
Abstract
Introduction
Halcyon™ O-ring linear accelerators (linacs) provide a robust and efficient radiotherapy option for clinics. Interest in volumetric arc therapy (VMAT) based total body irradiation (TBI) has grown, with most current VMAT TBI protocols employing C-arm linacs; however, the feasibility of Halcyon-based VMAT TBI has been recently hypothesized. This study investigates the planning feasibility and dosimetric quality of VMAT-based, lung-sparing TBI delivered by Halcyon linac to pediatric patients.
Methods
10 pediatric patients (94 – 134 cm in height) previously treated to 12 Gy TBI through traditional 3D planning techniques were retrospectively replanned on a Halcyon linac. 2-3 VMAT plans containing 4-6 isocenters each with 2-2.5 arcs were created to treat the head, abdomen, and legs, with 1-2 static-gantry treatment matching areas being used between VMAT planning regions.
Results
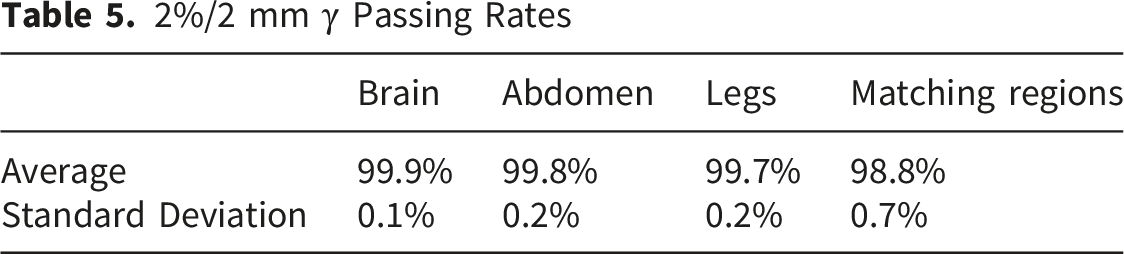
Lung doses were significantly reduced below the clinically significant level of 8 Gy, achieving mean doses of 6.66 ± 0.52 Gy (55.5% ± 4.3%). Target coverage was achieved with D90% of 77.5% ± 12.5% and homogeneity indexes of 0.92 ± 0.1. Planning time took 5-6 hours per patient: 1.5 hours for contouring and field placement and 3.5-4.5 hours for plan optimization and dose calculations. Using a dose rate of 800 MU/min field delivery time took an average of 20.8 ± 7 minutes with average portal dosimetry quality assurance passing rates of 99.6% and 99.9% for 2%/2mm and 3%/3mm gamma analysis metrics.
Conclusion
VMAT lung sparing TBI via Halcyon linacs is feasible and dosimetrically acceptable, with greatest applicability to smaller patients (<100 cm). Planning and setup complexity increases dramatically for larger patients (>100 cm) due to the smaller maximum field sizes (28 x 28 cm2) achievable. Future developments in software-based automations for target delineation, multiple field matching, and plan optimization could allow for more practicable treatment of larger patients.
Keywords
Introduction
Total body irradiation (TBI) is a frequently used component of conditioning regimens for allogeneic hematopoietic stem cell transplant (HSCT) used in the treatment of hematologic malignancies including leukemia, lymphoma, and multiple myeloma.1,2 TBI is employed to eradicate malignant cells and provide host immunosuppression for donor cell engraftment. The treatment process for TBI poses a unique clinical challenge in which the efficacy of eradicating malignant cells throughout the body must be weighed against the toxicities caused by irradiating all major organs. Of particular interest, subacute and long-term lung toxicities, such as pneumonitis and fibrosis, remain the main dose-limiting toxicities of TBI.3,4 For this reason, significant interest exists in the development of more advanced lung sparing TBI delivery techniques.
There are a variety of planning techniques to deliver TBI, the majority based on traditional 2D techniques with extended source-to-surface distance (SSD) fields. 5 To achieve lung-sparing TBI using 2D techniques, many centers, including our own, will machine custom molded lung blocks for each patient based on lung volume outlines acquired from computed tomography (CT) scan. During treatment, these blocks are precisely positioned between the source and the patients’ lungs to reduce lung dose. While there certainly exists institutional variation with regards to rigging and aligning these lung blocks, all TBI with lung blocks poses the challenge of machining custom blocks and their precise alignment before treatment.5,6 This can be quite challenging for many patients and radiation therapists. There is considerable interest in exploring whether VMAT based TBI treatments may help reduce this setup complexity.
