
Abstract
There is considerable practice variation in treatment of the node negative (N0) contralateral neck in patients with head and neck cancer. In this study, we examined the impact of N0 neck target delineation volume on radiation dose to the contralateral parotid gland. Following institutional review board approval, 12 patients with head and neck cancer were studied. All had indications for treatment of the N0 neck, such as midline base of tongue or soft palate extension or advanced ipsilateral nodal disease. The N0 neck volumes were created using the Radiation Therapy Oncology Group head and neck contouring atlas. The physician-drawn N0 neck clinical target volume (CTV) was expanded by 25% to 200% to generate volume variation, followed by a 3-mm planning target volume (PTV) expansion. Surrounding organs at risk were contoured and complete intensity-modulated radiation therapy plans were generated for each N0 volume expansion. The median N0 target volume drawn by the radiation oncologist measured 93 cm3 (range 71-145). Volumetric expansion of the N0 CTV by 25% to 200% increased the resultant mean dose to the contralateral parotid gland by 1.4 to 8.5 Gray (Gy). For example, a 4.1-mm increase in the N0 neck CTV translated to a 2.0-Gy dose increase to the parotid, 7.4 mm to a 4.5 Gy dose increase, and 12.5 mm to an 8.5 Gy dose increase, respectively. The treatment volume designated for the N0 neck has profound impact on resultant dose to the contralateral parotid gland. Variations of up to 15 mm are routine across physicians in target contouring, reflecting individual preference and training expertise. Depending on the availability of immobilization and image guidance techniques, experts commonly recommend 3 to 10 mm margin expansions to generate the PTV. Careful attention to the original volume of the N0 neck CTV, as well as expansion margins, is important in achieving effective contralateral gland sparing to reduce the resultant xerostomia and dysguesia that may ensue after radiotherapy.
Introduction
Despite the advent of intensity-modulated radiation therapy (IMRT), xerostomia remains a common toxicity following head and neck (H&N) radiation and a cause of decreased quality of life for many patients. 1 –4 Preservation of function of parotid and other salivary glands is important to limit xerostomia, dysguesia, dental decay, and dysphagia. The prevention of severe xerostomia is a trademark quality-of-life benefit for patients with H&N cancer treated with IMRT.
A series of studies have identified that mean radiation dose to the parotid gland is a good predictor of alteration in salivary flow. 5 –9 Comprehensive evaluation of the relationship between xerostomia and dose to the parotid gland requires precise delineation of organs at risk and dose–volume histogram analysis. Dose–response relationships have been determined using whole mouth 5,6 and parotid 10,11 salivary flow rates and salivary gland scintigraphy. 12,13 Early investigations by Eisbruch et al demonstrated a mean parotid salivary gland dose of <26 Gray (Gy) to significantly preserve salivary flow rates. 8,9 However, a more recent combinatorial analysis failed to identify a threshold dose but did establish a normal tissue complication probability (NTCP) curve for parotid gland function 1 year after radiotherapy. 14
Many studies indicate that IMRT enables normal tissue sparing, resulting in reduced xerostomia and improved well-being for patients with H&N cancer. 3,15,16 These conformal dose distributions, with corresponding sharp dose gradients, necessitate precise target definition and treatment delivery. Many patients with H&N cancer require bilateral neck irradiation due to gross nodal disease or high occult risk. In these patients, sparing of the contralateral parotid gland can be challenging, particularly if the planning target volume (PTV) expansion requires significant margins because daily image guidance and precision immobilization are not available. Furthermore, there is significant variation in target volume definition across clinicians. 17,18 The purpose of this study is to examine the impact of node negative (N0) neck target volume on radiation dose to the contralateral parotid gland designated for dose sparing with IMRT.
Materials and Methods
Following approval by the University of Wisconsin Carbone Cancer Center Institutional Review Board, 12 patients with an indication for radiation treatment of the contralateral N0 neck (primary tumor involving the base of tongue or soft palate, tumor approaching midline, or presence of significant ipsilateral nodal disease) were selected to study the impact of N0 nodal volume on radiation dose to the contralateral parotid gland. Patients with disease crossing midline were excluded because of the negative dosimetric impact of the primary clinical target volume (CTV) on dose to the contralateral parotid gland. The disease sites included tumors from the base of tongue, 5 tonsil, 4 supraglottic larynx, 2 and H&N of unknown primary. 1 All cases were treated with IMRT via tomotherapy. In preparation for therapy, all patients underwent a computed tomography simulation scan with head and shoulder mask immobilization.
