment characteristics are summarized in Table 1. Sixty (87%) patients underwent surgery after initial diagnosis. Fifty-nine (86%) patients had received chemotherapy prior to SBRT, and 25 of them were treated concomitantly with RT. Seven patients with gynecological tumors underwent brachytherapy after external beam RT. The median prior dose of the external beam RT was 50.4 Gy (range, 12.6-60 Gy) with a median 1.8 Gy (range, 1.8-3 Gy) per fraction.
Patient, Tumor, and Treatment Characteristics.

Abbreviations: GI, gastrointestinal; GU, genitourinary; RT, radiotherapy; SBRT, stereotactic body radiotherapy; LR, local recurrence; RR, regional recurrence.
Median interval between external beam RT and robotic SBRT was 18 months (range, 1-132 months). Indication for SBRT was persistent disease in 3 (4%) patients, local recurrence in 29 (42%) patients, regional recurrence in 13 (19%) patients, and oligometastatic disease in 24 (35%) patients. SBRT was applied to abdominal region in 38 (55%) patients and pelvic region in 31 (45%) patients. Sites treated include lymph nodes (n = 21), vagen/cervix (n = 10), pancreas (n = 8), liver (n = 8), adrenal gland (n = 7), presacral (n = 6), and other (n = 9). Forty-two (61%) patients were previously irradiated with external beam RT to the same region.
The median GTV was 67 cm3 (4-1094 cm3). The median prescription dose was 30 Gy (range, 15-60 Gy) delivered with a median 3 fractions (range, 2-5 fractions). Sixty-one (88%) patients were treated on consecutive weekdays, and 8 (12%) patients were treated every other day. The median prescription isodose line was 79% (range, 60%-87%). The maximum point dose within the PTV ranged from 18 to 75 Gy (median, 38 Gy).
The median BED10 Gy was 101 Gy (range, 38-195 Gy) and the median BED2 Gy was 240 Gy (range, 88-684 Gy). For SBRT, the median BED2 Gy was 158 Gy (range, 38-660 Gy) and the median BED10 Gy was 60 Gy (range, 20-180 Gy). The median cumulative BED2 Gy was 220 Gy (range, 88-660 Gy) and the median cumulative BED10 Gy was 101 Gy (range, 38-180 Gy).
Tumor Response
Median follow-up for all patients was 12 months (range, 2-44 months). No patient was lost to follow-up. The overall response rate after SBRT was 51% (8% complete response and 43% partial response) at the time of the first follow-up. Stable and progressive disease rates were 35% and 11%, respectively. After a median follow-up of 12 months, 14 (20%) patients had complete response, 18 (26%) had partial response, 13 (19%) had stable disease, and 24 (35%) had progression. Thirty-eight (55%) patients had systemic disease at the last follow-up. Table 2 demonstrates detailed patient outcomes at the last control.
Clinical Outcome.
