
Abstract
Background:
Ga-68-macroaggregated albumin (68Ga-perfusion) positron emission tomography/computed tomography (PET/CT) is a novel imaging technique for the assessment of functional lung volumes. The purpose of this study was to use this imaging technique for functional adaptation of definitive radiotherapy plans in patients with non-small cell lung cancer (NSCLC).
Methods:
This was a prospective clinical trial of patients with NSCLC who received definitive 3-dimensional (3D) conformal radiotherapy to 60 Gy in 30 fx and underwent pretreatment respiratory-gated (4-dimensional [4D]) perfusion PET/CT. The “perfused” lung volume was defined as all lung parenchyma taking up radiotracer, and the “well-perfused” lung volume was contoured using a visually adapted threshold of 30% maximum standardized uptake value (SUVmax). Alternate 3D conformal plans were subsequently created and optimized to avoid perfused and well-perfused lung volumes. Functional dose volumetrics were compared using mean lung dose (MLD), V5 (volume receiving 5 Gy or more), V10, V20, V30, V40, V50, and V60 parameters.
Results:
Fourteen consecutive patients had alternate radiotherapy plans created based on functional lung volumes. When considering the original treatment plan, the dose to perfused and well-perfused functional lung volumes was similar to that of the conventional anatomical lung volumes with an average MLD of 12.15, 12.67, and 12.11 Gy, respectively. Plans optimized for well-perfused lung improved functional V30, V40, V50, and V60 metrics (all P values <.05). The functional MLD of well-perfused lung was improved by a median of 0.86 Gy, P < .01. However, plans optimized for perfused lung only showed significant improvement in the functional V60 dose parameter (median 1.00%, P = .04) but at a detriment of a worse functional V5 (median 3.33%, P = .05).
Conclusions:
This study demonstrates proof of principle that 4D-perfusion PET/CT may enable functional lung avoidance during treatment planning of patients with NSCLC. Radiotherapy plans adapted to well-perfused but not perfused functional lung volumes allow for reduction in dose to functional lung using 3D conformal radiotherapy.
Keywords
Introduction
Local treatment failures are still a major cause for the disappointing outcomes for patients with nonsmall-cell lung cancer (NSCLC) treated with radiotherapy. Locoregional failures still occur in up to 37% of patients 1 and is a major cause of the morbidity and mortality related to this disease. To minimize the risk of failure, the focus of the current international research is on intensification of radiotherapy treatment. Efforts to intensify radiotherapy are severely limited by the need to constrain dose to the surrounding normal lung in order to preserve function. 2 Unfortunately, acute lung injury secondary to radiation therapy (RT) in the form of pneumonitis is a potentially debilitating toxicity, sometimes leading to death of the patient. A recent meta-analysis suggests that symptomatic pneumonitis still occurs in 29.8% of patients and fatal pneumonitis in 1.9%. 3 However, the currently used RT planning constraints that are designed to limit the risk of pneumonitis are based on evidence over a decade old. 4 These constraints are based on population-based volumetric measurements of total irradiated lung irrespective of regional variation in function and do not account for individual variation in pulmonary physiology. Recent efforts to dose escalate without personalizing radiotherapy planning to the individual’s risk of pneumonitis have met with limited or no success. 5 On the other hand, it has been estimated that tumor control probability (or likelihood of cure) for conventional radiotherapy could be improved by ∼50% (from 19.9% to 28.7%) by adaptively intensifying radiotherapy. 6
Ventilation and perfusion (V/Q) imaging is an in vivo technique that measures regional lung function and may be used to individualize lung radiotherapy. Although both V/Q contribute to overall lung function, one does not necessarily match the other. Mismatched perfusion deficits may occur due to vascular disruption or pulmonary embolism, while reverse mismatch may occur due to severe obstructive airways disease 7 or tumor-associated ventilatory obstruction. Assessment of lung perfusion (Q) is particularly relevant to radiation-induced lung damage as, along with pneumocytes, vascular endothelium is considered one of the most radiation-sensitive tissue in the lungs. 8 Preferential sparing of pulmonary parenchyma with intact perfusion during radiotherapy is likely to reduce subsequent vascular injury and may ameliorate the risk of resultant toxicity from pneumonitis. Planar scintigraphy using 99mTc-labeled macroaggregated albumin (MAA) is a long-established imaging standard for functional lung perfusion evaluation. Single positron emission computed tomography (SPECT) is a more modern functional assessment technique enabling 3-dimensional (3D) imaging, 9 which has lead to improved sensitivity, specificity, and reproducibility. 10 -12 The advent of hybrid SPECT/CT devices further improved diagnostic accuracy by enabling anatomic characterization of scintigraphic abnormalities. 13 Perfusion SPECT/CT has been demonstrated to improve functional lung avoidance during lung radiotherapy planning by several groups. 14 -16 However, at present it is unknown which specific threshold of lung perfusion constitutes the most clinically significant functional lung for radiotherapy avoidance. This is an area that warrants further clinical investigation.
