
Abstract
Introduction
Radiation-induced heart injury (RIHI) remains an important concern in left-sided postmastectomy radiotherapy (PMRT), particularly when internal mammary lymph nodes (IMLNs) are included in the target volume. Helical tomotherapy (HT) provides excellent target conformity for complex targets, but cardiac sparing remains challenging. This study evaluated whether dose-gradient function (DGF)-guided optimization could further reduce cardiac exposure in left-sided breast cancer patients treated with HT after modified radical mastectomy.
Methods
Twenty-six female patients with left-sided breast cancer who underwent PMRT were retrospectively included. Initial HT plan was generated and evaluated using DGF, which quantifies dose falloff outside the target volume. The patient with the minimum DGF curve area (
Results
DGF-guided re-optimization significantly reduced cardiac dose parameters while maintaining target coverage and overall plan quality. MHD decreased from 6.190 ± 0.384 Gy to 5.322 ± 0.332 Gy (P < 0.001), and cardiac
Conclusion
DGF-guided optimization may improve HT plan quality for left-sided PMRT and achieve additional reductions in cardiac dose and model-based cardiac risk estimates, particularly in cases requiring IMLNs irradiation.
Keywords
Introduction
Breast cancer is the most prevalent cancer among women worldwide and a leading cause of female mortality. 1 Postoperative adjuvant radiotherapy is crucial to breast cancer management, reducing recurrence, metastasis, and death. Unlike radiotherapy after breast-conserving surgery (BCS) for left-sided cancer, postmastectomy radiotherapy (PMRT) positions the cardiac and left anterior descending coronary artery (LAD) within a steep dose gradient region, particularly when the internal mammary lymph nodes (IMLNs) are targeted. Consequently, the risk of radiation-induced heart injury (RIHI) rises substantially with increasing exposure.2,3 Electing to irradiate the IMLNs creates a significant dosimetric challenge for radiotherapy planning. Even without deliberate targeting, incidental irradiation can deliver approximately 40-60% of the prescribed dose (e.g., 25-30 Gy mean dose from a 50 Gy prescription). However, deliberately including the IMLNs within the clinical target volume (CTV) inevitably raises radiation exposure for adjacent critical organs, especially the heart and lungs.4,5 Clinical evidence consistently demonstrates that IMLNs irradiation increases cardiac dose. For left-sided breast cancer, the mean heart dose (MHD) rises from approximately 3.3 Gy without IMLNs irradiation, to 4.6 Gy with incidental exposure, and further to nearly 6.9 Gy when IMLNs are formally included in the planning target volume (PTV). 6 Given the established linear relationship between MHD and the risk of major coronary events, even a moderate increase in MHD may translate into a clinically significant rise in long-term cardiac morbidity and mortality.7,8
Therefore, a central challenge in PMRT for left-sided breast cancer is achieving adequate target coverage of the chest wall and regional lymph nodes while minimizing radiation exposure to the heart. Helical Tomotherapy (HT) enables integrated irradiation of the chest wall and regional lymph nodes (including IMLNs) through its continuous helical irradiation and intensity-modulated capabilities, making it suitable for treating extensive and complex target volumes in PMRT. Due to frequent extension of the PMRT target volume into the supraclavicular region and IMLNs, conventional techniques often encounter difficulties with field matching and exhibit dose irregularities. HT, however, provides longitudinal continuous coverage through a single plan, improving dose uniformity within the target and reducing hot and cold spots. 9 Cardiac sparing is particularly challenging in left-sided PMRT, especially when irradiation of the IMLNs is required. Although HT can provide excellent target coverage for complex target volumes, it may also increase low-dose exposure to surrounding normal tissues. For patients with left-sided breast cancer, the IMLNs target volume is closely related to the anatomy of the heart and LAD, making cardiac dose control a core dosimetric objective in PMRT planning. Epidemiological evidence has demonstrated a linear association between MHD and the incidence of ischemic cardiac disease, further underscoring the importance of minimizing cardiac radiation exposure. 8 On this basis, HT combined with directional or complete blocking strategies can reduce moderate-to-high dose exposure to organs at risk (OARs), such as the heart (specifically the left anterior descending artery) and the lungs, while maintaining good target coverage and conformal quality for the chest wall and regional lymph nodes (including the IMLNs). 10
Traditional planning evaluation metrics, including dose-volume histogram (DVH), conformity index (CI), and homogeneity index (HI), are widely used to assess target volume coverage and dose uniformity, but do not directly quantify the three-dimensional spatial dose gradient.11,12 In contemporary radiation therapy planning, parameters derived from DVH are not only used for post-planning evaluation but are also routinely used to guide iterative plan optimization and quality assurance, particularly in breast cancer radiotherapy.13,14 Although various indices based on conformation and distance have been proposed to indirectly reflect dose distribution characteristics, their ability to describe the spatial rate of dose falloff around complex target regions remains limited.15,16 To address this, gradient-based metrics have been introduced. Paddick et al proposed a dose gradient index (DGI) to complement conformity assessment. 17 More recently, Sung et al introduced the dose gradient curve (DGC), providing a quantitative description of dose decay as a function of distance from the target volume. 18 Building upon this concept, spatial dose gradients have been widely used to describe dose falloff outside the PTV and to evaluate plan quality in various radiotherapy techniques.19,20 Specifically, the dose-gradient function (DGF) has been applied as a quantitative metric to guide plan optimization and reduce radiation-induced lung injury in breast cancer radiotherapy. 21 However, the clinical applicability of DGF-guided optimization in HT-based PMRT, particularly for patients requiring IMLNs irradiation, remains unclear. 22 Therefore, this study aimed to evaluate whether DGF-guided optimization could improve dosimetric plan quality and reduce cardiac exposure in HT-based PMRT for left-sided breast cancer after modified radical mastectomy, and to explore its potential impact on model-based cardiac risk estimates.