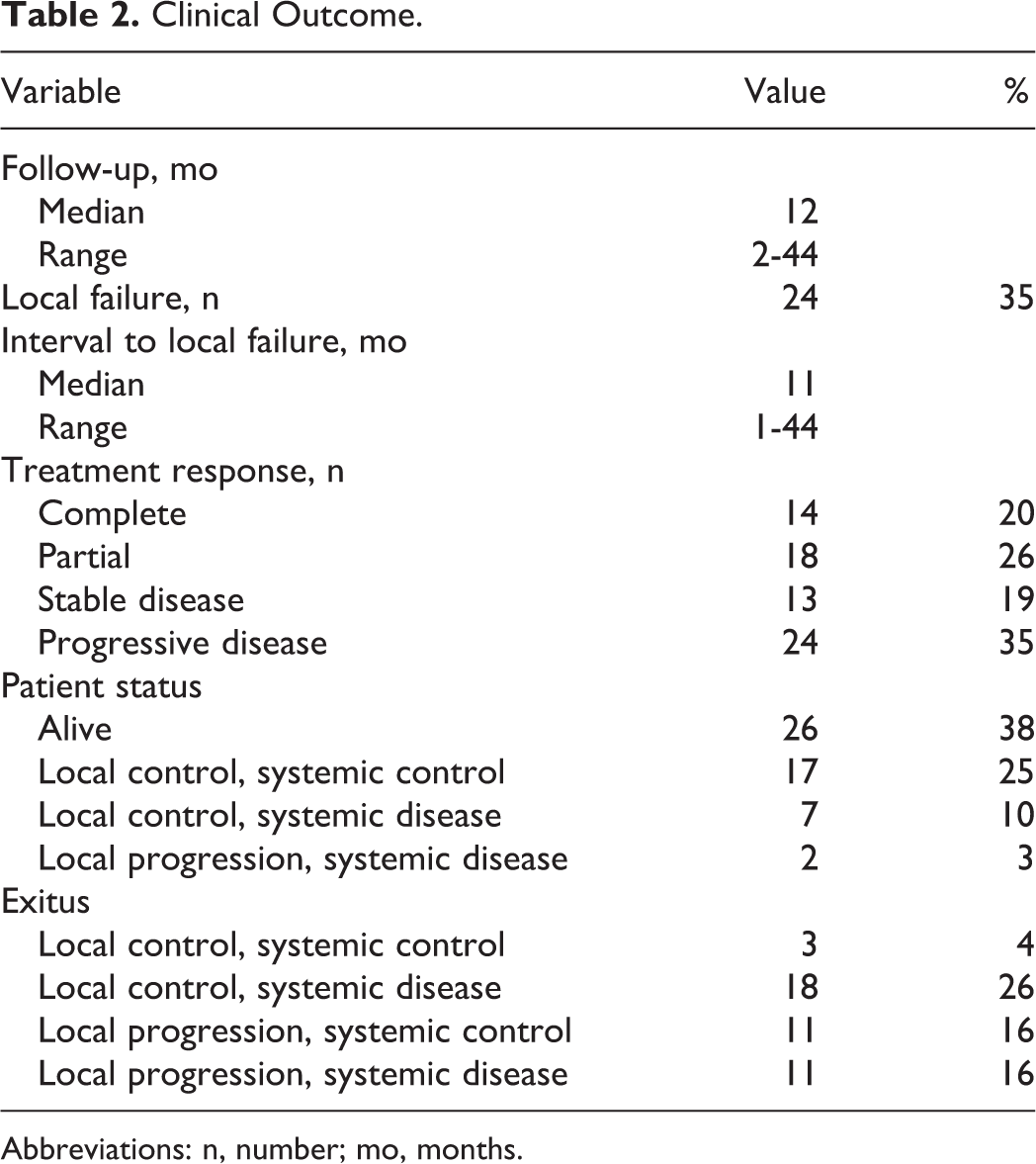
Abbreviations: n, number; mo, months.
Local Control
During the follow-up, local recurrence occurred at median 11 months (range, 1-44 months) after SBRT. At the 12-month median follow-up, local control was 65%. At the time of analysis, 18 (26%) patients were alive with disease, 8 (12%) were alive with no evidence of disease, whereas 22 (32%) patients had died due to progressive disease. At the last follow-up, 45 (65%) patients had local control and remaining 24 (35%) patients had local progression at treated site. Among patients with progressive disease, 11 (46%) patients were presented with only progression in treated site, and remaining 13 (54%) had progressive systemic disease. Among patients with local control (n = 45), 25 (56%) developed systemic disease during follow-up.
The 1-, 2-, and 3-year LC rates were 67%, 61%, and 55%, respectively (Figure 1). Patients with adrenal gland metastases had the longest 1-year local control. Local control according to patient and treatment characteristics is presented in Table 3.

Kaplan-Meier estimate of local control for all patients.
Univariate Analysis of Prognostic Factors for 1-Year Local Control and Overall Survival.
