
Abstract
Objective
This study evaluated the clinical efficacy and safety of simultaneous integrated boost (SIB) followed by selective sequential boost radiotherapy (RT) in patients with spinal metastases (SM) and explored the protocol's potential for dosimetric optimization.
Methods
In this retrospective study, 34 consecutive patients with SM underwent SIB followed by selective sequential boost RT at Peking University Third Hospital between July 2021 and December 2024. Prescribed doses were 30 Gy in 10 fractions to the planning target volume (PTV), with dose escalation to the boost planning target volume (PTV_boost) of either 40 Gy in 10 fractions or 48 Gy in 12 fractions. The primary endpoints included pain relief (Numerical Rating Scale), neurological improvement (Frankel Grade), and adverse events (RTOG/EORTC criteria). Secondary endpoints comprised local control rate (LCR), evaluated by MRI or CT, and cancer-specific survival (CSS).
Results
The median follow-up was 9.9 months (range: 3.4-44.3 months), and 26 of 34 patients reported pain before treatment; of these, 84.6% (22/26) experienced pain relief (30.8% complete, 53.8% partial). Neurological function improved in 72.7% (16/22) of affected patients, with complete improvement in 27.3% and partial improvement in 45.5%. The majority of adverse events were grade 1–2 and resolved following appropriate symptomatic management. Kaplan–Meier analysis showed LCRs of 97.1%, 90.2%, 90.2%, and 90.2% at 3, 6, 12, and 24 months, respectively, and CSS rates of 97.0%, 97.0%, 87.0%, and 56.8% at the corresponding intervals.
Conclusions
Individualized dose-escalation RT may be a promising treatment for SM, potentially delivering significant pain relief, neurological recovery, and durable local tumor control, all while maintaining strict dosimetric constraints for organs at risk. Further prospective multicenter trials are essential to validate its safety and efficacy.
Keywords
Introduction
The spine is among the most common sites for metastasis in cancer patients, with approximately 40%–70% of patients with advanced malignancies developing spinal metastases (SM).1,2 The likelihood of metastasis varies by spinal segment: the cervical spine accounts for less than 10%, the thoracic spine 60%–80% and the lumbar spine 15%–30%. 3 The most common primary sources of SM are malignancies arising in the prostate, breast, lung, kidney, and gastrointestinal tract.1,4 Advances in early tumor detection and comprehensive treatment strategies have significantly extended overall survival (OS) in cancer patients, consequently leading to a yearly rise in SM incidence. 4 SM is often accompanied by severe pain, metastatic spinal cord compression (MSCC), hypercalcemia, and pathological fractures, all of which significantly impair patients’ quality of life.5,6 Therefore, optimizing treatment strategies for SM—to alleviate symptoms, improve local tumor control, and minimize treatment-related toxicity—has become a pressing clinical challenge. Currently, the primary treatment modalities for SM include surgery, radiotherapy (RT), and drug therapy.7-9 Regarding the optimal RT fractionation regimen for SM, no international consensus has yet been reached. 10 The American Society for Radiation Oncology recommends several fractionation regimens, including 8 Gy in a single fraction, 20 Gy in 5 fractions, 24 Gy in 6 fractions, and 30 Gy in 10 fractions. 11 Conventional external beam radiotherapy (cEBRT) and stereotactic body radiotherapy (SBRT) are the main RT modalities in clinical practice. 12 SBRT, a high-precision, high-dose conformal RT technique, delivers substantial doses (8-24 Gy per fraction) to the tumor region over fewer fractions while sparing organs at risk (OARs), thereby achieving favorable local symptom control.13,14 However, the indications for SBRT in SM remain controversial, and standardized patient selection criteria have yet to be established. 15 The RTOG 0631 trial recommends SBRT for patients with metastatic lesions located at least 3 mm from the spinal cord, thereby ensuring spinal cord safety when administering high single-fraction doses. Whether SBRT is appropriate for multi-segment or larger-volume SM remains to be further investigated. 16 Although SBRT improves local symptom control, its impact on prolonging OS remains uncertain. In contrast, cEBRT delivers lower per-fraction doses across numerous sessions, gradually accumulating the dose to effectively control the tumor. Given the lower in-field recurrence rates observed with cEBRT, current international clinical practice tends to favor multi-fraction RT.17,18 The widely used 30 Gy/10-fraction regimen achieves approximately 60%–70% pain control at three months, underscoring the need for further optimization.19,20 Recent RT advances have prompted dose-escalation studies aimed at relieving local symptoms and improving patient outcomes. 21 Among these strategies, simultaneous integrated boost (SIB) and sequential boost (SEQ) are two widely adopted approaches that have demonstrated both feasibility and therapeutic efficacy across a range of tumor types.