Positron emission tomography/computed tomography (PET/CT) offers a unique opportunity to further improve the image quality of functional lung imaging owing to its superior sensitivity for detecting radioactive substances, higher spatial and temporal resolution, and commercial availability of respiratory-gated 4-dimensional (4D) acquisition systems. 17 By substituting the conventional 99mTc radionuclide with 68Ga, a positron emitter, it is now possible to perform CT coregistered perfusion 68Ga-MAA PET. 18 We have previously reported that nongated 3D V/Q PET/CT has superior image quality and provides fully tomographic images with potential for better regional quantitation of lung function when compared to V/Q SPECT/CT in the context of pulmonary embolism. 19 We have further improved this technique through the use of respiratory-gated (4D) acquisition, demonstrating that optimal image registration and spatial fidelity can be achieved using coregistration of specific phases of the 4D PET and 4D CT, 20 thereby reducing blurring caused by respiration motion and resultant artifact at the lung bases.
The purpose of this study is to investigate the utility of 4D perfusion PET/CT in facilitating functional avoidance of the lungs during radiotherapy planning. We aim to use the pretreatment perfusion PET/CT images of patients with NSCLC undergoing curative intent radiotherapy in order to simulate radiotherapy delivery based on avoidance of perfused lung. The central hypothesis of this study is that radiotherapy planning informed by perfusion PET/CT can be used to reduce dose to functional regions of lung.
Materials and Methods
The present work was part of observational prospective clinical trial (Universal Trial Number U1111-1138-4421) of patients undergoing curative intent radiotherapy with or without chemotherapy for NSCLC. This study received institutional review board approval from the Peter MacCallum Cancer Centre. All patients had pretreatment spirometry with testing for diffusing capacity of the lung for carbon monoxide (DLCO). As part of this trial, patients underwent pretreatment perfusion PET/CT. All scans were performed on a GE-Discovery 690 PET/CT scanner (GE Medical Systems Milwaukee, Wisconsin) in a default planning position using the radiotherapy palette and head rest with their arms raised. The patient's breathing trace was tracked using the Varian RPM respiratory tracking system (Varian Medical Systems, Palo Alto, California). The patients were instructed to breathe freely for the duration of the scans. No breathing training or coaching was used. A contemporaneous low-dose chest 4D-CT acquisition was performed using 140 kVp energy photons at 10 mA and a slice thickness of 5 mm. After intravenous cannulization, approximately 40 MBq 68Ga-MAA was injected as a bolus. Immediately after administration of 68Ga-MAA, a 3D List-mode respiratory-gated PET scan was acquired over the chest (2 bed positions, 5 minutes per bed position, and slice thickness 3.27 mm). The field of view for both 4D-PET and 4D-CT encompassed the entire lung fields. This acquisition was subsequently reconstructed as both a gated (4D) and an ungated scan. Phase-matched attenuation correction with 5 and 10 respiratory bins was used to reconstruct the 4D-PET/CT scan. The free-breathing PET acquisition was subsequently coregistered with the average (AVG) intensity projection of the 4D CT for purposes of treatment planning as described previously, 20 with subsequent PET thresholding applied to the time-AVG 4D PET images.