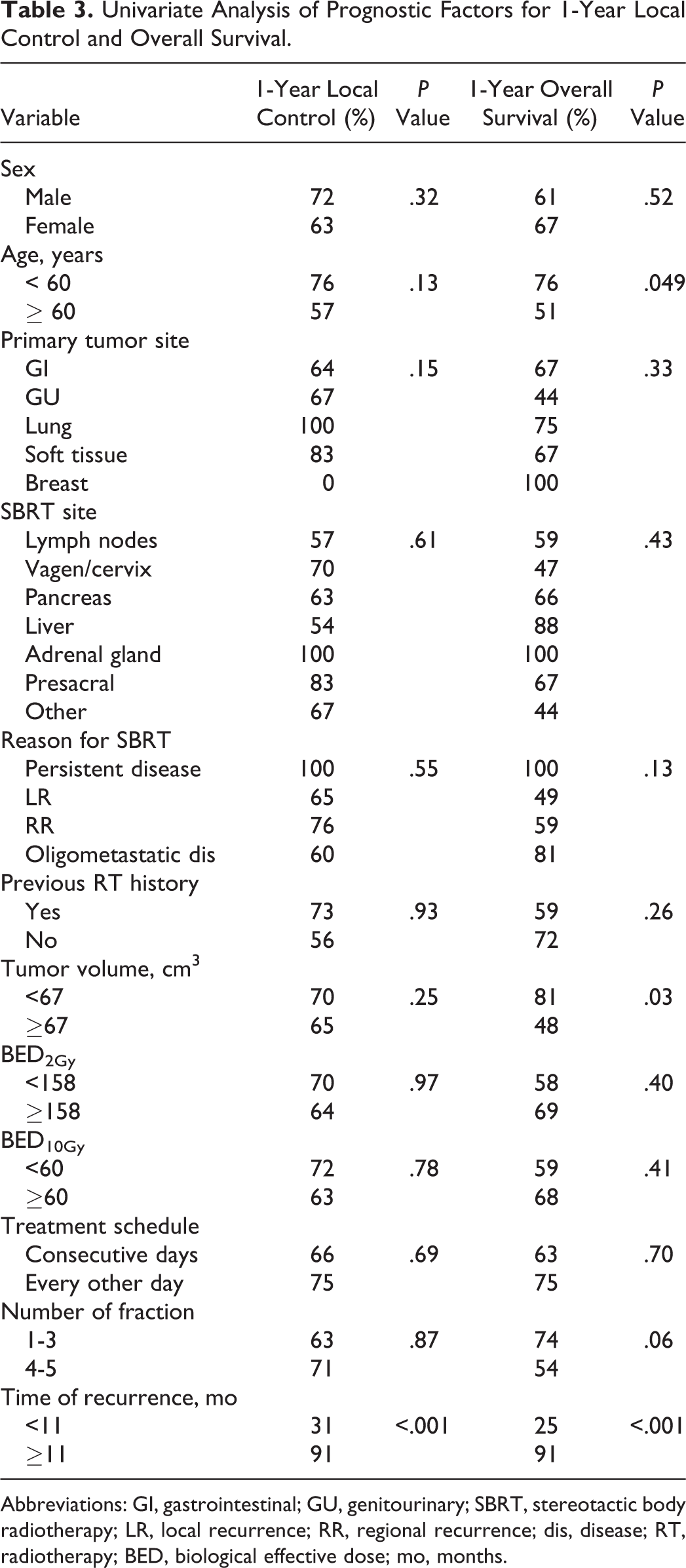
Abbreviations: GI, gastrointestinal; GU, genitourinary; SBRT, stereotactic body radiotherapy; LR, local recurrence; RR, regional recurrence; dis, disease; RT, radiotherapy; BED, biological effective dose; mo, months.
The patients with local recurrence occurring <11 months had a significantly shorter 1-year local control rate than patients with ≥11 months (31% vs 91%, P < .001). There were no significant differences in 1-year OS regarding sex (P = .32), age (P = .13), primary tumor site (P = .15), SBRT site (P = .61), reason for SBRT (P = .55), previous RT history (P = .93), tumor volume (P = .25), BED2 Gy (P = .97), BED10 Gy (P = .78), treatment schedule (P = .69), and number of fraction (P = .87).
