
Abstract
Introduction
CT-guided biopsy has good diagnostic accuracy, but adverse events such as pneumothorax are common. There are few reports on the safety and efficacy of CT-guided biopsy in the elderly.
Methods
This was a retrospective single-centre cohort study. Patients who underwent CT-guided lung biopsy between February 2017 and August 2024 were included. Patient background, disease background, examination status, and adverse events were ascertained. Elderly were defined as those aged 75 years and older. The primary outcome was the incidence of all adverse events, and the secondary outcomes were the incidence of pneumothorax and diagnostic accuracy. Categorical variables were compared by Chi-square test, and continuous variables by t-test. Multivariable analysis was performed by logistic regression analysis adjusted for age, sex, lung comorbidities, and radiological findings of target lesion.
Results
There were significant differences between the two groups in ECOG-PS and the distance from the surface to pleura and target. In the primary outcome, any adverse events occurred in 207 patients (56.2%), with no significant difference between elderly (97/180, 53.9%) and non-elderly (110/188, 58.5%) patients (p = 0.401). Pneumothorax was the most common adverse event, occurring in 151 (41.0%) patients, with no significant difference between elderly (68/180, 37.8%) and non-elderly (83/188, 44.1%) (p = 0.244). On multivariate analysis, elderly (75years or older) was not clearly associated with the occurrence of all or severe adverse events, pneumothorax, and confirmed diagnosis. Location in the lower lung field and distant from the pleura were significantly associated with the incidence of all adverse event. In the secondary outcomes, emphysema or interstitial pneumonia, location in the lower lung field, and distant from the pleura were significantly associated with pneumothorax. There was no significant difference in the diagnostic accuracy disease between the elderly and non-elderly patients.
Conclusions
The incidence of adverse events and diagnostic accuracy of CT-guided biopsy are similar in elderly and non-elderly patients, and this method is useful even in elderly patients.
The safety and efficacy of CT-guided lung biopsy in elderly patients are equivalent to those in non-elderly patients.
Introduction
Computed tomography (CT)-guided lung biopsy is one of the methods of lung biopsy. Compared to conventional bronchoscopy, 1 it shows good diagnostic accuracy with a sensitivity of 90% and specificity of 95% for malignant tumors. 2 Because it can be performed in an awake state and is less painful than bronchoscopy, it may be safe for elderly patients who have concerns about complications from general anesthesia or sedation. On the other hand, there are complications such as pneumothorax and hemorrhage.3,4 Pneumothorax is estimated to be 20–40%, pneumothorax requiring drainage 7%, and hemorrhage 3–8%.5,6 Regardless of tumor morphology (solid, part-solid, ground glass nodule) or small lesion (<20 mm), CT-guided lung biopsy has been shown to be safe and effective.7–12 However, few reports have evaluated safety and efficacy in the elderly.1,13 In order to evaluate the primary outcome of the incidence of all adverse events, and the secondary outcomes of the incidence of pneumothorax and diagnostic accuracy, we hypothesized that CT-guided lung biopsy would not be associated with higher adverse event rates in patients aged ≥75 years compared with younger patients and performed a detailed analysis of elderly cases in which CT-guided biopsy was performed at our hospital.
Patients and Methods
Patients’ Selection
This was a retrospective study. Patients scheduled for CT-guided lung biopsy between February 2017 and August 2024 were selected. Patients for whom the procedure was intended for drainage and patients for whom the procedure was cancelled were excluded. Patients who had undergone thoracis radiotherapy were included. Patients who had previously undergone CT-guided biopsy were treated as separate cases, and duplication was permitted. The number of CT-guided biopsy sessions received was described as the number of examinations. Patients receiving antiplatelet and/or anticoagulant therapy were also included. We performed CT-guided biopsy after allowing an appropriate washout period for patients undergoing antiplatelet or anticoagulant therapy. We set the washout period to 7 days for clopidogrel and 3 days for ticlopidine, while aspirin was not discontinued.
Baseline Characteristics
Patient backgrounds included age, sex, body mass index (BMI), Eastern Cooperative Oncology Group-Performance status (ECOG-PS), smoking status, comorbidities (emphysema, interstitial pneumonia (IP), asthma, hypertension, diabetes mellitus, chronic kidney disease, cardiovascular diseases, cerebrovascular diseases, malignancy), and antithrombotic therapy (use of anticoagulant or antiplatelet). Disease backgrounds included location of the target lesions, longest diameter of lesions, depth from the surface to the proximal end of target lesion, depth from the surface to the pleura, and lesion type (solid, part-solid, non-solid). Location of the target lesions is classified by upper lung field (both upper lobe of the lung), lower lung field (middle lobe, lower lobe, and lingula), and others. The examination status included the purpose of the examination, the position of the patient during the examination, and the time required. Adverse events included pneumothorax, pneumothorax requiring drainage and its duration, hemoptysis, hypoxia defined as decline of SpO2 under 95% in the ambient air, arrhythmia, fever (38 °C or higher), and infections. Severe adverse events are defined as those requiring additional treatment or unexpected delay in discharge such as pneumothorax requiring drainage, haemoptysis requiring intubation, and hypoxia due to pneumothorax, haemoptysis, or infection. Infections encompassed all perioperative infections (including both post-biopsy pneumonia and localized site infection). Furthermore, an unexpected delay in discharge was defined as a delay exceeding 24 h. We also collected on the diagnosis (final diagnosis, diagnostic accuracy, and insufficient for oncogene testing).