VMAT is a form of radiation treatment that delivers radiation in a continuous arc around the patient, allowing for precise targeting of the tumor while sparing surrounding healthy tissue. Within the last several years, VMAT-based organ-sparing TBI has become a topic of interest, with the advantages of effective tissue sparing and the potential for shorter treatment times.7,8 VMAT TBI has been studied extensively and is routinely clinically implemented in various clinics throughout the world with traditional c-arm linear accelerators (linacs)9-11 and TomoTherapy™ machines.12-14 A recent Children’s Oncology Group (COG) study reported that while only 14 institutions (16% of respondents) use VMAT or TomoTherapy-based planning, 79% favor developing more advanced techniques to reduce lung dose. 4 Several institutions have now published protocols for c-arm linac-based VMAT TBI 11 and there have been 4 studies following patients treated with VMAT TBI: Tas et al, Marquez et al, Yaray et al, and Zhang-Velten et al.8,11,15-17
Given the growing implementation of VMAT-TBI using c-arm linacs, there has also been more recent interest in exploring the feasibility of VMAT-TBI using the Varian Halcyon™ o-ring linac. This is of particular interest for smaller, single-linac centers where Halcyon linacs are commonly employed and in which traditional extended SSD treatments are often not possible due to restricted vault size. However, the reduced maximum field size (28 cm × 28 cm) of Halcyon machines as well as the lower maximum dose rate (800 MU/min) pose a significant challenge to Halcyon-based VMAT TBI. This study investigates the dosimetric capability and planning feasibility of lung sparing Halcyon-based VMAT-TBI for pediatric patients, where the smaller field size may introduce less limitations to efficient therapy. This study also aims to demonstrate the potential role for Halcyon in expanding access to advanced, organ sparing TBI therapy in pediatric patient populations and to smaller centers which may only have Halcyon machines and/or lack the space necessary for extended SSDs. Published works have provided single adult patient experiences in VMAT TBI18,19 and VMAT Total Marrow Irradiation (TMI) 20 on Halcyon linacs; however this study expands the dosimetric analysis to a larger cohort of 10 pediatric patients, where lung-sparing TBI is of particular clinical interest.
Methods
Structure Segmentation
10 pediatric patient cases of varying ages (3 – 11 years) and sizes (94 – 134 cm), who previously received 2 Gy × 6 fractions (12 Gy) traditional 3D-based lung-sparing TBI at the University of Pennsylvania, were retrospectively replanned with a VMAT technique on a Halcyon linac. Halcyon enclosed O-ring gantries have a couch longitudinal travel limit of 165.5 cm, which would require taller patients to be flipped from head-first supine to feet-first supine part-way through treatment. To account for this, the patients’ full-body computed-tomography (CT) simulation scans were duplicated with the orientation flipped, with both orientations registered together for cumulative dose assessments. CT slice thickness was 3 mm for each patient scan.
Due to the Halcyon field size limitations, planning target structures were separated into 5 total target regions: 3 main body regions (brain, abdomen, and legs) and 2 field matching sections. Field matching regions were placed at regions of known daily set-up variations: (1) chin, neck, and shoulders, and (2) pubic symphysis and upper thighs. For VMAT optimization, the lungs were contoured and cropped out of the abdomen target contour with a 0.5 cm margin to allow for dose fall-off prior to the lung tissue interface. To assess overall plan quality, all 5 targets were combined, retaining the 0.5 cm margin outside of the lungs.
Planning
All planning was performed using Eclipse™ Treatment Planning System (TPS) AAA® ver. 16.10 (Varian Medical Systems Palo Alto, CA, USA) using Halcyon version E, in which field junction overlap optimization is done automatically. The Halcyon linear accelerator employs a 6MV flattening filter free (FFF) beam, which was used for all treatment plans. The collimator angles for each pair of coplanar arcs was selected to be complementary (e.g. 330 an 30 degrees, or 350 and 10 degrees). Halcyon leaf characteristics include a dual stacked and staggered design with leaf thickness of approximately 7.7 cm. 21 A 2.5 mm calculation grid was used for each patient plan. For the 2 field matching regions, a traditional feathering-based 3D planning technique was performed with 2 plans (2 Gy x 3 fractions each). For all matching regions, the first field opening was defined to match the edges of the superior and inferior target regions exactly, while the second field openings were one multileaf collimator (MLC) width smaller (equaling 2 cm total) in both superior and inferior directions. The Radformation EZFluence™ (Radformation Inc. New York, NY, USA) software was used to create uniform fluence within the AP-PA field matching regions.22,23 Within the EZFluence software, fluence optimization was performed to limit the hot spot to 105%, after which the transmission was manually adjusted within the TPS to reduce hot spots between matching and VMAT planning regions. For one particularly small patient (length = 95 cm), only 2 VMAT planning regions were used, requiring only 1 matching region.