Radiotherapy Treatment Planning
All patients were planned to receive 60 Gy in 30 fractions of radiotherapy using 3D conformal techniques. Radiotherapy planning scans were performed with patients positioned supine with both arms elevated above the head. A respiratory-sorted 4-dimensional computed tomography (4DCT) data set was generated using the Philips Brilliance (Koninklijke Philips Electronics, Amsterdam, the Netherlands) CT scanner coupled with a Philips Bellows system or a Varian RPM system. The 4DCT scans were acquired in helical mode and binned into 10 phases for image reconstruction. The patients were imaged using 140 kVp, 3-mm slice thickness, 3-mm increment, and 0.44-s rotation time, and images were reconstructed with ∼3.5-mm3 voxel resolution (3-mm slice thickness × 1.0742-mm pixel spacing). From the respiratory-sorted imaging phases, AVG and maximum intensity projection (MIP) series were reconstructed. Target delineation was performed on an Elekta FocalSim (Medical Intelligence, Schwabmünchen Germany) workstation. Standardized lung window/level settings (1700/−300) were used in the MIP image series. An internal target volume was delineated from the MIP series, and a further isotropic expansion of 5-mm was used to generate the clinical target volume (CTV) and a further 10-mm isotropic expansion from CTV was used to create the planning target volume (PTV). The lung organ at risk (OAR) was defined as the volume of both lungs minus the volume of the GTV. Treatment planning was performed on the Elekta CMS/XiO V4.4 planning system blinded to the findings of the perfusion PET/CT. Doses to OARs were calculated using the AVG series. Typically a 3- to 4-field radiotherapy technique using 6 MV photons was used with effort made to avoid the contralateral unaffected lung and spare spinal cord, while ensuring the PTV was within −5% and +7% of the prescribed dose, per International Committee on Radiation Units and Measurements (ICRU) 62 recommendations. Dose constraints to OARs dose were as follows: spinal canal ≤45 Gy, mean lung dose (MLD) ≤20 Gy, V5 ≤60%, V20 ≤35%, and V30 ≤30%.
Functional Avoidance Radiotherapy Planning
Functional avoidance radiotherapy planning was performed on a data set created from rigidly registering 4D-PET/CT scan with the 4DCT radiotherapy planning scan. All Digital Imaging and Communications in Medicine (DICOM) data sets were imported into the iPlan treatment planning system (v4.5, BrainLAB; Feldkirchen, Germany). A single nuclear medicine physician (MSH) and a single radiation oncologist (SS) contoured functional lung volumes defined as either “perfused” or “well-perfused” lung using a visually adapted threshold technique. The perfused lung volume was defined as any perfused lung parenchyma, as defined by lung tissue with 68Ga-MAA radiotracer uptake. The well-perfused lung was defined using an automated contour of lung parenchyma with a maximum standardized uptake value (SUVmax) threshold of 30% (ie, inclusion of the top 70% of voxels), which was then visually adjusted to exclude any central tracer clumping (Figure 1). Two functionally guided radiotherapy plans were then generated based on functional lung by a single radiotherapy planner (TD), a 3D conformal plan optimized to avoid perfused lung and a second 3D conformal plan optimized to avoid the well-perfused lung, respectively. Functional radiotherapy plans were limited to the use of the same or fewer numbers of beams as the original plan used for treatment. Dose volumetrics of the functional lung volumes (ie, calculating MLD and Vdose by excluding nonfunctioning lung) were compared to the “anatomical lung” volume as defined by the geometric lung OAR volume used for treatment. Each plan was optimized to the respective lung volume independently without being informed by the other available lung volumes.