Based on extensive clinical experience and research at our radiation oncology center, we have explored an individualized dose-escalation RT protocol for SM using a combination of SIB and SEQ techniques. The protocol delivers 30 Gy in 10 fractions (3 Gy/fx; BED₁₀ = 39 Gy) to the planning target volume (PTV), while a SIB delivers 40 Gy in 10 fractions (4 Gy/fx; BED₁₀ = 56 Gy) to the boost planning target volume (PTV_boost). Depending on patient-specific factors, two additional 4 Gy fractions may be delivered sequentially, escalating the total dose to the PTV_boost to 48 Gy in 12 fractions (4 Gy/fx; BED₁₀ = 67.2 Gy). This study aims to comprehensively evaluate the efficacy and safety of this approach, with the objectives of establishing an optimized precision RT protocol for SM and informing evidence-based clinical guidelines.
Materials and Methods
Clinical Data
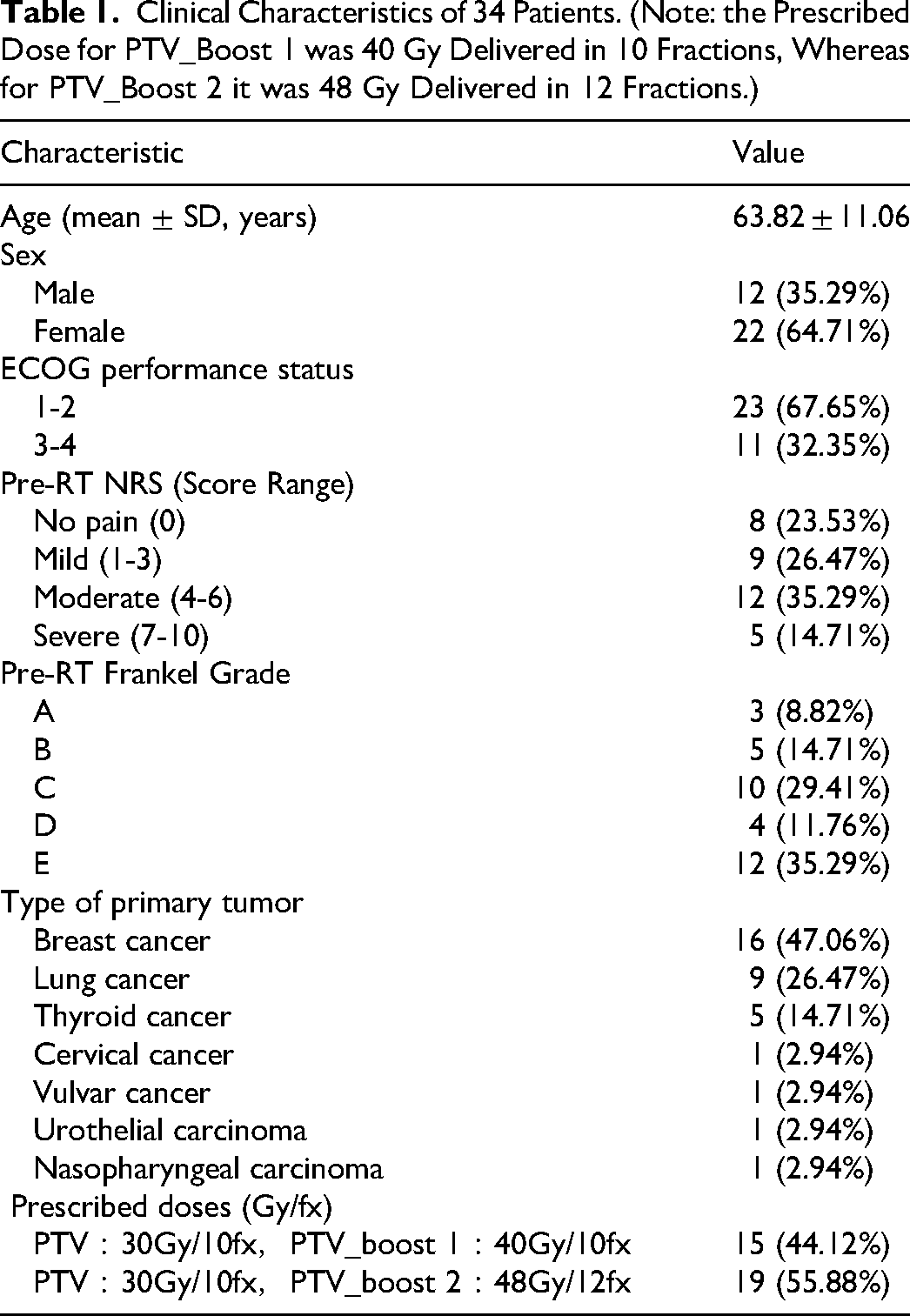
This retrospective study, conducted in compliance with the STROBE guidelines for reporting observational research, 22 included 34 consecutive patients with SM who underwent individualized dose-escalation RT at the Department of Radiation Oncology of Peking University Third Hospital from July 1, 2021, to December 20, 2024. Of these patients, 15 received 30 Gy in 10 fractions to the PTV and 40 Gy in 10 fractions to the PTV_boost, while 19 received 30 Gy in 10 