Grouping
Patients aged 75 years or older at the time of the examination were defined as elderly, and were divided into two groups: elderly and non-elderly.
CT Guided Biopsy Techniques
First, two respiratory physicians and one radiologist reviewed the CT images to determine whether CT-guided biopsy would be appropriate. In conducting, we employed a 21- or 22-gauge biopsy needle. Needle lengths of 80 mm or 160 mm are available, selected at the attending physician's discretion based on lesion depth. Patient positioning was determined by lesion location, performed either supine position, prone position or lateral position. The procedure is performed under local anaesthesia with 1% xylocaine. For patients experiencing significant anxiety, pentazocine may be administered intramuscularly beforehand (this applies to less than 1% of patients). The examination is conducted in the presence of at least two respiratory physicians (one of whom must have over ten years’ experience) and one radiological technologist.
For patients taking aspirin orally, the procedure is performed without interruption. For other antithrombotic agents, the procedure is performed after observing the specified withdrawal period for each drug. Heparin replacement is only performed when specifically requested.
The number of biopsies ranges from one to four. If a sufficient specimen is obtained in one attempt, the procedure concludes there. However, if the specimen volume is inadequate, up to four biopsies may be performed. All decisions regarding this are made at the discretion of the attending physician.
At our hospital, this examination is performed on all patients during their hospital stay. Following the procedure, patients must remain in bed for two hours. After this period, a chest x-ray is conducted to confirm the absence of pneumothorax, at which point restrictions are lifted.
Outcome
The primary outcome was the incidence of all adverse events, and the secondary outcomes were the incidence of pneumothorax and the diagnostic accuracy evaluated by the proportion of confirmed diagnosis by CT-guided biopsy.
Statistical Analysis
The baseline characteristics of the patients were described in accordance with the groups by age. Categorical variables are presented as counts and percentages, and continuous variables are presented as the mean and standard deviation (SD). Normal distribution of continuous variables was confirmed by the Shapiro-Wilk test. Univariable analyses were performed by Chi-squared test or Fisher's exact test which appropriate for categorical variables and by Welch's t-test for continuous variables. Multivariable analysis regarding the safety of CT-guided biopsy for elderly patients and the diagnostic accuracy were performed by Logistic regression analysis, adjusted by sex, overweight or obesity (defined as no less than 25 kg/m2 of BMI), poor performance status, comorbidity with COPD or IP, depth to the pleura (dichotomized at 30 mm), and the radiological findings such as location in the lower lung field, distant from the pleura, smaller than 20 mm of the longest diameter, and lesion type (solid or not). As a sensitivity analysis for confirmed diagnosis, we also performed Logistic regression analysis adjusted by the factors described above other than depth to the pleura and depth to the target. Statistical tests with a two-sided P value of less than 0.05 as statistically significant. All statistical analyses were performed by using R version 4.5.1 (R Foundation for Statistical Computing, Vienna, Austria).
Ethics
All the authors had no conflicts of interest concerning the present study. This study complied with the principles of the World Medical Association Declaration of Helsinki. This study was reviewed and approved by the National Hospital Organization Kyoto Medical Center Institutional Review Board (Approval number: 24-025). This was a retrospective study, and no consent was obtained from the patients. Instead, an opt-out method was used, which guaranteed the right of the participants to refuse to participate in the study. The results were reported according to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement. 14
Results
Patient's Selection
Patient selection is shown in Figure 1. From February 2017 to August 2024, 396 patients were scheduled for CT-guided examinations. 23 patients who were intended for drainage were excluded. 5 patients who discontinued the examination were excluded. Biopsies were performed on a total of 368 patients (180 elderly and 188 non-elderly).

Study flowchart. Screening, patient selection, exclusion, and classification.
Baseline Characteristics
Patient characteristics are shown in Table 1. The median age was 80.87 years for the elderly and 67.48 years for the non-elderly. 105 patients (28.5%) had emphysema, and 27 patients (7.3%) had interstitial pneumonia, with almost no difference between elderly and non-elderly patients. There were no statistically significant differences in sex, performance status, smoking status, comorbidities, or antithrombotic drug use.