VMAT planning with the Halcyon 2.0 automated multi-isocenter (Varian Medical Systems Palo Alto, CA, USA) treatment technique was used for the 3 main body regions: brain, abdomen, and legs. For the brain, one isocenter was used with 2 full 360° arcs. For the abdomen and leg regions, 3-4 isocenters were used, with each isocenter containing 2-2.5 arcs depending on patient thickness and simulation positioning. Overlap between isocenter groupings was set to approximately 7 cm. Within Halcyon treatment planning, an automatic isocenter grouping is possible to allow for automatic second isocenter alignment. The limit of this grouping is 8 cm. Any isocenter shift that is less than the 8 cm limit will allow for imaging at the first isocenter and an automatic translation. For the treatment plans highlighted in this study, a 7 cm isocenter shift, or overlapping region between isocenter groups, was utilized. While Halcyon plans can automatically shift to a second isocenter if the isocenter shifts are only in the superior-inferior direction separated by 8 cm or less, separate plans can be created to deliver the arcs from isocenters that are further apart. Figure 1 provides a visual representation of the VMAT isocenter grouping placements and planning target volumes for a 105 cm patient. VMAT group specific target objectives included: Dmax ≤ 14 Gy, D90% ≥ 12 Gy, and V110% ≤ 5%. Lung sparing was optimized to a mean dose of ≤ 6 Gy and Dmax ≤ 12 Gy. Planning optimization structures and 12 VMAT isocenter grouping placements for 1 patient of 105 cm length (Purple = brain planning target, green = matching region 1, maroon = abdomen planning target, orange = matching region 2, and cyan = leg planning target). AP-PA matching fields are not pictured
Plan Evaluation
Plan quality was evaluated on 2 metrics: (1) dosimetric quality and (2) planning and delivery quality. Overall dosimetric plan quality was performed by analyzing the total body target structure with a 0.5 cm margin around the lungs, with dose metrics including maximum dose, mean target dose, V100%, D90%, mean lung doses, and homogeneity indexes (
Planning and delivery quality analysis contained total planning time, the number of isocenters, number of plans, machine delivery time, and gamma passing rates. Quality assurance of all treatment plans was performed with portal dosimetry using Varian Eclipse Version 16.10 AAA®, reporting both 2%/2mm and 3%/3mm gamma passing rates with a 10% dose threshold.
Results
Dosimetric Analysis
Dosimetric Plan Quality Analysis*

All relative doses are with respect to a prescribed dose of 12 Gy.