fractions to the PTV and 48 Gy in 12 fractions to the PTV_boost. Data collection was completed on March 20, 2025, to maintain consistency and integrity in the study timeline. The treatment protocol was developed by a multidisciplinary team comprising radiation oncologists, orthopedic surgeons, radiologists, medical oncologists, pathologists, and nuclear medicine specialists. Key inclusion criteria were: (1) histologically confirmed solid malignancies with SM verified by CT, MRI, or PET–CT; (2) life expectancy greater than six months based on the Tokuhashi score; (3) presence of a metastatic lesion within 3 mm of the spinal cord, involvement of three or more consecutive vertebrae, large tumor volume, or other factors precluding SBRT; and (4) signed informed consent. Exclusion criteria included: (1) spinal instability requiring prior fixation; (2) primary non–solid malignancies; and (3) incomplete RT. Patients were followed up for 3.4 to 44.3 months (median, 9.9 months). Baseline characteristics are detailed in Table 1. All patient data were fully de-identified prior to analysis to ensure patient anonymity and data confidentiality. This study was approved by the Ethics Committee.
Clinical Characteristics of 34 Patients. (Note: the Prescribed Dose for PTV_Boost 1 was 40 Gy Delivered in 10 Fractions, Whereas for PTV_Boost 2 it was 48 Gy Delivered in 12 Fractions.)