Baseline Characteristics of the Patients.

Data are shown with mean and (standard deviation) or number and (percentage).
The existence of emphysema and interstitial pneumonia was confirmed by a chest CT taken just before the CT-guided biopsy.
BMI; body mass index, ECOG-PS; Eastern Cooperation of Oncology Group Performance Status, IP; interstitial pneumonia.
Radiological Findings of Target Legions and Procedures for CT-Guided Lung Biopsy
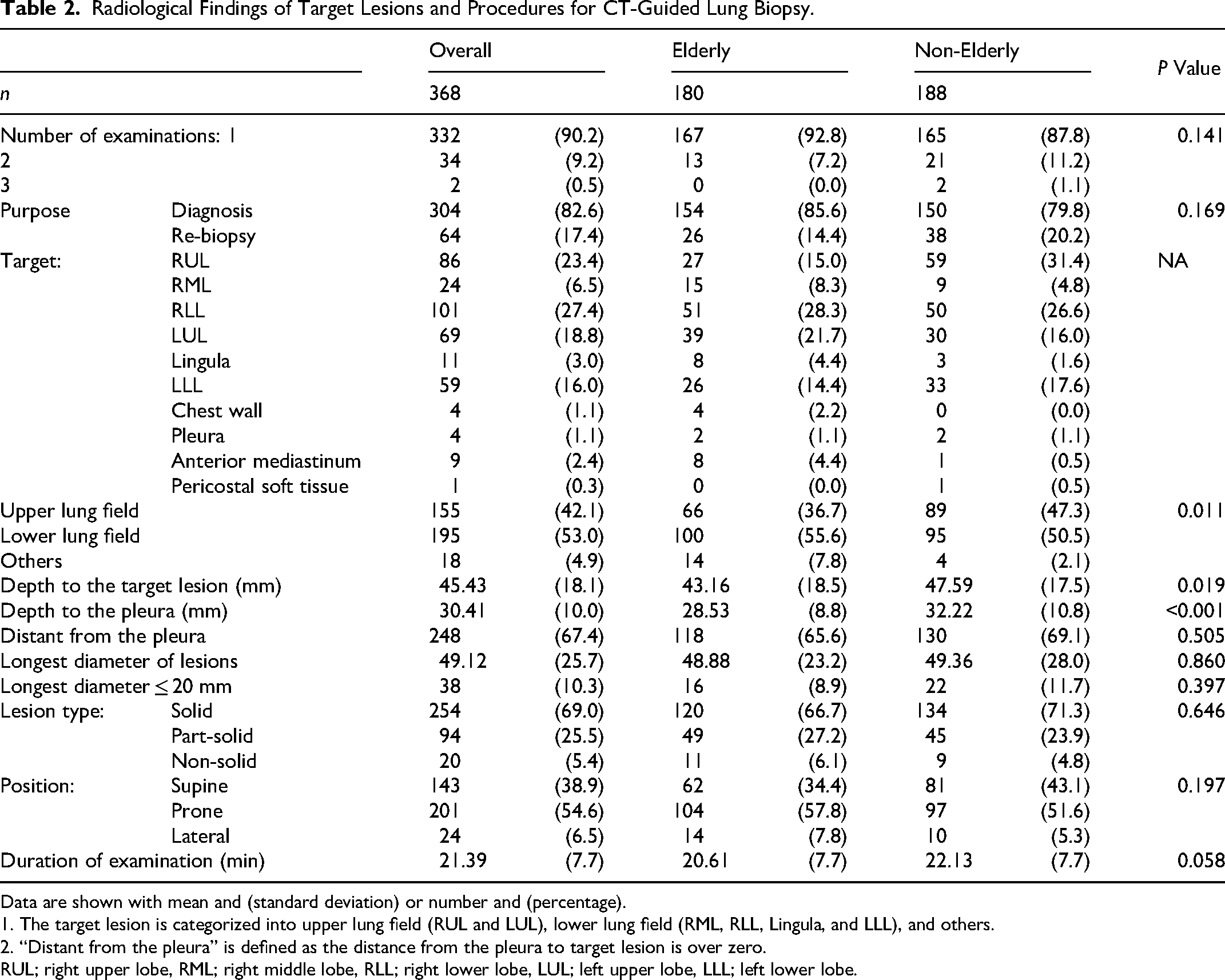
Target lesions and examination procedures are shown in Table 2. Overall, 53.0% of the target sites were in the lower lung field and 42.1% in the upper lung field. There was significantly difference in the location of target lesion between the elderly and non-elderly (p = 0.011). However, the lower lung field, which is considered a risk for pneumothorax, 10 was not significantly different among the elderly (55.6%) and non-elderly (50.5%) (p = 0.349). The overall depth from the surface to the target lesion was 45.43 mm (43.16 mm for the elderly, 47.59 mm for the non-elderly), significantly shorter in the elderly (p = 0.019). Likewise, the depth to the pleura was significantly shorter in the elderly than the non-elderly (28.53 mm vs 32.22 mm, p < 0.001). The percentage of patients whose target lesion was distant from the pleura was 65.6% in the elderly and 69.1% in the non-elderly, with no significant difference. Duration of examination tended to be longer in the non-elderly, but not significantly different (p = 0.058).