Overall Survival
At the time of analysis, 26 (38%) patients were alive and 43 (62%) had died. Forty (93%) patients died due to tumor progression, 2 (5%) died due to cardiac reasons, and 1 (2%) died due to renal failure. The median OS of all patients was 20 months (95% confidence interval [CI]; range, 11-29 months). The 1-, 2-, and 3-year OS rates were 64%, 43%, and 19%, respectively (Figure 2). The patients who were < 60 years had a significantly better 1-year OS than patients ≥60 years (76% vs 51%, P = .049; Figure 3). Tumor volume was also significantly correlated with 1-year OS, which was longer in patients with a tumor volume < 67 cm3 compared to ≥ 67 cm3 (81% vs 48%, P = .03; Figure 4). There were no significant differences in 1-year OS regarding sex (P = .52), primary tumor site (P = .33), SBRT site (P = .43), reason for SBRT (P = .13), previous RT history (P = .26), BED2 Gy (P = .40), BED10 Gy (P = .41), treatment schedule (P = .70), number of fraction (P = .06). The patients with local recurrence occurring <11 months had a significantly shorter 1-year OS rate than patients with ≥11 months (25% vs 91%, P < .001). The OS according to patient and treatment characteristics is presented in Table 3.

Kaplan-Meier estimate of overall survival for all patients.

Kaplan-Meier curves of local control (A) and overall survival (B) according to age.

Kaplan-Meier curves of local control (A) and overall survival (B) according to tumor volume.
Multivariate analysis showed only time of recurrence to be significant prognostic factor of local control (hazard ratio [HR] 22.1; 95% CI, 4.97-98.21; P < .001) and OS (HR 7.37; 95% CI, 3.19-16.99; P < .001).
Toxicity
Acute toxicities were observed in 8 (12%) patients. Five (7%) of these patients had grade 3-4 acute toxicity. Late toxicities were observed in 10 (15%) patients: 4 with ileus (grade 3), 2 with rectovaginal fistula (grade 4), 2 with intestinal perforation (grade 4), 1 with skin fistula (grade 4), and 1 with renal toxicity (grade 3). Table 4 summarizes tumor and treatment characteristics of patients developing late toxicity.
Tumor and Treatment Characteristics of Patients Developing Late Toxicity.
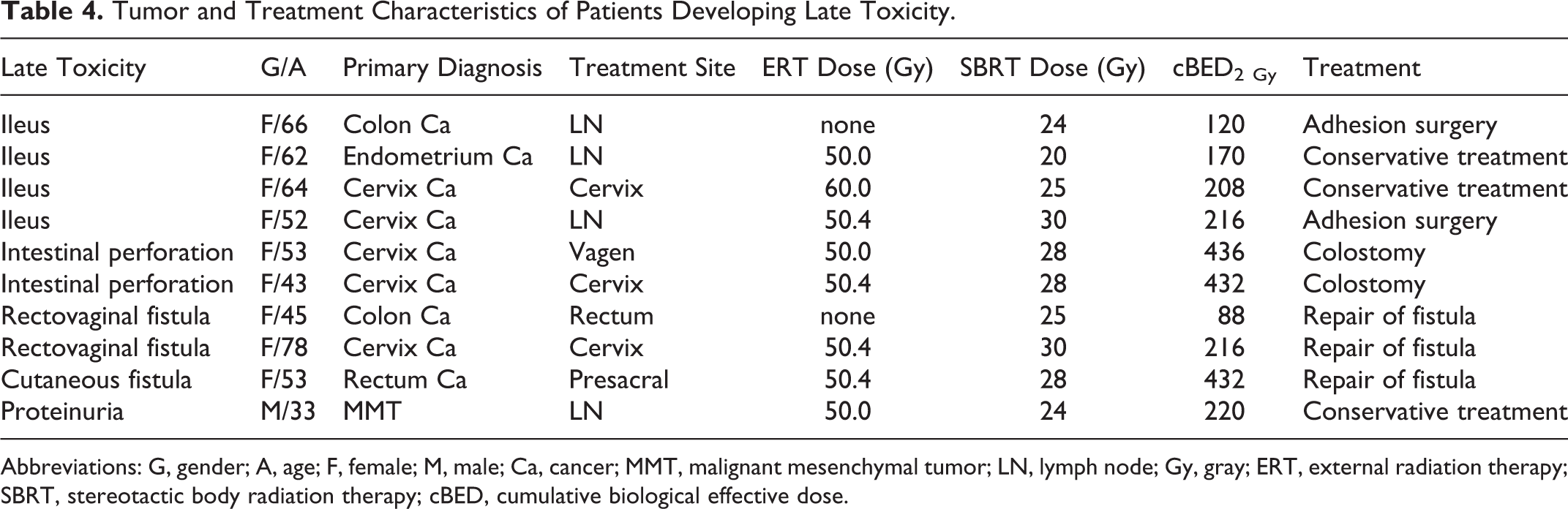
Abbreviations: G, gender; A, age; F, female; M, male; Ca, cancer; MMT, malignant mesenchymal tumor; LN, lymph node; Gy, gray; ERT, external radiation therapy; SBRT, stereotactic body radiation therapy; cBED, cumulative biological effective dose.