Methods
Positioning, Delineation of OARs and Target Volumes
All patients were positioned supine with a supportive headrest for cranial stabilization. Site-specific immobilization devices were employed: an S-type head-neck-shoulder mask secured cervical lesions, while low-temperature thermoplastic mesh and carbon fiber baseplates stabilized the thoracic, lumbar, and sacral regions. Vacuum cushions supplemented positioning for patients with reduced immobilization capacity. Simulation imaging utilized a Philips Brilliance 16-slice large-bore (85 cm) CT scanner, with contrast-enhanced protocols applied unless contraindicated by severe allergies or renal impairment. The scan coverage extended ≥10 cm beyond lesion margins in both craniocaudal directions, acquired at 5-mm slice intervals. A laser-guided crosshair system ensured reproducible alignment between simulation and treatment setups. Digital Imaging and Communications in Medicine (DICOM) datasets were imported into the treatment planning system (TPS), supplemented by MRI fusion for enhanced anatomical definition. To ensure consistent delineation of target volumes and OARs, all contours were generated following a standardized protocol. Developed by our Spinal Metastases Radiation Oncology team, this protocol follows the International Commission on Radiation Units and Measurements (ICRU) recommendations. Participating radiation oncologists received regular training and adhered strictly to the established protocol. All contours underwent independent review and approval by senior radiation oncologists before treatment delivery, ensuring accuracy, reproducibility, and adherence to protocol-defined standards. The gross tumor volume (GTV) encompassed all tumors visible on CT/MRI. The clinical target volume (CTV) encompassed the GTV plus regions at risk for subclinical disease spread. If any part of the vertebral body, pedicle, transverse process, lamina, or spinous process was involved by the GTV, the entire corresponding anatomical structure was included in the CTV. Circumferential CTVs encasing the spinal cord were avoided unless the vertebral body, bilateral pedicles or laminae, spinous process, or extensive epidural disease were involved. The PTV and PTV_boost were generated by applying a 5-mm isotropic margin to the CTV and GTV, respectively. In regions where the PTV was in close proximity to the spinal cord, a selective inward retraction of 3–4 mm was applied to minimize radiation exposure to the spinal cord (Figures 1 and 2). The dose constraints for OARs were defined as follows: spinal cord Dmax < 40 Gy; esophagus Dmean < 34 Gy and V30 < 50%; trachea Dmax < 40 Gy; heart Dmean < 26 Gy and V25 < 10%; lung V20 ≤ 10%; liver Dmean < 30 Gy and V30 < 50%; kidneys Dmean < 15 Gy; stomach, small bowel, and colon Dmax < 20 Gy and V15 < 120 cc; and rectum and bladder Dmax < 20 Gy and V30 < 50%. Dose constraints were individually adjusted based on the anatomical location of each lesion.

VMAT-Based Dose Distribution in a Thoracic Vertebral Metastasis. (Prescription: 30 Gy to PTV; 40 Gy to PTV_boost. A: Axial; B: Coronal; C: Sagittal).

Dose-Volume Histogram of the Planning Target Volume in a Thoracic Vertebral Metastasis Treated with VMAT.
Radiation Therapy Planning and Delivery
The individualized dose-escalation regimen was delivered via volumetric modulated arc therapy (VMAT). The prescribed doses were 30 Gy in 10 fractions (3 Gy per fraction; BED₁₀ = 39 Gy) to the PTV, with dose escalation to the PTV_boost of either 40 Gy in 10 fractions or 48 Gy in 12 fractions. After the initial 10 fractions, a multidisciplinary panel of at least three radiation oncologists performed a comprehensive evaluation based on five criteria: (1) clinical response, including pain relief and/or neurological improvement; (2) treatment tolerance, assessed via acute toxicities to the spinal cord and other OARs, hematologic parameters, and performance status; (3) dosimetric feasibility, defined as ≥5 mm of separation between the PTV_boost and the spinal cord; (4) documented informed consent detailing potential risks and benefits; and (5) safety monitoring, whereby new acute toxicities or clinical deterioration prompted treatment modification or discontinuation. Patients meeting all criteria received two additional 4 Gy fractions to the PTV_boost, escalating the total dose from 40 Gy to 48 Gy. All plans underwent dosimetric verification, ensuring a gamma pass rate ≥95% (3%/2 mm criteria). Treatments were delivered once daily (5 fractions/week). Daily cone-beam CT (CBCT) was used to guide setup corrections via bony anatomy alignment. Offline adaptive replanning was performed whenever significant anatomical changes (eg, weight loss altering body contour) or technical deviations (eg, inadequate immobilization causing setup inaccuracies) were detected during treatment.