Radiological Findings of Target Lesions and Procedures for CT-Guided Lung Biopsy.
Data are shown with mean and (standard deviation) or number and (percentage).
1. The target lesion is categorized into upper lung field (RUL and LUL), lower lung field (RML, RLL, Lingula, and LLL), and others.
2. “Distant from the pleura” is defined as the distance from the pleura to target lesion is over zero.
RUL; right upper lobe, RML; right middle lobe, RLL; right lower lobe, LUL; left upper lobe, LLL; left lower lobe.
Outcomes of CT Guided Lung Biopsy
Adverse events and diagnoses are shown in Table 3. Incidence and 95% CI of primary and secondary outcomes grouped by age are displayed in Figure 2. The diagnostic rate for CT-guided lung biopsy was 75.3%. Among the diagnosed diseases, malignant tumors accounted for 86.3% and benign diseases for 13.7%. The diagnostic accuracy for malignancy was 65.5 versus 64.3, P = 0.896, and that for benign nodules was 12.8 versus 8.0, P = 0.180; no significant difference was observed between the elderly and non-elderly patients for either.

Incidence and 95% CI of primary and secondary outcomes. Diamonds indicate actual incidence of each outcome, and error bars indicate 95% CI. No outcome shows a significant difference between the elderly and non-elderly.
Outcomes of CT-Guided Biopsy.
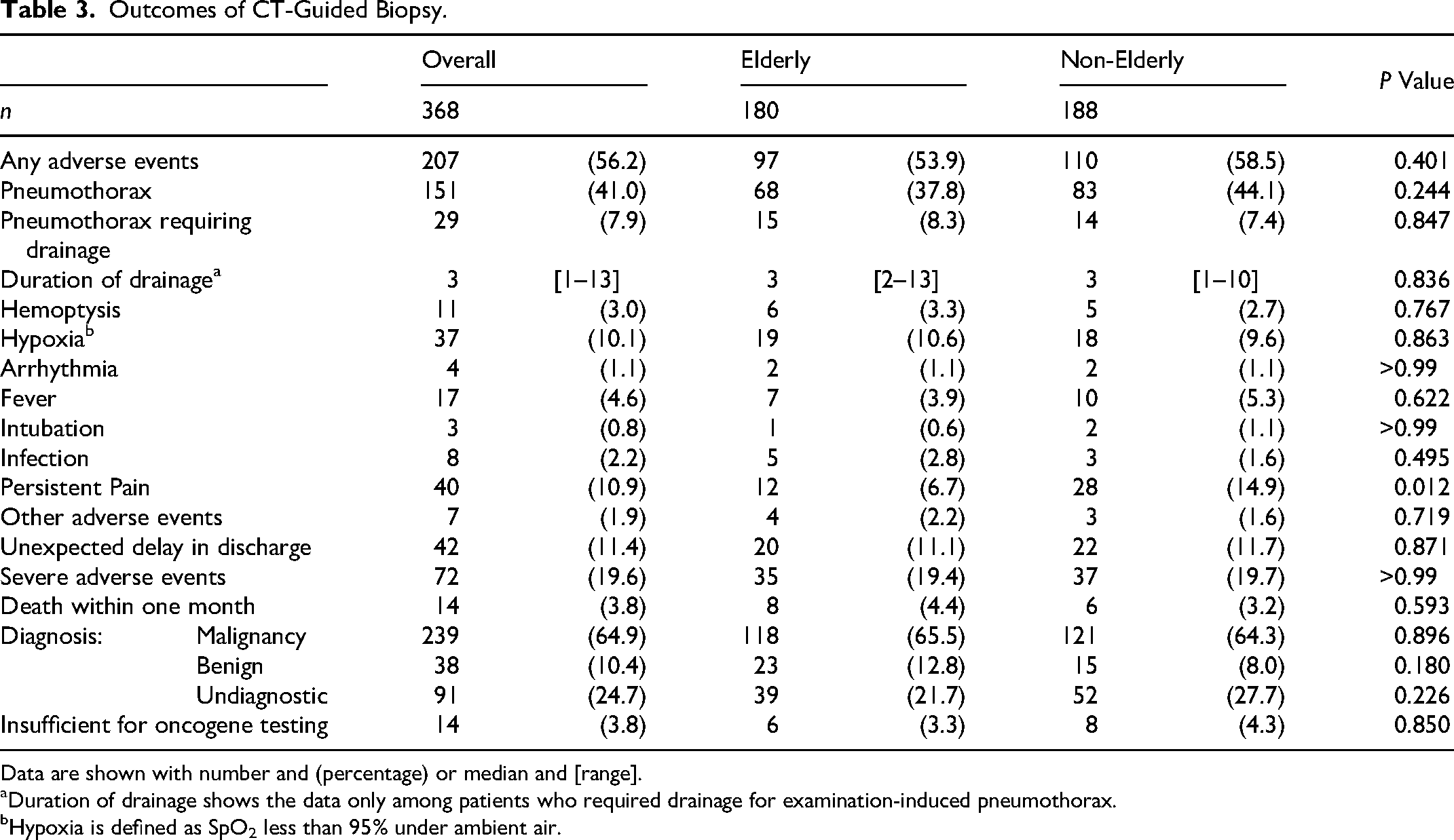
Data are shown with number and (percentage) or median and [range].