Materials and Methods
Patient Selection
A total of 26 female patients with left-sided breast cancer who underwent PMRT at our institution between April 27, 2021, and July 17, 2023 were retrospectively screened according to predefined eligibility criteria. Patients who met the inclusion criteria and had complete clinical, target delineation, and dosimetric data available for analysis were included in the study. The mean patient age was 52 years (range 34-72 years). Seventeen patients received IMLNs irradiation, while nine did not.
This retrospective study was approved by the Ethics Committee of Yunnan Cancer Hospital, The Third Affiliated Hospital of Kunming Medical University, Peking University Cancer Hospital Yunnan (approval No. KYLX2024-285; approved on November 20, 2024). Written informed consent was obtained from all participants. All patient information was de-identified prior to analysis. The study was conducted in accordance with the Helsinki Declaration of 1975, as revised in 2024.
Target Volume Delineation
The CTV was delineated by an experienced radiation oncologist according to the Radiation Therapy Oncology Group (RTOG) guidelines for modified radical mastectomy in breast cancer. The PTV was generated by adding 0.5 cm to the isotropic CTV, excluding any portions extending into the lung or beyond the skin surface. OARs included the heart, left lung, right lung, combined lungs, right breast, spinal cord, left humeral head and LAD. LAD delineation followed the method described by Memorial Sloan Kettering Cancer Centre, in which the anterior cardiac region was defined as the superficial 1 cm volume of the left anterior quadrant of the heart. 23
IMLNs irradiation was indicated based on the following criteria: (1) ≥4 positive axillary lymph nodes after dissection; (2) Inner-quadrant or central primary tumour with axillary lymph node metastases; (3) Age < 35 years with axillary lymph node metastases; (4) Radiologic evidence of IMLNs involvement at diagnosis or pathological confirmation in the absence of axillary lymph node dissection.
Treatment Planning
All treatment plans were generated using the Precision™ treatment planning system (TPS) on the Radixact® X system (Accuray Inc., Sunnyvale, CA, USA). Dose calculations utilized a convolution-superposition algorithm. All plans utilized a fixed beam width of 2.5 cm, a pitch of 0.4, and a modulation factor of 3.5. The initial plan was optimized using the institution’s standard planning template, without applying full-field or organ-based targeted blocking techniques. The optimization objectives prioritized PTV coverage, followed by cardiac and pulmonary protection. Relative weights were iteratively adjusted until all clinical requirements were met. Optimization was conducted using the iterative algorithm within the Precision™ TPS, running for approximately 3000 iterations.
Prescription dose was 50Gy in 25 fractions (2Gy per fraction), with a requirement for ≥95% PTV coverage. Critical organ dose constraints followed our institutional criteria: cardiac (
Dose-Gradient Function (DGF)
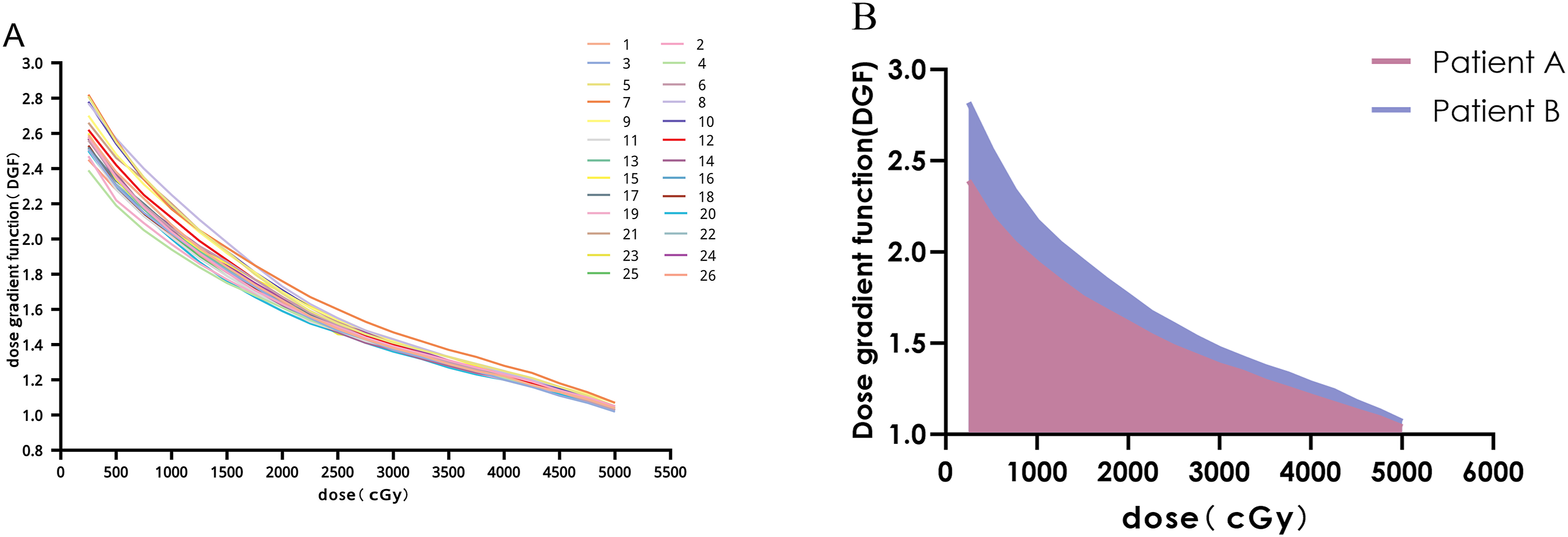
A fast dose decay rate outside the target volume is a desirable plan feature, as it reduces radiation exposure to surrounding normal tissues. To quantify this rate, Li et al proposed the DGF, which enables the assessment of dose distribution characteristics for plan evaluation and re-optimization.