Hybrid 68Ga-perfusion PET/CT imported into the iPlan planning system, demonstrating a patient with severe emphysema. Perfusion alone images is shown on the left panel, with coregistered PET/CT shown on the right panel. Anatomical (cyan contour), perfused lung (yellow contour), and well-perfused (red contour) lung volumes are displayed. A visually adapted standardized uptake value (SUV) thresholding technique was used to define well-perfused lung. PET/CT indicates positron emission tomography/computed tomography.
Statistical Analyses
The anatomical, perfused, and well-perfused lung volumes were compared using repeated measures analysis of variance. The following volumetric parameters were compared using Wilcoxon signed rank test: MLD, V5, V10, V20, V30, V40, V50, and V60. Median differences and their respective nonparametric confidence intervals were reported.
Results
Between December 2011 and September 2012, 14 consecutive patients with NSCLC were enrolled into this prospective study. The median (range) age of patients was 65 (47-90) years old. There were 5 patients with AJCC stage I disease, 1 patient with stage II disease, 7 patients with stage III disease, and 1 patient with stage IV disease (with resected brain metastasis). The most common tumor location was the RUL (n = 7). Patient characteristics and lung volumetrics are outlined in Table 1. The patient cohort consisted of exsmokers with preexisting airways disease, with a median (range) DLCO of 54% (27%-70%). The mean (95% CI) PTV volume was 400 cm3 (238-562 cm3). The mean volumes (95% CI) were 3722 cm3 (3016-4428 cm3), 3026 cm3 (2538-3514 cm3), and 1936 cm3 (1497-2376 cm3) for the anatomical, perfused, and well-perfused lung volumes, respectively. These volumes were significantly different on multiple comparison testing (P < .001). Figure 2A-D demonstrates a representative perfusion PET/CT in a patient with severe emphysema, the original plan used for treatment based on the anatomical lung, a plan optimized for perfused lung, and a plan optimized for well-perfused lung, respectively. All plans met the ICRU 62 dose prescription and target coverage goals.
Patient Characteristics.