Follow-up and Clinical Evaluation Criteria
Patient evaluation protocol: Pre- and post-RT assessments included monitoring of pain relief, neurological function improvement, acute/chronic RT-related toxicities, local control rates (LCR), and cancer-specific survival (CSS). Evaluations were conducted at the following time points: pre-RT, upon RT completion, and 1 month post-RT, with subsequent assessments every 3 months until 12 months post-treatment. After the 12-month mark, assessments were performed every 6 months.
Pain response evaluation: Pain relief was assessed using the Numerical Rating Scale (NRS) ranging from 0 to 10, where 0 indicated no pain; 1–3 indicated mild pain (tolerable with no interference in daily activities); 4–6 indicated moderate pain (persistent and causing sleep disturbances); and 7–10 indicated severe pain (associated with autonomic dysfunction or restricted mobility). On the first day of RT, before treatment, patients underwent an NRS pain assessment, and their use of analgesic medications was documented. Pain response was assessed based on the following criteria: Complete pain relief (CR-P) was defined as a NRS score of 0 with no increase in the analgesic dose. Partial pain relief (PR-P) was defined as either a reduction of ≥2 points in the NRS score at the treatment site compared to baseline, without an increase in daily analgesic consumption, or a reduction of ≥25% in analgesic consumption without an increase in the NRS score. Pain progression (PP-P) was defined as either an increase of ≥2 points in the NRS score at the treatment site compared to baseline, while daily analgesic consumption remained stable, or an increase of ≥25% in daily analgesic consumption when the NRS score at the treatment site was either stable or had increased by 1 point relative to baseline. Nonresponse (NR) referred to cases that did not meet the evaluation criteria for CR-P, PR-P, or PP-P. 23 Overall pain responder rate (ORR-P) was calculated as the sum of CR-P and PR-P.
Neurological function response evaluation: The Frankel grading system was utilized, where Grade A signified a complete loss of function below the injury level; Grade B denoted sensory preservation without motor function; Grade C indicated non-functional motor preservation (muscle strength ≤2); Grade D represented functional motor preservation (muscle strength ≥3); and Grade E reflected normal neurological function. Complete neurological function recovery (CR-N) was defined as achieving a post-RT Frankel grade of E, with MRI confirmation of complete spinal cord decompression. Partial neurological function recovery (PR-N) was defined as an improvement of at least one Frankel grade, while no neurological function response (NR) was defined as the absence of any change from the pre-treatment Frankel grade. Neurological function progression (PP-N) was defined as a deterioration of at least one Frankel grade, and overall neurological function responder rate (ORR-N) was calculated as the sum of CR-N and PR-N.
Adverse effects were assessed in accordance with RTOG/EORTC criteria.
Local tumor response evaluation: The initial imaging assessment (CT/MRI) was conducted one month following RT, with subsequent evaluations every three months up to 12 months post-treatment. Beyond 12 months, clinical examinations and imaging assessments were performed every six months. Local tumor response to RT was rigorously evaluated using RECIST 1.1 criteria: Complete response (CR) was defined as the complete disappearance of all target lesions that received RT, confirmed at least 4 weeks apart; partial response (PR) as a reduction of at least 30% in the sum of the longest diameters of target lesions from baseline, confirmed at least 4 weeks apart; progressive disease (PD) as an increase of at least 20% in the sum of the longest diameters of target lesions or the appearance of new lesions; and stable disease (SD) as any change in the sum of the longest diameters of target lesions that did not meet the criteria for PR or PD. Non-tumor-related deaths and patients alive at the end of the study were considered right-censored.
Statistical Methods
Descriptive analyses were performed to evaluate pain relief, neurological function improvements, and RT-related toxicities. LCR and CSS were estimated using the Kaplan–Meier method. All statistical analyses were performed with SPSS Statistics version 24.0 (IBM Corp., Armonk, NY, USA).