The maximum doses produced by Halcyon-based VMAT planning were significantly reduced compared to traditional 3D planning techniques. The average maximum dose from VMAT was 16.5 ± 0.63 Gy (137% ± 5.2%), while for 3D planning was 20.1 ± 9.7 Gy (167.6% ± 0.8%). The 3D plan maximum doses were acquired from the resulting treatment plans generated. An example of the generated plan figure can be seen in the Appendix (Figure S1). These maximum doses are consistent with prior work with Halcyon VMAT TBI.18,19 Dose homogeneity, which can be visualized in Figure 2, was acceptable, with homogeneity indexes varying from 0.75 – 1.06, with a mean value of 0.92 ± 0.10. When compared to traditional 3D planning techniques, the overall dose homogeneity is reduced, with an average homogeneity index of 0.29 ± 0.04 for 3D planning. This is expected due to the significant dose modulation occurring within VMAT planning techniques compared with open field 3D techniques. There is a loss of dose homogeneity within the 3D matching regions, this is due to manual hot spot reduction to reduce the maximum dose to <105%. However, if an institution prefers more uniform coverage, the level of hot spot reduction can be reduced to maintain coverage. Coronal views of a mid-plane halcyon VMAT dose distributions for 4 patients with a dose range of 10.8 Gy (90% of prescription dose) up to the maximum dose within the plan
Lung Dose Comparison Between Traditional 3D and VMAT Planning Techniques

Planning and Delivery Analysis
Planning Workflow Analysis

Plan Delivery Time Analysis
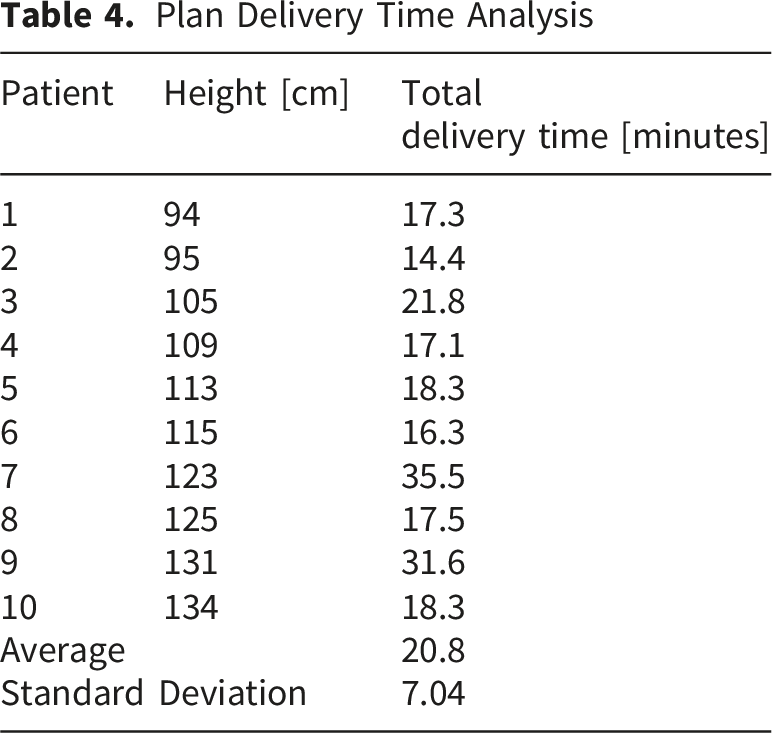
Typical clinical 3D based lung sparing TBI treatment appointment scheduling is for 60 minutes per fraction, with typical patient set-up times of 10 – 15 minutes and beam on times of 30 – 40 minutes. Additionally for lung sparing patients, an imaging appointment of typically 90 minutes must be added to define the lung block positioning on the patient’s skin as described previously. For the 10 patients included within this study, the average active beam on time was 31.5 ± 3.8 minutes, with an average lung block imaging appointment taking 73.9 minutes. The estimated set-up and imaging time for a VMAT based TBI treatment on the Halcyon is 20 – 30 minutes, given the fast delivery of kV cone-beam CT (CBCT) imaging and the necessity to flip the orientation of the patient and reimage half-way through treatment. When comparing the total treatment time of traditional 3D based TBI treatments and a Halcyon based VMAT TBI treatment, cumulative treatment times are estimated to be of similar time length with the potential for reduced treatment time for smaller patients due to reduced beam-on time.
2%/2 mm γ Passing Rates
3%/3 mm γ Passing Rates

Discussion
Institutions clinically implementing VMAT TBI with c-arm LINACs have shown feasibility in delivering 12 – 14 Gy to the entire body while keeping mean dose to the lungs at 6 – 10 Gy without the need for lung shielding. 20 In this regard, the Halcyon plans created within this study are comparable to c-arm linac-based VMAT TBI as well as traditional 2D TBI with lung blocks. This study also encountered several advantages and disadvantages of Halcyon TBI for treatment delivery compared to a standard c-arm linac. Advantages of Halcyon VMAT TBI include advanced patient positioning verification using CBCT at each treatment isocenter, faster gantry rotation (2 RPMs), and lower MLC leakage. Disadvantages of Halcyon VMAT TBI are notable for smaller field sizes, fixed and reduced SSD, lack of lateral isocenter positioning, and lower dose rate delivery, most notable among these being the smaller field size. This resulted in increased planning time compared to traditional 3D techniques (6 hours vs 3 -5 hours). 26 Moreover, the table travel limits would require taller patients to be flipped part-way through treatment, necessitating a new setup, imaging, and alignment process. This issue has been bypassed with c-arm linacs by utilizing a rotating treatment table,11,25 but the enclosed bore design with attached treatment couch of the Halcyon precludes this solution and would require new developments. For these reasons, while lung sparing Halcyon TBI is dosimetrically feasible, pediatric patients are ultimately most likely to benefit from the further development of this technology by virtue of their smaller size. Additionally, the feasibility of Halcyon VMAT TBI could potentially expand access to TBI therapies to smaller, more resource limited clinics which may only have Halcyons or lack a vault large enough for 2D extended SSD setups.