Abbreviations: adenoCa, adenocarcinoma; DLCO, diffusing capacity of the lung for carbon monoxide; LUL, left upper lobe; LLL, left lower lobe; NSCLC/NOS, nonsmall cell lung cancer; PTV, planning target volume; RUL, right upper lobe; RLL, right lower lobe; SCC, squamous cell carcinoma; T, Tumour; N, Lymph Node; M, Metastasis.
aPatient with bulky bilateral mediastinal disease, no pulmonary parenchymal primary disease.
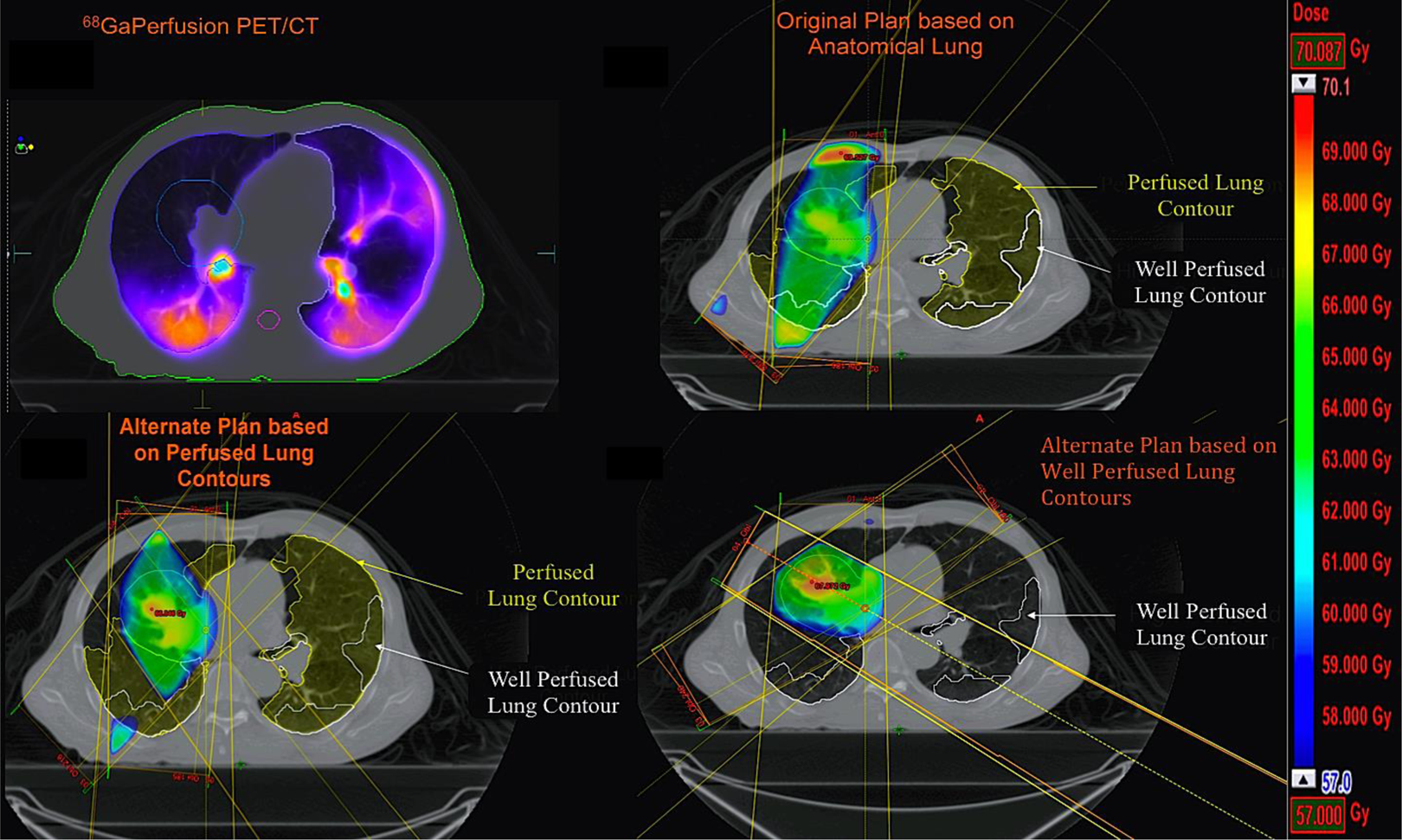
Demonstrates planning methodology used in study. A, Perfusion positron emission tomography (PET) showing the PTV contoured in cyan, (B) the plan used for treatment with “perfused” and “well-perfused” lung contours demonstrating avoidance of contralateral anatomical lung, (C) an alternate plan optimized to perfused lung contours, and (D) an alternate plan optimized to well-perfused lung contours.
Three-dimensional conformal lung planning optimized to avoid regions of functional lung resulted in improved dose volumetric outcomes to functioning lung. Conventional planning techniques blinded to the findings of the perfusion PET/CT resulted in minimal or no significant changes to the functional lung dose volumetrics (Table 2). When alternate plans were optimized to the perfused lung volume, the V60 dose volume parameter improved by a median of 1% to the functional lung; however, this was at the expense of a worse V5 dose volume parameter, at a median detriment of 3.33% (Table 3). When optimizing the plan to the well-perfused lung volume, the median dose was significantly reduced to the functional lung for the MLD, V30, V40, V50, and V60 dose volume parameters (Table 4).
Evaluation of the Conventional Plan Optimized for Anatomical Lung, Comparing Conventional Dose Volumetrics Versus “Perfused” Lung and “Well-Perfused” Lung Dose Volumetrics.a

Abbreviations: CI, confidence interval; DVH, dose–volume histogram.
aStatistically significant findings highlighted in bold. Differences were calculated on a per patient basis.
Comparison of the Conventional Plan Versus the Alternate Plan Optimized for “Perfused Lung,” Evaluating “Perfused Lung” Dose Volumetrics.a

Abbreviations: CI, confidence interval; DVH, dose–volume histogram.
aStatistically significant findings highlighted in bold. Differences were calculated on a per patient basis.