21
It is defined as follows: Workflow of DGF-guided plan evaluation and re-optimization. (A) DGF curves for all 26 patients; (B) Illustration of the area under the DGF curve (

Mechanisms of DGF-Guided Radiotherapy Plan Optimization
Geometrical Parameters and DGF Curve Areas for 26 Patients

Estimated Relative Risk Increase (RRI)
RIHI was estimated using the linear dose-response relationship reported by Darby et al, which demonstrated a 7.4% increase in the relative risk of major coronary events per 1 Gy increase in MHD.
8
The RRI of major coronary events was estimated according to the Darby dose-response model based on MHD. Accordingly, the RRI was calculated as:
This provides a model-based estimation and does not represent actual observed clinical outcomes.
Evaluation Parameters
To assess dosimetric differences between original and optimized plans, DVH parameters were extracted for all targets and OARs. Heart dosimetry parameters included MHD and
Statistics
Statistical analyses were performed using IBM SPSS Statistics (Version 27). Paired t-tests were used to compare dosimetric differences between the original and optimized plans. Pearson correlation and simple linear regression analyses were used to assess the associations between the DGF curve area (
Reporting Guideline
The reporting of this study was prepared with reference to the STARD 2015 statement, where applicable, together with relevant EQUATOR reporting guidance for observational dosimetric studies. 24
Results
Plan Quality and Target Coverage
Comparison of Dosimetric Parameters Between the Original and DGF-Guided Optimized Plans in the 25 Patients Who Underwent Re-Optimization
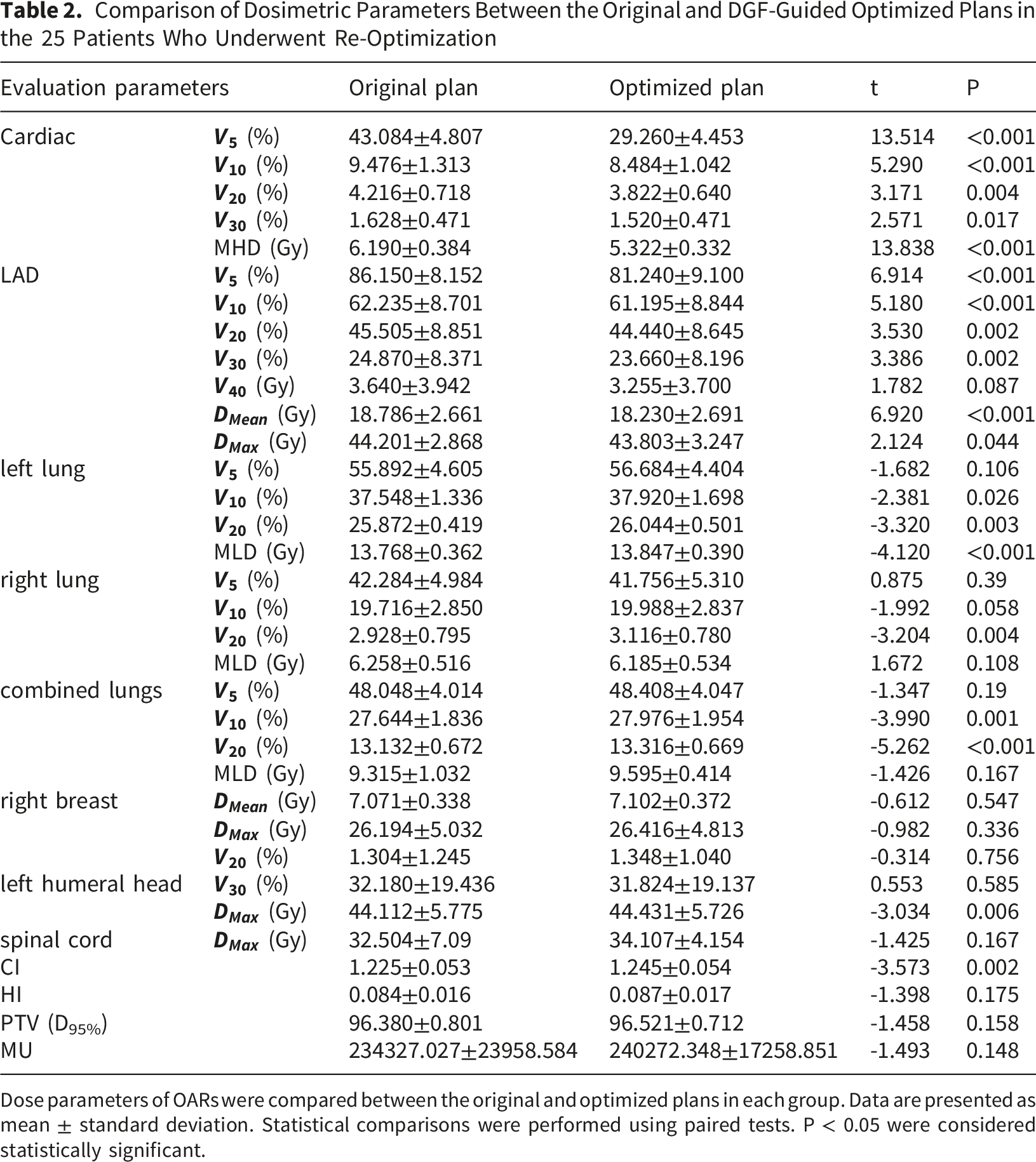
Dose parameters of OARs were compared between the original and optimized plans in each group. Data are presented as mean ± standard deviation. Statistical comparisons were performed using paired tests. P < 0.05 were considered statistically significant.