Duration of drainage shows the data only among patients who required drainage for examination-induced pneumothorax.
Hypoxia is defined as SpO2 less than 95% under ambient air.
Overall, any adverse events occurred in 207 patients (56.2%), with no significant difference between elderly (97/180, 53.9%) and non-elderly (110/188, 58.5%) patients (p = 0.401). Pneumothorax was the most common adverse event occurring in 151 (41.0%) patients, with no significant difference between elderly (68/180, 37.8%) and non-elderly (83/188, 44.1%) (p = 0.244). Pneumothorax requiring drainage occurred in 29 patients (7.9%), with no significant difference between elderly (15/180, 8.3%) and non-elderly (14/188, 7.4%) (p = 0.847). The median duration of drainage was 3 days. Hemoptysis occurred in 11 patients (3%) overall. Unexpected delay in discharge occurred in 42 patients (11.4%) and death within one month occurred in 14 patients (3.8%), with no significant difference between elderly and non-elderly. Severe adverse events occurred in 35 (19.4%) patients of the elderly and 37 (19.7%) patients of the non-elderly (p > 0.99). All deaths occurring within one month were attributable to the underlying disease, and there were no fatalities related to the CT-guided biopsy procedure.
Multivariable Analysis for Adverse Events
Logistic regression analysis for all adverse events is shown in Table 4. The location in the lower lung field (OR 1.82, 95%CI 1.16-2.86, p = 0.010) and lesions distant from the pleura (OR 3.91, 95%CI 2.42-6.31, p < 0.001) were independent risk factors for all adverse events. Meanwhile, Logistic regression analysis for severe adverse events is shown in Table 5. Poor performance status (OR 2.04, 95%CI 1.07-3.88, p = 0.030), existence of emphysema or interstitial pneumonia (OR 2.26, 95%CI 1.27-4.00, p = 0.005) and lesions distant from the pleura (OR 2.04, 95%CI 1.10-3.79, p = 0.024) were independent risk factors for severe adverse events. Elderly was not a significant factor associated with all or severe adverse events.
Multivariable Analysis for all Adverse Events.

Odds ratios and 95% confidence intervals are estimated by the Logistic regression analysis.
OR; odds ratio, CI; confidence interval, ECOG-PS; Eastern Cooperation of Oncology Group Performance Status, IP; interstitial pneumonia.
Multivariable Analysis for Severe Adverse Events.

Odds ratios and 95% confidence intervals are estimated by the Logistic regression analysis.
OR; odds ratio, CI; confidence interval, ECOG-PS; Eastern Cooperation of Oncology Group Performance Status, IP; interstitial pneumonia.
Multivariable Analysis for Pneumothorax
Logistic regression analysis for pneumothorax is shown in Table 6. Existence of emphysema or interstitial pneumonia (OR 2.17, 95%CI 1.31-3.59, p = 0.003), lower lung field (OR 2.06, 95%CI 1.30-3.27, p = 0.002), distance from the pleura, (OR 2.82, 95%CI 1.69-4.70, p < 0.001) were independent risk factors for pneumothorax. In contrast, a score of ECOG-PS no less than 2 (OR 0.54, 95%CI 0.28-1.03, p = 0.063) showed a protective trend for pneumothorax. Elderly was not a significant factor associated with the incidence of pneumothorax.
Multivariable Analysis for Pneumothorax.