Target volume delineation of the contralateral N0 neck volumes was created using parameters from the Radiation Therapy Oncology Group (RTOG) H&N contouring atlas. Target and avoidance structures were contoured using Philips Pinnacle3 version 9.0 treatment planning software. Based on N0 volume, the median, 25th, and 75th percentile patients were identified from the study group and used in the N0 expansion studies. The identified contralateral N0 nodal volumes were uniformly (isometrically) expanded by 25%, 50%, 75%, 100%, and 200% of the original volumes. Planning target volumes, to account for positional uncertainty, were constructed by applying a 3 mm uniform expansion to all 6 of the N0 nodal volumes. The organs at risk, including the brainstem, spinal cord, parotid gland, mandible, larynx, oral cavity, and optic structures, were contoured for treatment planning. Sets of residual planning volumes for the contralateral parotid gland were constructed excluding the PTVs to eliminate conflicting constraints from the optimization.
Planning was performed on Tomotherapy version 4.0.4 planning stations. Helical Tomotherapy plan parameters consisted of 2.5-cm field width and 0.287 pitch. The modulation factor is proportional to the maximum of the degree of intensity modulation in the plan. The optimal modulation factors were found to be 2.5 or less. Separate plans were generated for the 0%, 25%, 50%, 75%, 100%, and 200% N0 nodal volume expansions. The 50% N0 plan was used to develop a patient-specific protocol that was applied to each of the volume studies for 250 iterations. The resulting plans maintained the same degree of target coverage (and tumor control) and allowed the assessment of normal tissue dosimetry.
Results
Patient characteristics are detailed in Table 1. Twelve patients with indications for radiation therapy to the contralateral, N0 neck were chosen for the study based on either advanced T-stage or advanced ipsilateral nodal disease. Of the 12 patients, 9 had oropharynx primaries (5 base of tongue and 4 tonsil), 2 had supraglottic larynx cancer, and 1 had squamous cell cancer of the neck from unknown H&N primary site.
Patient Characteristics.

The mean N0 neck target volume drawn by the radiation oncologist for these 12 patients with H&N squamous cell carcinoma measured 93 cm 3 with a range of 71 to 145 cm 3 (Table 1) with an example shown in Figure 1. The patients at the 75th, 50th, and 25th percentiles (ranked third, sixth, and ninth) were then chosen for volumetric expansion and subsequent analysis. Volumetric expansion of the N0 neck CTV in 25%, 50%, 75%, 100%, and 200% increments led to a uniform expansion of the physician-drawn CTV by 2.2, 4.1, 5.8, 7.4, and 12.5 mm, respectively (Figure 2 and Table 2).

Clinical target volume delineation in the node negative (N0) neck depicting highly conformal N0 target and 25%, 50%, 100% (bold), and 200% volumetric expansions. Note, for example, that the 50% and 100% expansions reflect 4.1 and 7.4 mm expansions of the baseline N0 target contour. This range of variation is common across practitioners as is variation in clinical target volume (CTV) to planning target volume (PTV) expansions.

Progressive volumetric expansion of the clinical target volume (CTV) showing corresponding increase in the CTV margin in mm. For example, a 50% volume expansion of the node negative (N0) target corresponds with a 4.1 mm increase in the CTV margin.
Volumetric Expansion of CTV With Resultant Increase in Dose to Parotid.
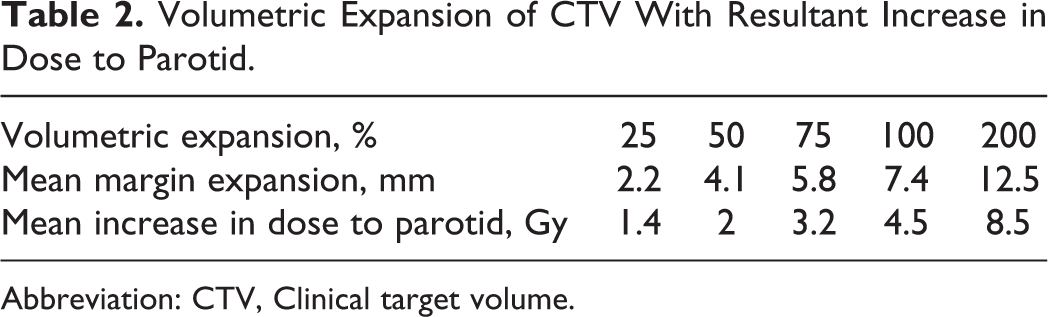
Abbreviation: CTV, Clinical target volume.