Comparison of Dosimetric Parameters Between the Original and Optimized Plans in the Non-irradiated and Irradiated IMLNs Groups
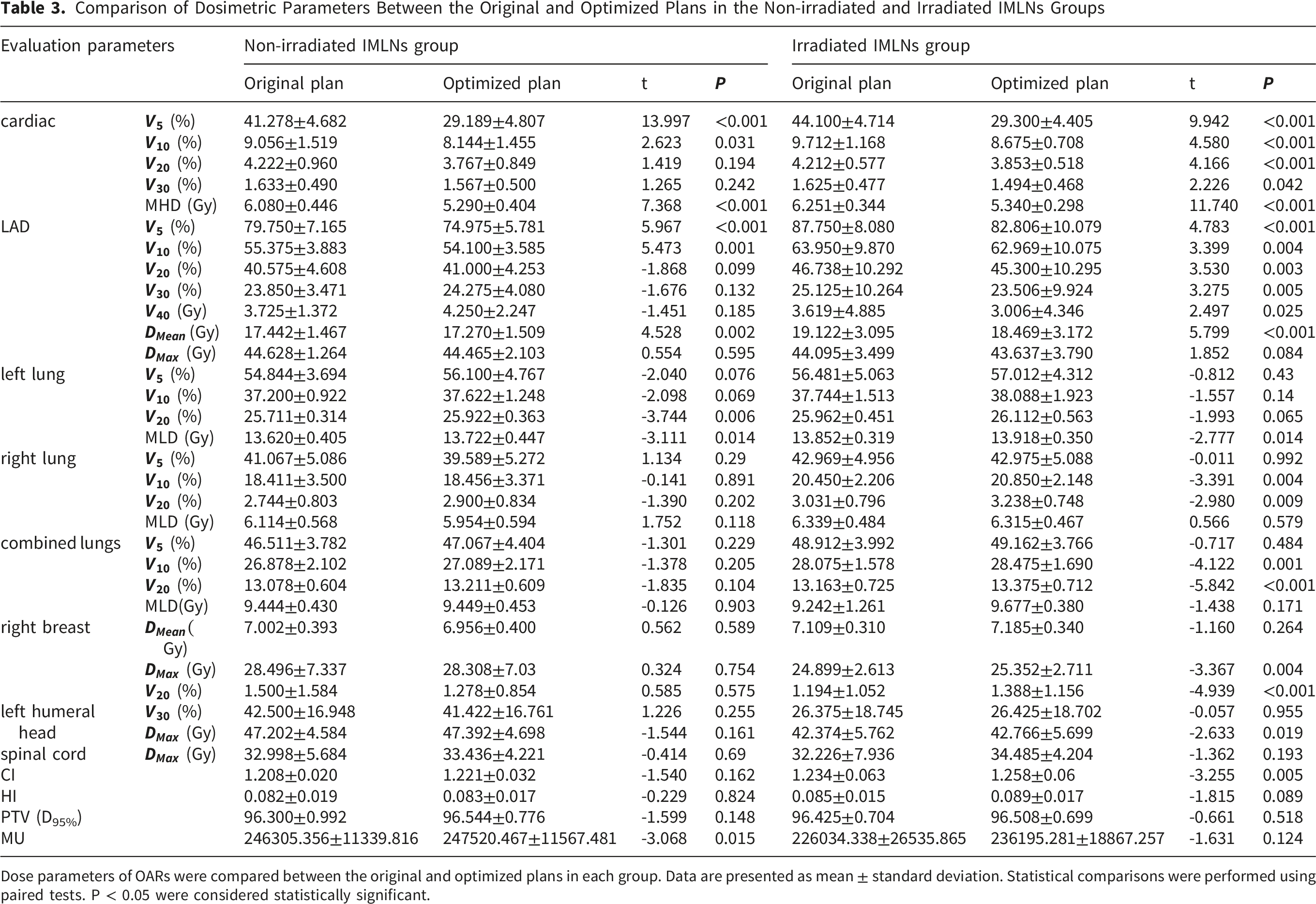
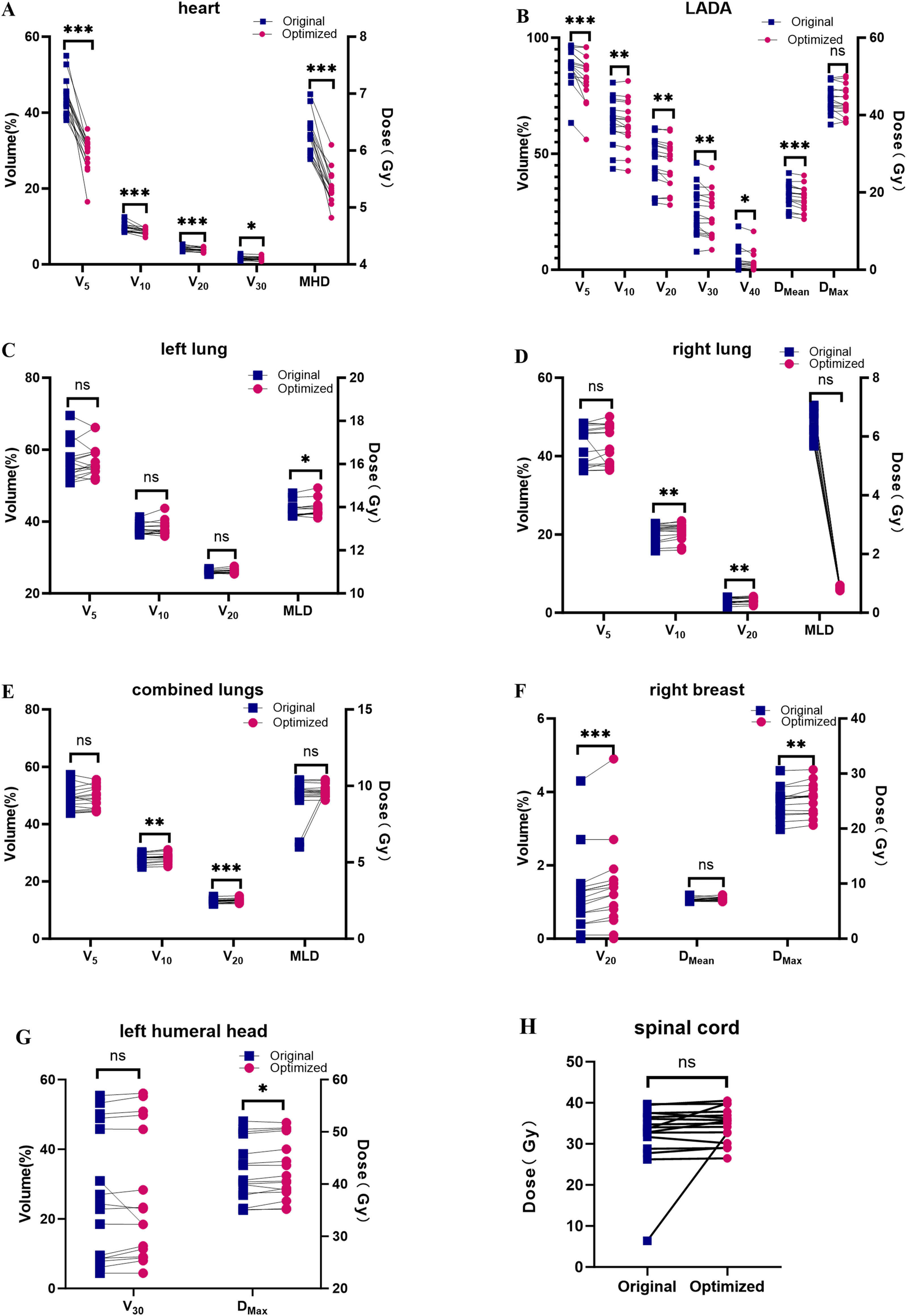
Dose parameters of OARs were compared between the original and optimized plans in each group. Data are presented as mean ± standard deviation. Statistical comparisons were performed using paired tests. P < 0.05 were considered statistically significant.
Heart and LAD Dose Parameters
For all patients, DGF-guided optimization significantly reduced cardiac dose parameters (Table 2). MHD decreased from 6.190 ± 0.384 Gy to 5.322 ± 0.332 Gy (P < 0.001). Significant reductions were also observed in cardiac
Subgroup analyses were summarized in Table 3 and illustrated in Figures 4 and 5. In the non-irradiated IMLNs group, significant reductions were observed in cardiac