Comparison of the Conventional Plan Versus the Alternate Plan Optimized for “Well-Perfused” Lung, Evaluating “Well-Perfused Lung” Dose Volumetrics.a

Abbreviation: CI, confidence interval; DVH, dose–volume histogram.
aStatistically significant findings highlighted in bold. Differences were calculated on a per patient basis.
Discussion
In this study, we propose 4D-68Ga-perfusion PET/CT as a novel imaging modality to facilitate regional avoidance of functional lung during radiotherapy. We were able to demonstrate the significant benefits in functionally adaptive planning in terms of reduction in dose to functional lung. On visual evaluation, it was apparent that it was the distribution of perfusion across diseased lung that most influenced the capacity for functional lung avoidance, not the absolute size of perfused lung or the PTV. In this scenario, PET/CT has several inherent advantages in comparison to SPECT/CT imaging. The perfusion-PET/CT procedure image is acquired in a shorter time than a perfusion SPECT/CT scan, thus is more convenient for the patient, particularly in those with significant respiratory distress or discomfort related to their cancer or background lung disease. The PET/CT also yields images of higher quality due to superior counting sensitivity and resolution. The intrinsically quantitative nature of PET also facilitates more accurate estimates of perfused functional lung volume, particularly if acquired as a respiratory-gated (4D) study. Previous research by our group 19 and others 21,22 has validated 3D-68Ga-ventilation/perfusion PET/CT as an accurate imaging biomarker of pulmonary pathophysiology. Our experience with acquisition of 4D respiratory-gated PET imaging has been applied to further enhance the interpretation of perfusion PET/CT in the context of this study, through mitigation of respiratory-induced image artifact.
Loss of perfusion in response to radiotherapy has been previously documented through the use of older scintigraphic techniques. SPECT/CT imaging is an advance on planar V/Q scintigraphy that allows for in vivo assessment of regional lung perfusion. Post-irradiation, regional lung perfusion deficit is evident on SPECT imaging within 3 to 9 months after RT. 23,24 Lung perfusion seen in SPECT imaging is thought to be a surrogate for lung function based on phantom 25 and animal 26 experiments. The dose–effect relationship in perfused regions of lung appears consistent when detected by SPECT/CT in patients irradiated for lung cancer, breast cancer, and lymphoma. 27 A recent publication in NSCLC 28 found that the dose to perfused functional lung was a stronger predictor for toxicity (area under the curve [AUC] 0.76-0.98) than the dose to conventionally measured lung (AUC 0.62-0.86). However, SPECT/CT suffers from major limitations. The SPECT/CT is unable to account for subtle spatial and temporal changes in lung function, has poorer resolution than PET, and has limited capacity to account for breathing motion. Zhang et al, 29 the authors of the largest prospective series (spanning 14 years) of SPECT/CT, concluded that analysis of a dose–effect relationship in the lung using SPECT/CT was limited by inaccuracies including changes in patient anatomy over time and image registration errors from breathing. Given that the estimated radiation dose from perfusion PET to the patient is comparable to perfusion SPECT/CT scanning and lower than other blood flow assessments such as CT pulmonary angiography, 30 PET represents a logical new advance that may facilitate more accurate investigation of perfusion loss secondary to lung irradiation.