Volumetric expansion of the N0 neck CTV by 25%, 50%, 75%, 100%, and 200% (with subsequent 3 mm PTV expansion prior to IMRT planning) increased the resultant mean dose to the contralateral parotid gland designated for sparing by 1.4, 2.0, 3.2, 4.5, and 8.5 Gy, respectively (Figure 3 and Table 2).
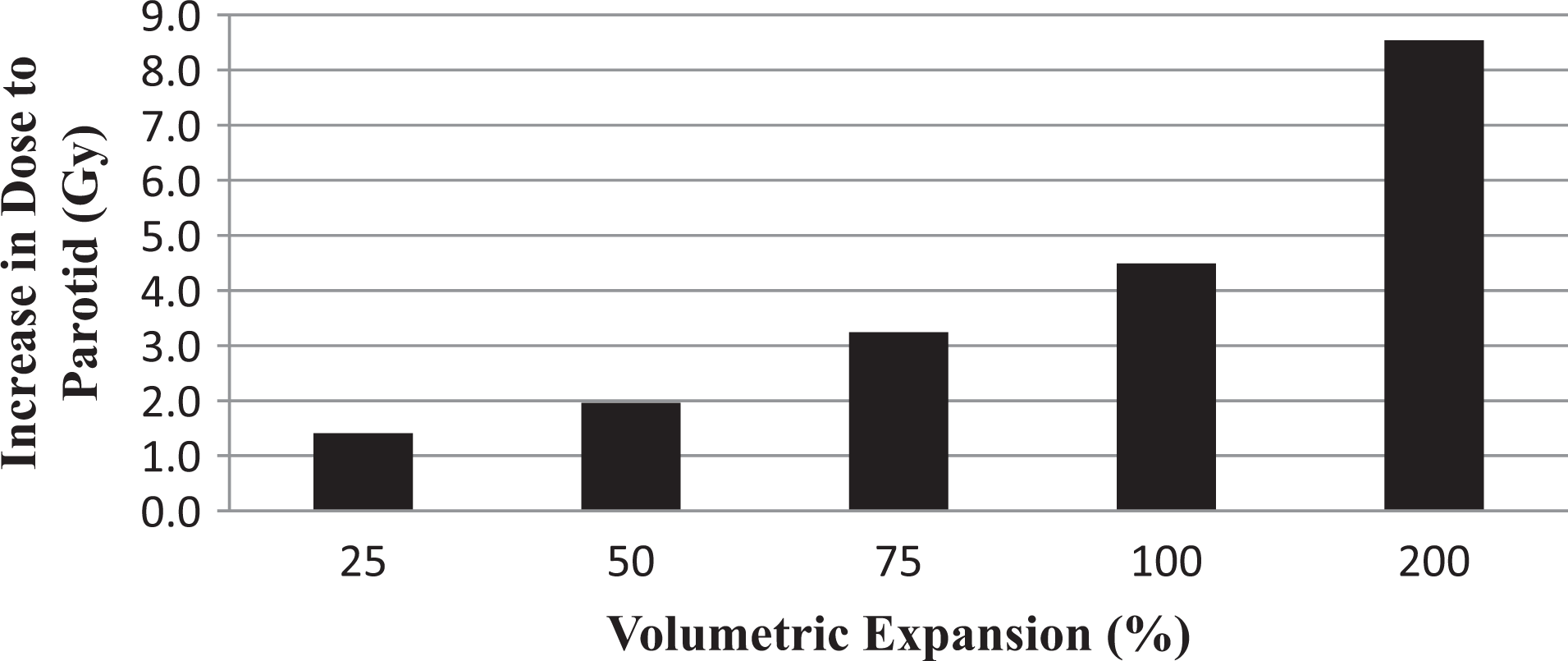
Incremental volumetric expansion of the node negative (N0) target contour with corresponding increase in dose to the parotid gland designated for sparing (contralateral to the primary tumor). For example, a 50% or 100% volume expansion of the N0 target translates to a 2.0 or 4.5 Gy increase in the parotid gland dose, respectively.