Results
Pain Response Evaluation
Among the 34 patients with SM included in this study, 76.47% (26/34) reported cancer-related pain the pre-RT, with baseline pain intensity, assessed using the NRS, ranging from 1 to 10 (median score: 4), as detailed in Table 2. When stratified by pain intensity, the mild pain group (NRS 1-3; 9 cases) exhibited a CR-P rate of 55.56% (5/9) and a PR-P rate of 44.44% (4/9), with no cases of non-improvement or worsening observed. In the moderate pain group (NRS 4-6; 12 cases), the CR-P and PR-P rates were 25.00% (3/12) and 58.33% (7/12), respectively, while 16.67% (2/12) of patients showed no improvement. In the severe pain group (NRS 7-10; 5 cases), no CR-P was achieved; however, a PR-P was observed in 60.00% (3/5) of patients, while 40.00% (2/5) showed no improvement. The ORR-P, defined as the sum of CR-P and PR-P, was 84.62% (22/26), with a CR-P rate of 30.77% (8/26) and a PR-P rate of 53.85% (14/26). Most patients began to experience pain relief within 1–2 weeks following RT, and no cases of pain exacerbation were observed throughout the entire follow-up period.
Association Between pre-RT NRS Scores and Pain Response at Last Follow-up.

Neurological Function Response Evaluation
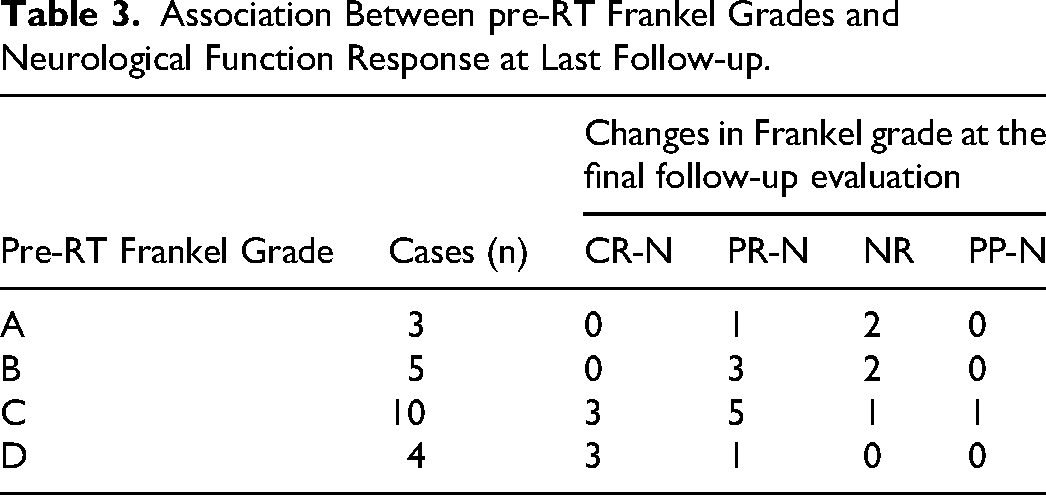
Among the 34 patients in this study, 64.71% (22/34) presented with neurological deficits (Frankel grades A–D) prior to RT, as shown in Table 3. Prior to RT, the Frankel grading was predominantly Grade C (10 cases, 45.45%), followed by Grade B (5 cases, 22.73%), Grade D (4 cases, 18.18%), and Grade A (3 cases, 13.64%). At the final follow-up of patients with baseline Frankel Grade A (3 cases), CR-N was not observed in any patient; PR-N was achieved in 33.33% (1/3) of cases, while 66.67% (2/3) remained at their baseline status. Among Frankel Grade B patients (5 cases), no CR-N was documented; however, PR-N was observed in 60.00% (3/5) of cases, with 40.00% (2/5) remaining unchanged. Among Frankel Grade C patients (10 cases), CR-N was achieved in 30.00% (3/10) of cases, PR-N in 50.00% (5/10), NR in 10.00% (1/10), and PP-N in 10.00% (1/10). Among Frankel Grade D patients (4 cases), CR-N occurred in 75.00% (3/4) of cases and PR-N in 25.00% (1/4), with no cases of regression observed. The ORR-N was 72.73% (16/22), comprising a CR-N rate of 27.27% (6/22) and a PR-N rate of 45.45% (10/22). By the end of the follow-up period, one patient experienced neurological function deterioration, with the Frankel grade declining from C to B. Most patients began to experience neurological function improvement within 2–8 weeks following RT.