Other OARs
Changes in dose to other OARs were generally small after optimization (Table 2 and Figure 3). For all patients, left lung Comparison of dosimetric parameters between the original and optimized plans in 25 patients who underwent re-optimization. Dose parameters of the cardiac (A); LAD (B); left lung (C); right lung (D); combined lungs (E); right breast (F); left humeral head (G); and spinal cord (H) are shown.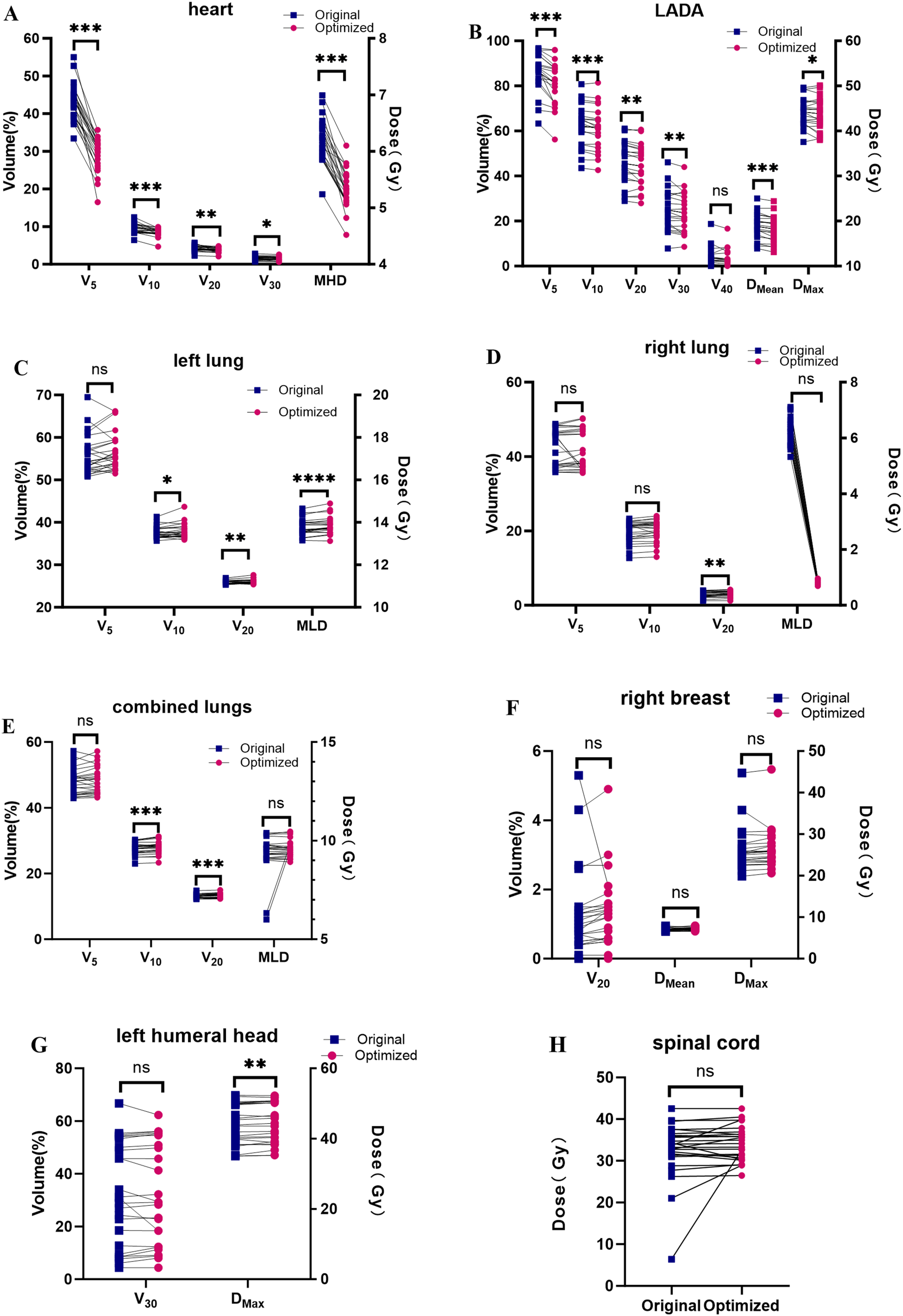
Subgroup analyses showed similar trends (Table 3), with minor yet statistically significant increases in some lung dose parameters, though clinically acceptable. Doses to the right breast and spinal cord remained stable. These trends are consistently illustrated in Figures 4 and 5. Comparison of