The patients with previous RT history had significantly higher rate of acute toxicity compared to no RT history (19% vs 0%, P = .019). However, there was no significant difference in late toxicity (21% vs 4%, P = .76). No association was found between acute toxicity and SBRT site (abdomen vs pelvis; 5% vs 19%, P = .13). However, the rate of late toxicity was higher in pelvic tumors than abdominal tumors (3% vs 28%, P = .004). It was found that acute (6% vs 17%, P = .26) and late (9% vs 20%, P = .31) toxicities were not correlated with tumor volume (< 67 vs ≥ 67 cm3). There was no association between acute toxicity and cBED10 Gy (< 101 vs ≥ 101 Gy; 5% vs 18%, P = .14) or late toxicity and cBED2 Gy (< 220 vs ≥ 220 Gy; 18% vs 11%, P = .50).
Discussion
The SBRT can be used in the treatment of selected metastatic and recurrent patients whose tumors are not amenable to surgery. It is a noninvasive procedure compared to other local treatment strategies. It is also feasible and generally well tolerated with acceptable toxicity profiles.
The use of SBRT in oligometastatic disease, defined as fewer than 5 lesions, shows encouraging preliminary results and still under investigation. 21,22 Rwigema et al reported the treatment results of 38 patients with 44 unresectable nodal and soft tissue oligometastases in the abdominopelvic region. 23 They underwent a median dose of 40 Gy (24-50 Gy) in 4 to 5 fractions. Increasing SBRT dose and smaller GTV were associated with improved LC. In another study, 69 patients with 94 abdominal oligometastases were evaluated and overall survival rates were found significantly higher in favorable histology cases (prostate and kidney tumors). 24 In the largest study, Fastaia et al reported treatment results of 993 patients with 1363 metastatic foci. 25 Local control rate, at a median 7.7 months of follow-up, was 82% for all patients and 76% for patients with liver metastases (n = 530). Our results are comparable with previously reported findings. In the current study, the 1-year OS and local control rates were 64% and 67% for all patients and 88% and 54% for liver metastases, respectively. Although the OS rates were higher in liver metastases, low rates of local control might be due to small number of patients with liver metastasis.
SBRT is an alternative treatment option to surgery in patients with adrenal gland metastases; however, clinical experience is limited. Holy et al evaluated local control rates in 13 patients with isolated adrenal gland metastasis who were treated with SBRT. 12 At a median 21 months after SBRT, the local control rate was 77% and median OS was 23 months, which was similar to the data of surgical series. Casamassima et al treated 48 patients with SBRT for adrenal gland metastases. 11 They reported 1-year local control and OS rates as 90% and 40%, respectively. In another study by Chawla et al, 30 patients with adrenal gland metastasis were treated with SBRT. 26 They reported 1-year OS and local control rates as 44% and 55%, respectively. These rates were quite low compared to those of the present study. In our study, patients with adrenal gland metastasis had the highest 1-year local control (100%) and OS survival (100%). These higher rates could be attributed to the differences in the total dose and primary disease status.