In addition to the technical limitations posed by Halcyon, this study also has several methodological limitations worth noting. Firstly, this study was planned retrospectively using CT scans that had been used to delineate lung volume outlines for lung block machining for patients receiving 3D TBI. Reproducible extremity placement was not considered during these simulations, resulting in several patients within this study having far spread apart legs and arms. This resulted in plans containing substantially higher monitor units and modulation factors in these regions as well as longer delivery times and reduced dose coverage. If we had used full-body CT scans with more desirable patient positioning, target coverage could be increased, and treatment delivery time would likely decrease. An additional limitation caused by the retrospective nature of this study is the inability to measure actual plan delivery time. As no patients were treated with this technique, only estimates can be made regarding the expected scheduling time required for patient setup, imaging, and alignment. A review of patient setup, imaging, and delivery were provided for the traditional 3D-based planning with lung blocks to provide a better comparison of entire treatment time between traditional 3D and VMAT techniques. However, additional scheduling time would need to be allotted to patients who exceed the table travel limitations on the Halcyon couch, which would require an orientation-flip with re-imaging and alignment. Despite limitations, both technical and methodological this study overall supports dosimetric feasibility of VMAT TBI on Halcyon, especially in a pediatric and low resource setting.
It is worth also discussing the current clinical considerations of VMAT TBI. Most notably, it is not yet known whether the dosimetric capabilities of VMAT TBI correlate to improved outcomes for patients, as there is only limited data following patients treated with techniques. That said, early follow-up studies of patients treated with VMAT TBI may suggest an overall trend towards lower rates of level 3+ pneumopathies compared to traditional TBI. 27 A recent retrospective study reported that only 4 of 32 patients (12.5%) receiving myeloablative VMAT TBI had grade 3+ pneumonitis, with 3 in the setting of documented respiratory infection and only 1 (3.1%) believed to be solely radiation-related. 17 Zhang-Velten et al suggest these outcomes are a tentative improvement on standard-dose traditional TBI, citing studies suggesting grade 3+ pneumonitis can occur in 10% to 30% of patients with lung shielding and fractionation28-30 and 50% of patients treated with single fraction (8 – 10 Gy). 31 In a study of VMAT TBI outcomes in pediatric and young adult patients, those treated with myeloablative regimens reported consistent lung sparing to 58.5% of the mean dose at an average of 7.3 Gy with 100% overall survival and relapse free survival. 15 Among patients treated with a non-myeloablative regimens, 2 of the 4 deaths reported were due to acute respiratory distress syndrome neither of which were fully attributable to radiation therapy. Importantly, no early pulmonary toxicity or nephrotoxicity related to VMAT TBI were reported. Finally, Tas et al reported on 30 patients with ALL and AML treated with VMAT TBI. 8 No 3+ lung toxicities were seen in this study. Overall, more clinical outcomes data is needed to fully characterize the efficacy of VMAT TBI, but these early data may be beginning to suggest an overall reduction in rate and severity of adverse effects, most notably lung toxicity.
It is yet to be determined whether these same potential outcome improvements seen in these studies using c-arm linac-based methods might also be achievable with Halcyon-based VMAT TBI. However, given the plans obtained within this study achieve a similar reduction in mean lung doses on the order of 6 – 7 Gy, a clinical trial of Halcyon VMAT TBI may be feasible and safe.