dosimetric parameters between the original and optimized plans in the non-irradiated IMLNs group. Dose parameters of the cardiac (A); LAD (B); left lung (C); right lung (D); combined lungs (E); right breast (F); left humeral head (G); and spinal cord (H) are shown. Comparison of dosimetric parameters between the original and optimized plans in the irradiated IMLNs group. Dose parameters of the cardiac (A); LAD (B); left lung (C); right lung (D); combined lungs (E); right breast (F); left humeral head (G); and spinal cord (H) are shown.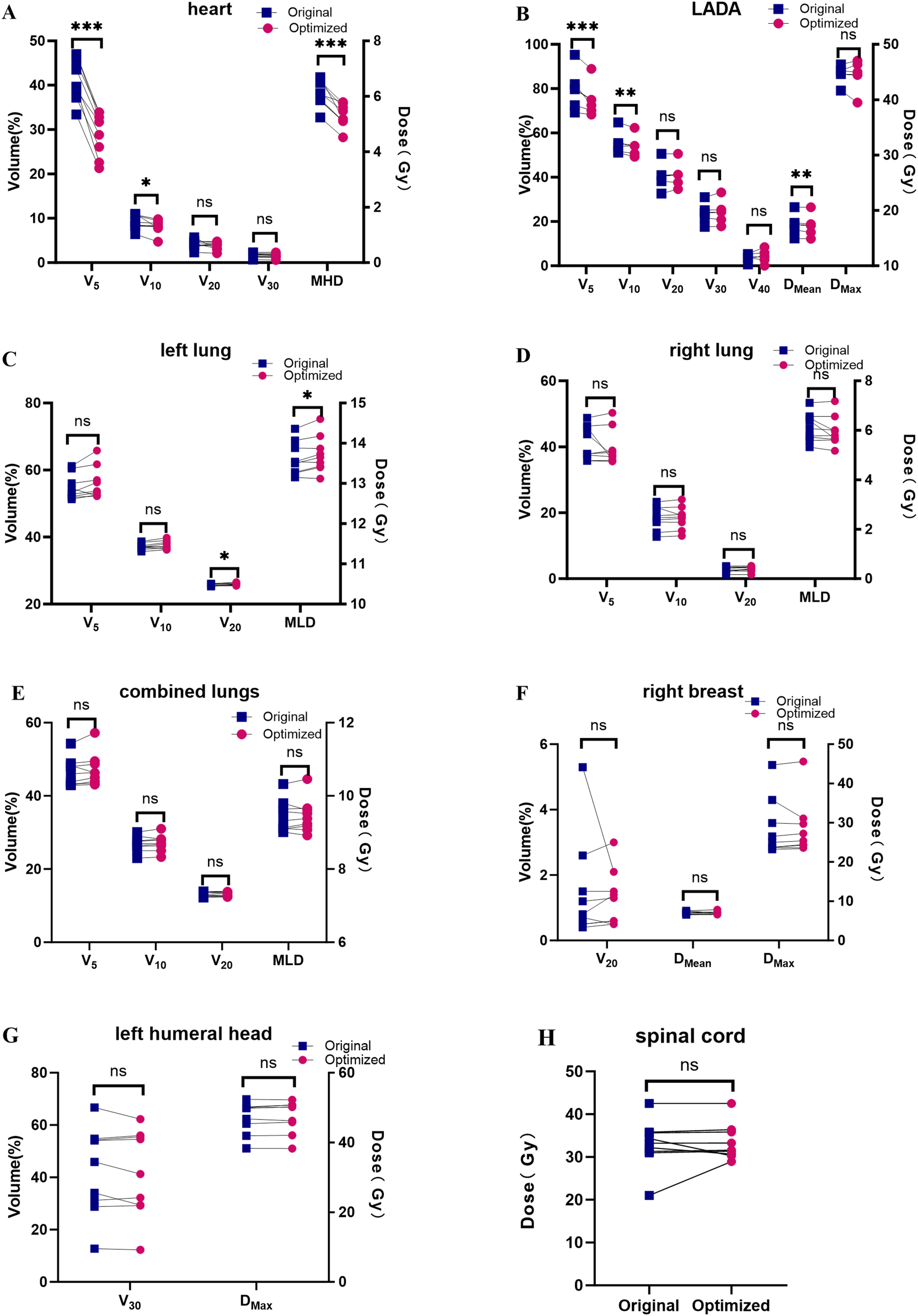
Estimated RRI of Cardiac Events
Estimated RRI of Major Coronary Events Before and After Optimization

RRI was calculated based on the Darby dose–response model, assuming a 7.4% relative increase in cardiac event risk per 1 Gy increase in MHD.