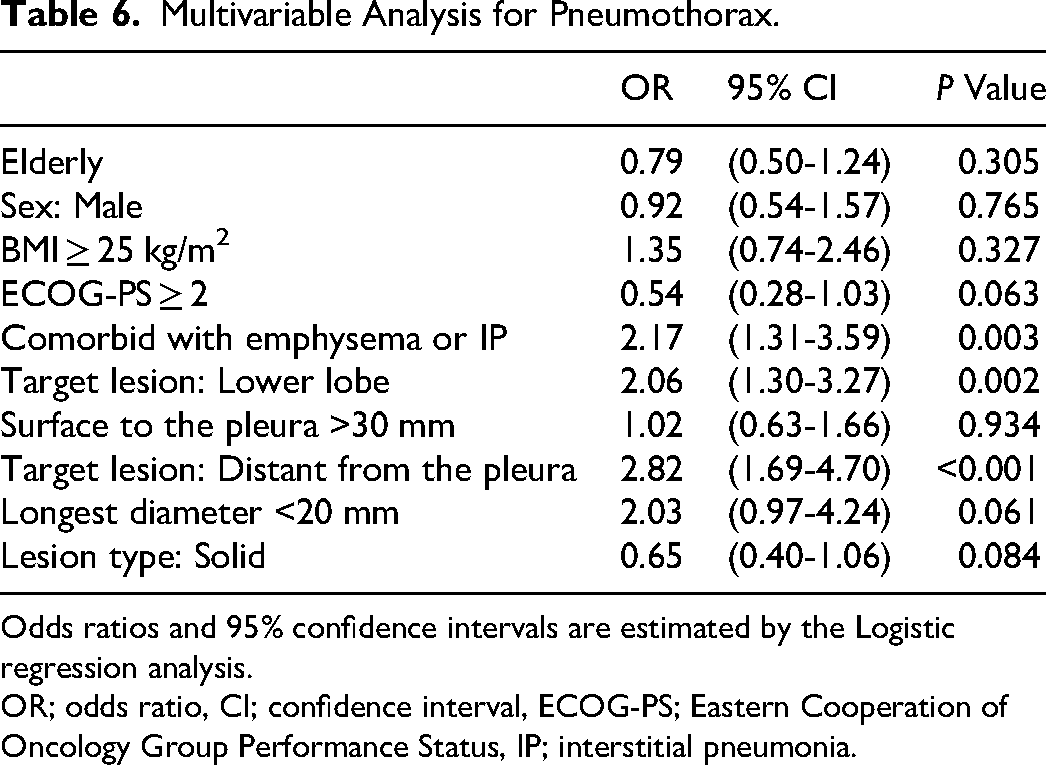
Odds ratios and 95% confidence intervals are estimated by the Logistic regression analysis.
OR; odds ratio, CI; confidence interval, ECOG-PS; Eastern Cooperation of Oncology Group Performance Status, IP; interstitial pneumonia.
Multivariable Analysis for Confirmed Diagnosis
Logistic regression analysis for diagnostic accuracy and sensitivity analysis are shown in Table 7. Lower lung field (OR 0.57, 95%CI 0.34-0.95, p = 0.031) and longest diameter <20 mm (OR 0.37, 95%CI 0.18-0.76, p = 0.007) were independent risk factors for failure to confirm the diagnosis. A sensitivity analysis for confirmed diagnosis also indicated the same trend; lower lung field (OR 0.59, 95%CI 0.35-0.98, p = 0.042) and longest diameter <20 mm (OR 0.36, 95%CI 0.18-0.73, p = 0.005) were independent risk factors for failure to confirm the diagnosis. In both analyses, the elderly was not a significant factor associated with confirmed diagnosis.
Multivariable Analysis for Confirmed Diagnosis.