In recurrent abdominopelvic tumors, curative surgical resection is often difficult and highly morbid. Thus, SBRT could be an attractive treatment option especially for patients treated with previous RT. There are several studies reporting on SBRT for recurrent gynecological and colorectal cancer. However, there are no standard treatment suggestions for these tumors. Dewas et al reported a series of 16 patients in whom SBRT was used for lateral pelvic recurrences. 27 Patients were treated with 6 × 12 Gy. They reported 1-year local control and OS rates of 51% and 46%, respectively. Defoe et al analyzed 14 previously irradiated patients treated with SBRT for presacral recurrent adenocarcinoma of the rectum. 28 The 1- and 2-year local control and OS rates were 91%, 68% and 90%, 79%, respectively. In our series, 6 patients had been treated with SBRT for recurrent presacral mass. At the median 12-months follow-up, the 1-year local control and OS rates were 83% and 67%, respectively.
In our recurrent gynecological patients, the 1-year local control rate was 70%, and OS was 47%. All of them had previous RT history. Guckenberger et al treated 19 patients with recurrent gynecological tumors with SBRT. 29 The majority (n = 16) of these patients underwent SBRT as a boost after conventional RT. At a median follow-up of 22 months, the 3-year local control and OS for the entire group were 81% and 34%, respectively. Deodato et al reported local control and 2-year OS as 83% and 64%, respectively, after SBRT in 11 patients with recurrent gynecological cancer within a median follow-up of 19 months. 30 The median tumor volume was 42 cm3 in the study by Deodato et al compared to 93 cm3 in our study. 30 Better local control and survival rates in the above-mentioned studies than the present study suggest that tumor volume, stage, and total dose might be important.
There is no consensus about the optimal treatment of recurrent pancreatic or periampullary tumors. Rwigema et al reported a series of 71 patients treated with SBRT for locally advanced pancreatic adenocarcinoma. 31 Results of that study suggested that patients with recurrent (n = 11) and metastatic (n = 8) pancreatic cancer had the lowest local control rates. The median survival was 13 and 3 months, respectively. In our study, 8 patients who underwent SBRT due to recurrent pancreatic tumor had low 1-year local control rate (63%). Although 7 of the 8 patients had been irradiated previously, survival was longer in our series (1-y OS 66%) as compared with the literature.
A number of prognostic factors have been demonstrated in the treatment of oligometastatic disease. Long disease-free interval, breast histology, 1 to 3 metastases, small tumor volume, and higher radiation dose delivered (BED > 100 Gy) were found to be a positive prognostic factor for local control and survival. 21,32 Likewise, we found that the age, GTV, and time of recurrence correlated with OS. We also found that the patients with local recurrence occurring < 11 months had a significantly shorter 1-year local control rate than patients with ≥11 months (31% vs 91%, P < .001).
In our series, the patients with previous RT history had significantly higher rate of acute toxicity compared to no RT history (19% vs 0%, P = .019). We also found that the incidence of late toxicity was significantly higher in pelvic tumors (3% vs 28%, P = .004). The median BED10 and BED2 were 60 and 180 Gy for abdominal tumors and 47 and 120 Gy for pelvic tumors, respectively. Contrary to expectations, doses were higher in abdominal tumors where toxicity was lower. No significant difference was found in relation to total dose and toxicity. However, the median tumor volume was higher in pelvic tumors as compared to abdominal tumors (80 vs 35 cm3).
In conclusion, SBRT is increasingly becoming a more important part of the treatment of recurrent and metastatic abdominopelvic tumors. Our study has several number of limitations due to its retrospective nature. The effect of prognostic factors on local control and OS was limited owing to the limited number of patients. Additionally, type of primary tumor and SBRT sites were heterogeneous. Despite these limitations, SBRT may offer OS and local control benefit particularly in patients with small tumors. We believe that SBRT will have an important role for selected patients with oligometastatic disease. Further prospective studies with longer follow-up periods are awaited.
Footnotes
Acknowledgments
This study was supported by a Hacettepe University research grant (1-05 A 101 009).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.