Association Between DGF Curve Area and Cardiac Dose Metrics
No significant association was observed between
Discussion
HT integrates computed tomography (CT) and linear accelerator technology, enabling efficient 360° rotational thin-layer irradiation and facilitating conformal treatment of large or anatomically complex targets adjacent to critical organs. Compared with conventional intensity-modulated radiation therapy (IMRT), HT may provide improved dose distribution and target conformality in selected complex target settings.25,26 For left-sided breast cancer, particularly following modified radical mastectomy, HT enables conformal dose delivery to the chest wall and regional lymph nodes, making it a useful technique for complex target coverage. With continued improvements in breast cancer survival, RIHI has emerged as a major long-term source of non-cancer morbidity and mortality, particularly after left-sided irradiation.
27
A systematic review indicated that the MHD in left-sided breast cancer patients receiving IMLNs irradiation was 8.4 Gy, approximately twice that of patients without IMLNs irradiation.
27
A retrospective study found that the cumulative incidence of ischemic cardiac disease in breast cancer patients irradiated to the IMLNs was 11.3% in those with cardiovascular risk factors and 6.4% in those without such risk factors.
28
A study of 55,000 breast cancer patients showed that left-sided patients had a 1.1-fold higher risk of cardiac death 10 years after radiotherapy than those with right-sided breast cancer.
29
Collectively, these findings underscore the critical need to minimize cardiac exposure, particularly when the IMLNs are included in the target volume. In the present study, DGF-guided re-optimization significantly reduced cardiac and LAD dose parameters compared with the original HT plans, with more pronounced reductions observed in the IMLNs irradiated subgroup. These results suggest that even within the inherently conformal framework of HT, DGF-guided optimization may achieve further cardiac sparing, thereby reducing model-based cardiac risk estimates without compromising target coverage. The significant cardiac dose reductions (IMLNs group:
While HT can provide favorable target conformity and normal tissue sparing, achieving a high-quality radiotherapy plan remains crucial for optimal therapeutic outcomes. Current plan evaluation methodologies have inherent limitations, because traditional metrics such as DVH parameters, CI, and HI provide valuable but incomplete information regarding the spatial characteristics of dose falloff.13,14 The gradient index (GI) proposed by Paddick et al is widely used but remains dependent on target volume and geometry.
17
Sung et al introduced the DGI to estimate average distances between isodose surfaces, while DGC and related gradient-based methods further extended this concept for plan evaluation and quality enhancement.16,18 However, these approaches still primarily rely on planar distance relationships and are insufficient for fully characterizing three-dimensional dose distributions. Building on this concept, Li et al proposed the DGF based on the overlapping volume histogram (OVH).