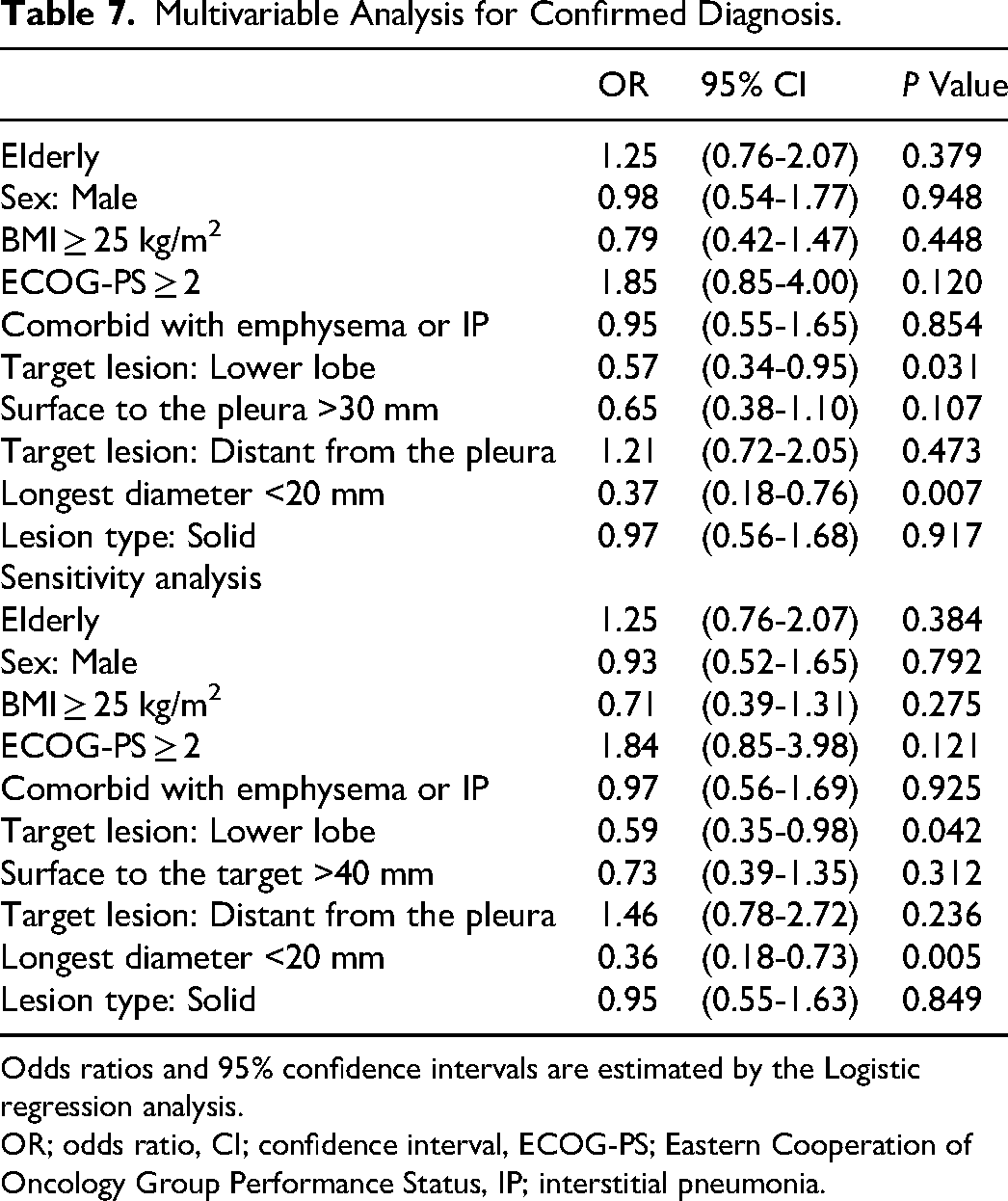
Odds ratios and 95% confidence intervals are estimated by the Logistic regression analysis.
OR; odds ratio, CI; confidence interval, ECOG-PS; Eastern Cooperation of Oncology Group Performance Status, IP; interstitial pneumonia.
Discussion
In this study, we compared adverse events from lung biopsies between elderly (≥75 years) and non-elderly patients and found no significant differences. Overall adverse events occurred in 56.2% of patients, with similar rates in both groups (53.9% vs 58.5%, p = 0.401). Pneumothorax was most common (41.0%), showing no age-related difference (37.8% vs 44.1%, p = 0.244). Multivariate analysis confirmed age wasn’t associated with adverse events. However, location in the lower lung field and deeper pleural lesions significantly increased risk of adverse events. Emphysema, interstitial pneumonia, location in the lower lung field, and pleural distance were linked to pneumothorax. Diagnostic accuracy showed no age-related differences, suggesting lung biopsy safety is comparable across age groups.
According to a large-scale meta-analysis by Heerink et al, the primary adverse events and their incidence were following. 15 Core needle biopsy: Overall complication rate 38.8% (95% CI: 34.3-43.5%). Fine needle aspiration biopsy (FNA): Overall complication rate 24.0% (95% CI: 18.2-30.8%). The incidence of major complications was: core biopsy 5.7% (4.4-7.4%), FNA 4.4% (2.7-7.0%). The most common complication, pneumothorax, occurred in 25.3% of core biopsies and 18.8% of FNAs. Of these, the proportion requiring thoracic drain insertion today was 5.6% for core biopsy and 4.3% for FNA. 15 Furthermore, Nakamura et al reported that risk factors for complications in FNA include the use of thicker needles (21G or thicker), smaller lesion size (risk decreasing by 3% for each 1 mm increase in lesion diameter), and increased distance traversing the lung parenchyma (risk increasing by 5% for each 1 mm increase). 16
Previous studies have also identified emphysema, lower lobe, distance from the pleura, depth from the pleura, number of punctures, and small lesions as independent risk factors for pneumothorax.6,10,11,17 However, according to a report by Takeshita et al, elderly (73 years or older) was an independent risk factor for pneumothorax requiring drainage. 5 It said that the elderly may be affected by decreased respiratory function, which makes it difficult for them to comply with breath-hold instructions during the examination. On the other hand, Yang et al reported that pneumothorax tended to be more common in elderly (65 years and older), but not significantly, and pulmonary hemorrhage showed little difference. 13 Our study was in support of the latter, and furthermore, it should be noted that the elderly group tended to frequently have targets in the lower lung field than the non-elderly group. Although the location in the lower lung field is associated with a higher risk of pneumothorax, the incidence of pneumothorax was still lower in the elderly group. This discrepancy may be associated with higher prevalence of poor PS in the elderly group than that in the non-elderly group, which had a protective trend for the incidence of pneumothorax. The protective effect of poor PS stems from the tendency to be reluctant to perform CT-guided biopsy on those with poor PS, particularly in patients with a high risk of pneumothorax.