Selection of an appropriate threshold for what is considered functional lung is challenging in light of the variability in previously reported literature involving SPECT technology. It is further hampered by the lack of correlative validation with clinical outcomes of these previously reported functional lung volumes. There is presently no consensus in the optimal definition of what constitutes the functional perfused lung volume. As such our definitions of perfused were based on those used in previous studies, 14,15 and our definition of well-perfused lung was based on visual assessment and our own clinical experience suggesting that an SUVmax threshold of 30% (highest perfused 70%) represents a reproducible visual threshold defining apparent high functioning lung. A previous study of 16 patients by Shioyama et al using SPECT/CT 31 optimized lung plans on the 50th and 90th percentile of functional lung and showed that the mean functional lung dose could be reduced by 2.2 and 4.2 Gy, respectively. McGuire et al 32 used an iterative process to define the highest functioning lung in 5 patients and demonstrated that 4-beam intensity-modulated radiotherapy (IMRT) planned to avoid the highest functional lung could reduce the V20 and V30 to functional lung by a mean (±standard deviation) of 16.5% (±6.8%) and 6.1% (±9.2%), respectively, when compared to 9-beam conventional IMRT plans. However, a potential drawback of adaptively planning to only the highest 10% of perfused lung is the theoretical disadvantage of potential deposition of additional dose in regions of moderately perfused lung which may in fact contribute to the patient’s overall lung function.
On the other end of the spectrum, Christian et al 14 defined functional lung volumes by threshold adjusting the SPECT perfusion image to match the volumes defined on CT. This approach would incorporate a large proportion of total available lung and may account for why there was no significant improvement in dose to functional lung found in adaptive planning for 5 of the 6 patients. The mean difference between conventional and functional lung measurements in that study was 1012 cm3. In comparison with our study, the mean difference between conventional volumes versus the perfused volumes (incorporating all radiotracer uptake in lung) was 696 cm3. Similar to Christian et al, 14 our biologically adapted plans optimized to just the perfused lung volumes did not demonstrate significant improvements in dose to functional lung. However, adapting radiotherapy plans to the highest perfused 70% (30th centile) of lung in our study allowed a median reduction in MLD and V30 by 7.5% and 1.8%, respectively. This indicates that an appropriate selection of a threshold of lung perfusion may be necessary to demonstrate gains in functionally adaptive planning. Whether a selected threshold is clinically relevant is the subject of validation in future studies correlating clinical symptoms to functional dose volumetrics.
Conclusion
This is the first study incorporating the use of perfusion-PET in lung radiotherapy planning and demonstrating proof of principle that this technology can be used for functional lung avoidance. Our study demonstrated modest but statistically significant improvements in dose to functional lung volumes using functionally adapted radiotherapy plans without compromising target coverage. Importantly, this effect was only seen when adapting radiotherapy planning to the well-perfused areas of lung. In this study, an effort was made to constrain adaptive planning technique to be similar to the original technique used for treatment, using a 3D conformal technique with an equivalent number of beams as the original plan and avoidance of contralateral (functional) lung. Additionally, the study cohort consisted of a patient population with a modest MLD of 11.2 Gy. It may be that more advanced planning techniques, such as IMRT, volumetric modulated arc therapy, or incorporation of noncoplanar beams as is commonly employed in stereotactic radiotherapy, may allow for greater sparing of dose to functional lung. We suggest that further investigation into the use of 4D-68Ga-perfusion PET/CT in functional lung avoidance is warranted using both larger patient cohorts and alternative radiotherapy planning techniques.
Footnotes
Abbreviations
Acknowledgments
We thank the invaluable contribution of Mr Peter Eu, for provision of radiopharmaceuticals used in this trial, and Mr Daniel Pham for guidance in the radiotherapy planning aspects.
Authors’ Note
SS is the principal investigator, responsible for oversight of trial and writing of the article. TD, TK, NH, and JC were responsible for radiotherapy planning, functional volume creation and contributed to writing of the article. DLB, MPM, FF, NP, DS, and MS were responsible for study design, conduct of trial, recruitment of patients onto trial, and contributed to writing of the article. RJH and MH were responsible for interpretation of functional imaging, contributed to design of the study, and writing of the article. MB performed the statistical analysis of this study. Australian and New Zealand Clinical Trials Registry, ACTRN12613000061730 (Universal Trial Number U1111-1138-4421).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr Shankar Siva has received National Health and Medical Research Council scholarship funding for this research, APP1038399. This trial was partially supported a Priority-drive Collaborative Cancer Research Scheme 2013 grant (APP 1060919).