21
Unlike conventional DVH or conformity-based metrics, DGF provides additional spatial information on dose falloff outside the target volume, which is particularly relevant for cardiac sparing in left-sided PMRT. DGF quantifies the three-dimensional spatial relationship between the target and surrounding structures by reflecting the radius ratio of an “equivalent sphere.” Closer isodose surfaces to the target correspond to a steeper dose gradient and faster dose attenuation, and a smaller area under the DGF curve indicates a more favorable dose falloff. This provides the theoretical basis for using the area under the DGF curve as an empirical internal benchmark to guide plan optimization, particularly in cases involving IMLNs irradiation. Specifically, we hypothesized that these principles could also apply to the complex three-dimensional relationship between the heart, as a major OAR, and the target volume in left-sided PMRT. In this study, we constructed DGF curves for the heart and used the minimum area under the curve (
Previous studies have shown a linear relationship between MHD and the risk of major coronary events, and higher cardiac dose exposure has been associated with increased cardiac risk.2,3,8,30 The spatial distribution of coronary artery stenosis has been shown to correlate with high-dose regions, especially those involving the LAD and IMLNs areas.31-33 Clinically, cardiac dose constraints emphasize minimizing MHD; for example, the RTOG 1304 protocol recommends an MHD of <4 Gy to reduce cardiac exposure. Accordingly, MHD and cardiac Comparison of cardiac 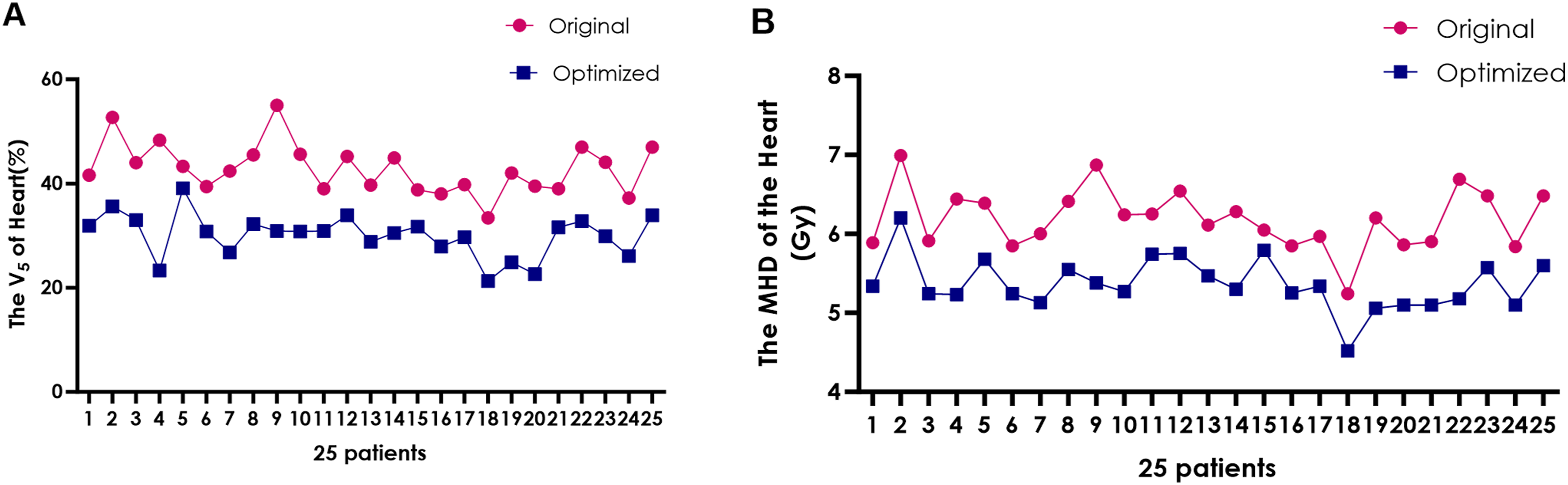
Importantly, DGF is not intended to replace existing HT planning strategies (e.g., complete/organ-based directional blocks, constrained blocks, gantry angle restrictions) but rather to serve as a complementary quantitative tool for characterizing three-dimensional dose gradients. In this study, all original plans were generated according to standard HT practice, and DGF-guided re-optimization was subsequently performed under the same clinical constraints. DGF was then used as an empirical internal benchmark for re-optimization without altering beam geometry or clinical constraints, thereby enabling additional cardiac sparing through intensity redistribution within existing constraints. In this context, DGF should be viewed not as a competing replacement for established cardiac-sparing techniques, but as an additional quantitative planning aid that may complement existing optimization strategies. The observed reduction in cardiac dose, particularly in cases involving IMLNs irradiation, suggests that DGF may provide additional benefit even when established HT optimization techniques are already used. Additionally, several advanced techniques, including proton therapy, respiratory gating, and active breathing control, have been shown to mitigate cardiac exposure.34-39 Combining DGF-guided optimization with motion management or geometric displacement techniques may further enhance cardiac protection by increasing the effective distance between the heart and the target volume. Such integrated strategies warrant further investigation. In the present workflow, DGF calculation required extraction of isodose volumes and external computation of the curve area, which added workload to the planning process. Although this process was not fully automated in the current study, future TPS scripting or other automated data-processing tools may improve clinical efficiency and reduce the additional workload associated with DGF-guided optimization.
This study has several limitations. First, it was a retrospective single-center study with a relatively small sample size, particularly in subgroup analyses. Second,
Conclusion
This study suggests that DGF-guided optimization complementing standard constraint-based approaches may improve HT plan quality for PMRT in left-sided breast cancer and achieve additional reductions in cardiac dose and model-based cardiac risk estimates. Particularly for complex target volumes requiring IMLNs irradiation, DGF-guided optimization in HT may offer further dosimetric advantages beyond conventional optimization.
Footnotes
Acknowledgments
The authors used generative artificial intelligence only for English language editing and readability improvement. All scientific content, data analysis, interpretation, and conclusions were developed and verified by the authors.
Ethical Considerations
This retrospective study was approved by the Ethics Committee of Yunnan Cancer Hospital, The Third Affiliated Hospital of Kunming Medical University, Peking University Cancer Hospital Yunnan (approval No. KYLX2024-285; approved on November 20, 2024).
Consent to Participate
Written informed consent to participate was obtained from all participants.
Consent for Publication
Not applicable, as no identifiable personal data are included in this study.
Author Contributions
Conception and design: Yunyan Yang and Xiang Pan.
Development of methodology and model: Han Bai and Ya Li.
Acquisition of data: Yunyan Yang; Jinli Peng and Tianwen Zhang.
Analysis and interpretation of data: Yunyan Yang and Yan Xu.
Writing, review, and revision of the manuscript: Yunyan Yang; Xiang Pan and Lingli Zhou.
Administrative, technical, or material support: Xiang Pan; Lingli Zhou; Han Bai and Ya Li.
All authors read and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Yunnan Provincial Department of Science and Technology-Kunming Medical University Joint Special Project for Applied Basic Research (No. 202201AY070001-161) and the Kunming Medical University Graduate Education Innovation Project (No. 2025S273).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are not publicly available due to patient privacy and institutional restrictions, but are available from the corresponding author upon reasonable request and with permission from the institution.