The incidence of pneumothorax and pneumothorax requiring drainage in this study was 41% and 7.9%, similar to previous reports2,5,6,8,17,18 and not significantly different between the elderly and non-elderly groups. This suggests that CT-guided lung biopsy can be safely performed in the elderly. The median drainage period was 3 days, which is considered short enough not to affect the initiation of treatment.
In our study, the diagnosis rate was 75.3%, which appears to be lower than previously reported.5,7,8,10–12 Multivariable analysis and sensitive analysis for diagnostic accuracy showed that location in the lower lung field and targets distant from the pleura were the significant factors associated with failure to confirm the diagnosis. Although the diagnosis rate is reported to decrease when the depth from the surface to target >40 mm, the sensitivity analysis revealed that the depth was not associated with the diagnosis. 7 Approximately 2/3 of the cases in the present study had the lesions distant from the pleura, which may have contributed to decreasing diagnostic accuracy. We have not introduced rapid on-site cytologic evaluation at our hospital, which may have also contributed to the lower diagnostic rate. Moreover, biopsies including benign disease may have affected the diagnostic accuracy; the diagnosis rate of benign disease has been reported to be as low as 50–60%.19,20
Our study has several limitations. First, this study consisted of insufficient number of patients for detecting approximately 5% absolute difference of the risk; statistic power for any adverse events was 0.25, and that of pneumothorax was 0.41. However, this study had nearly sufficient power for 10% absolute difference; statistic power for 10% difference in any adverse events was between 0.79 and 0.81, and that in pneumothorax was between 0.78 to 0.82. Insufficient number of patients may also influence statistical reliability. In this study, 72 patients experienced severe adverse events overall; however, overfitting may have occurred because the multivariate analysis included 10 factors. Second, as this is a single-centre study, there is variability in patient characteristics and in physicians’ treatment approaches, making direct comparison with other centres difficult. Third, an indication for CT-guided lung biopsy was at the discretion of the attending physician. This was anticipated that frail elderly individuals at high risk of developing adverse events were excluded from the examination from the outset, which may have influenced the incidence of adverse events. Fourth, at our hospital, two types of puncture needles are used; however, the choice of which to use is determined on the spot at the discretion of the attending physician, and the specific needle used is not recorded in the electronic medical record. Thicker needles improve diagnostic rates but increase the likelihood of adverse events, whereas thinner needles have the opposite effect. The absence of a standardised protocol for needle selection, leaving it to the attending physician's discretion, may influence both diagnostic rates and the incidence of adverse events. Similarly, the number of punctures performed is also not recorded in the electronic medical record. Consequently, in this retrospective study, we were unable to collect data on these two items and thus could not analyse them. Fifth, several adverse events (eg, alveolar haemorrhage) have not been counted as adverse events.
Conclusion
In this single-centre retrospective cohort, incidence of adverse events and diagnostic accuracy by CT-guided lung biopsy did not significantly differ between patients aged ≥75 years and younger patients. Age alone should therefore not be considered a contraindication, although careful attention to lesion location and underlying lung disease remains crucial.
Footnotes
ORCID iDs
Ethical Approval
This clinical study was approved by the National Hospital Organization Kyoto Medical Center Institutional Review Board (approval number: 24-025).
Informed Consent
This was a retrospective study, and no consent was obtained from the patients. Instead, an opt-out method was used, which guaranteed the right of the participants to refuse to participate in the study.
Authors’ Contributions
OK and KF designed the study, gathered information. SY drafted the manuscript. OK and KF revised the manuscript. NF, YO, ST, TI, TI, IO and KT supervised the study design and revised the manuscript. All the authors performed computed tomography-guided lung biopsy or drainage and collected relevant information. All the authors have read and approved the final version of the manuscript.
Funding
This study was supported in part by a grant from the National Hospital Organization's fiduciary funds (for English editing).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
The data that support the findings of this study are available from the NHO Kyoto Medical Center Ethical Committee, but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. Data are however available from the authors upon reasonable request and with permission of the NHO Kyoto Medical Center Ethical Committee.