Discussion
This study demonstrates that the treatment volume designated by the radiation oncologist for the N0 neck can have profound impact on the resultant dose to a contralateral parotid gland designated for sparing. The importance of parotid sparing was demonstrated by Eisbruch et al 8 who found that decreasing overall dose to the parotid gland allowed for sparing of salivary flow, which subsequently showed improvement approximately 6 months after the therapy. More importantly, the degree of patient-reported xerostomia significantly correlated with the mean dose received by the major salivary glands and oral cavity (depicting impact on minor salivary glands). 8
A follow-up study from the University of Michigan demonstrated that the salivary output through 1 year after the completion of radiotherapy was directly related to the dose and irradiated volume of the parotid gland. 7 A threshold effect was observed such that parotid glands receiving less than 26 Gy demonstrated a time-related recovery, while most parotid glands receiving more than 26 Gy produced minimal salivary output and were less likely to recover over time. 7 Li et al further quantified the recovery of salivary function by demonstrating that after 2 years, salivary function recovered to ∼85% of baseline when the dose was <25 Gy when compared to only ∼30% of baseline when the dose was >40 Gy. 9 However, a more recent study has questioned the notion of a threshold dose and created an NTCP curve for modeling the effect of radiotherapy on parotid gland salivary function. 14
A recently published study by Beetz et al developed a predictive model for xerostomia at 6 months and found that radiation dose to the parotid gland was the most important predictor of patient-related xerostomia 6 months after the completion of chemoradiotherapy. 19 Furthermore, xerostomia and dysphagia have been shown to improve for up to 2 years after the completion of radiotherapy. 20 Taken together, these studies underscore the value of minimizing radiation dose to the contralateral parotid gland designated for sparing by accurate and conformal target volume delineation in the N0 neck.
Patterns of failure reports for patients with H&N cancer treated with radiation identify dominant recurrence incidence within or adjacent to gross tumor (gross tumor volume or high-risk CTV) with uncommon failure in the N0 neck. Acknowledging the considerable variation that exists among radiation oncologists in target contouring, this low risk of failure in the N0 neck should provide some degree of confidence for tight volume definitions per the RTOG atlas. Classification of the recurrence type in H&N cancer commonly follows the description by Chao et al 21 : if 20% to 95% of the volume of recurrence was within the CTV, the failure is considered to be marginal. If >95% of the recurrence is within the CTV, the failure is considered to be in field, and if <20% of the recurrence is in the CTV, the failure is deemed out of field. Even with this liberal definition, the rates of marginal miss reported in series from the University of Michigan, University of Florida, Washington University, and University of California, San Francisco were only 3%, 2%, 2% and 0%. 21 –24 Although the probability of a marginal miss is low, there remains value for meticulous target delineation to minimize toxicities without compromising oncologic outcome. Overall, the low rates of failure in the N0 neck should serve as reassurance for the safety of drawing confined target volumes in the N0 neck as a means to limit dose to the contralateral parotid gland.
Limitations of this study include the retrospective nature of the work and the small sample size. Although 60 comprehensive IMRT treatment plans were run and analyzed following a series of volume expansions for this study, there is no substitute for prospective evaluation. A clinical trial that prospectively allocates patients to receive different target volumes for the N0 negative neck is under consideration at our center. This would also allow the inclusion of objective salivary flow measurement and patient-driven quality-of-life analysis to assess the ultimate impact of these dosimetric manipulations on ultimate outcome for patients with H&N cancer.
In conclusion, the treatment volume designated by the radiation oncologist for the N0 neck can have profound impact on resultant dose to the contralateral parotid gland designated for sparing in patients with H&N cancer. The finding from this study that a 4.1-, 7.4-, or 12.5-mm margin increase in the physician-drawn CTV translates into a 2.0-, 4.5-, or 8.5-Gy dose increase, respectively, to the contralateral parotid gland is notable. Depending on the availability of precision immobilization and image guidance techniques, experts commonly recommend 3 to 10 mm margin expansions of H&N target volumes. Careful attention to the original volume of the N0 neck CTV, as well as expansion margins, is important in achieving effective parotid gland sparing if this is considered a central treatment objective.
Footnotes
Abbreviations
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.