Additionally, now that significant reductions in lung dose are feasible with VMAT TBI on Halcyon and TrueBeam™, future research may need to pivot focus towards optimizing for a specific lung dose rather than simply pushing towards the lowest technically feasible dose. In this regard, it will be important to understand more about relapse rates across lung dose levels in patients treated with lung sparing TBI. For instance, while a lung dose of 6 – 7 Gy is possible, sufficient data are not available to suggest that this is the most clinically appropriate target dose when weighing pneumopathy risk against recurrence risk. For this reason, considerable attention must go towards optimizing towards a target dose that best balances the many factors which affect overall patient outcomes. Current evidence and guidelines suggest that 8 Gy is an appropriate upper limit for lung dose beyond which patient outcomes are known to deteriorate; however, further study is needed to find the most appropriate lower limit.
Another under explored distinction between conventional 2D TBI and VMAT TBI are consideration of dose rate. In conventional 2D based TBI, treatment delivery has long been reduced to <5-10 cGy/min to reduce the likelihood of pulmonary toxicities.5,32-34 However, no recommendations are provided on what dose rate to use for VMAT based TBI since the dose rate delivery is different between conventional and VMAT based TBI, 17 and studies have shown no additional lung toxicities due to increased delivered dose rate. 8 Previous works have reduce the MU delivery rate within the lung isocenter regions, 35 but no clinical evidence suggests if this technique is necessary or reduces pulmonary toxicities at the present time.
Moreover, an emerging concern with VMAT TBI more broadly is that irradiating the body in sequential segments might diminish the eradication of malignant cells. 1 This is especially relevant considering the importance of TBI in the treatment of hematological malignancies where malignant cells may be circulating the body crossing in and out of radiation fields during the time of treatment. This further underscores the overall need for VMAT TBI clinical trials and for published long-term follow up data on survival and recurrence outcomes. Marquez et al also demonstrated that VMAT TBI can simultaneously escalate dose to areas of risk and reduce dose to areas of concern, providing another tool for more advanced targeted therapies. 15
Conclusions
Halcyon VMAT lung sparing TBI achieves dosimetrically acceptable target coverage, maximum doses, and mean lung dose sparing, with significant reduction of expected lung doses compared to traditional 3D based lung sparing TBI planning techniques. However, due to the inherent challenges of planning and treating taller patients, Halcyon delivered VMAT TBI with lung sparing is most feasible for smaller patients (<100 cm); similar to recommendations produced by previous works. 20 There may exist a place for Halcyon VMAT TBI in pediatric use and in cases where organ sparing is of particular importance. Future developments in workflow optimizations through novel software-based automations of target delineation and multiple field matching could allow for more simplified treatment of larger patients (>110 cm).
We believe there is a strong possibility that despite the significant increases to treatment planning complexity, there may exist an overall benefit to patients in the right setting and circumstances with VMAT TBI. Identifying appropriate candidates for VMAT TBI, improving planning workflows and setup time, and better characterizing the long-term outcomes of VMAT TBI are future areas for improvement. Moreover, better identifying a role that Halcyon-based VMAT TBI might serve in the small clinic and pediatric setting is of value. Finally, because pneumopathies are the primary dose limiting toxicity of TBI, should durable reductions in lung toxicity emerge with VMAT TBI, a dose escalation study may become feasible with the hope that lung dose can be kept within an acceptable range while delivering higher doses to the rest of the body. The ultimate goal of such a study would be to provide more robust cures while keeping dose to OARs and side effects within acceptable limits.
Supplemental Material
Supplemental Material - Dosimetric Performance Analysis of Pediatric Based Halcyon™ Volumetric Arc Therapy-Based Lung-Sparing Total Body Irradiation
Supplemental Material for Dosimetric Performance Analysis of Pediatric Based Halcyon™ Volumetric Arc Therapy-Based Lung-Sparing Total Body Irradiation by Allison Haertter, Keshav Goel, Jacob Niculcea, Taoran Li, Christine E. Hill-Kayser, John Plastaras, Michael J. LaRiviere, Michele M. Kim in Technology in Cancer Research & Treatment.
Footnotes
Ethical Considerations
This project was reviewed by the University of Pennsylvania Institutional Review Board (Protocol #26-5956) and was determined to qualify as a quality improvement initiative that does not meet the regulatory definition of human subjects research. As such, formal IRB approval and ongoing oversight were not required.
Consent to Participate
The requirement for informed consent was waived as this study was classified as a quality improvement initiative and did not involve human subjects research as defined by applicable regulations.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr. LaRiviere reports having received travel funding by GE Healthcare in the past.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Taoran Li: reports employment with Varian Medical Systems.
Supplemental Material
Supplemental material for this article is available online.