Association Between pre-RT Frankel Grades and Neurological Function Response at Last Follow-up.
Adverse Effects
This study performed an analysis of radiation-induced toxicity patterns across different spinal regions. The actual doses received by target volume and some OARs are detailed in Table 4. In the cervical spine group (n = 8), the most common toxicities were radiation dermatitis (Grade 1-2 in 6 cases, including 5 cases of Grade 1 and 1 case of Grade 2, with no cases ≥ Grade 3) and mucositis (Grade 1-2 in 5 cases, Grade 3 in 1 case). Upper gastrointestinal (GI) reactions (Grade 1 in 4 cases, with no reactions ≥ Grade 2) and myelosuppression (Grade 1-2 in 5 cases, Grade 3-4 in 2 cases) were observed. In the thoracic spine group (n = 16), myelosuppression was the most notable toxicity (Grade 1-2 in 10 cases, Grade 3-4 in 3 cases). Other significant reactions included radiation dermatitis (Grade 1-2 in 10 cases), radiation esophagitis (Grade 1 in 5 cases), and 1 case of radiation pneumonitis (Grade 1). In the lumbar spine group (n = 5), the toxicities were relatively mild, with Grade 1 radiation dermatitis in 3 cases, Grade 1-2 lower GI toxicity in 2 cases, and myelosuppression (Grade 1-2 in 3 cases, Grade 3 in 1 case). In the sacral spine group (n = 2) and the double-region vertebral metastasis group (n = 3), all toxic reactions were Grade 1-2. Details are provided in Table 5.
Prescribed Dose Objectives and Actual Delivered Doses for PTV, PTV_Boost 1 (4 Gy × 10), PTV_Boost 2 (4 Gy × 12), and Selected OARs.

Distribution of Toxicity Grades for Radiation-Induced Adverse Effects Across Spinal Regions.

Local Control and Survival Analysis
The follow-up period concluded on March 20, 2025. A total of 34 patients with SM were enrolled in this study, with a median follow-up of 9.9 months (range, 3.4-44.3 months). During the follow-up, three instances of local progression were observed: one lung cancer case, one thyroid cancer case, and one breast cancer case post-RT. Kaplan–Meier analysis demonstrated LCRs of 97.06%, 90.19%, 90.19%, and 90.19% at 3, 6, 12 and 24 months, respectively. Survival analysis revealed that seven patients had died by the end of the follow-up period. Among these, six patients—three with lung cancer, and one each with breast cancer, nasopharyngeal carcinoma, and thyroid cancer—died from cachexia or organ failure secondary to tumor progression, while one lung cancer patient succumbed to COVID-19 infection. No treatment-related deaths were observed. The CSS rates were 96.97%, 96.97%, 86.96% and 56.83% at 3, 6, 12 and 24 months, respectively.
Discussion
The management of SM focuses on achieving symptom relief, preserving neurological function, maintaining spinal stability, controlling local tumor progression, and ultimately improving quality of life. To address these clinical priorities, we explored an innovative individualized dose-escalation RT strategy that employs optimized dose-gradient protocols. Specifically, the PTV receives 3 Gy per fraction over 10 fractions (BED₁₀ = 39 Gy), while the PTV_boost receives either 4 Gy per fraction over 10 fractions (BED₁₀ = 56 Gy) or 4 Gy per fraction over 12 fractions (BED₁₀ = 67.2 Gy). This study comprehensively evaluates the clinical efficacy of individualized dose-escalation RT in terms of pain relief, neurological function recovery, RT-related adverse events, LCR, and CSS.
RT has been demonstrated to promote the reossification of metastatic bone lesions, as the increased bone mineral density is generally associated with lesion healing. This process is considered conducive to enhancing spinal stability, thereby supporting long-term pain management.24,25 He et al demonstrated that, compared with the standard 30 Gy/10-fraction regimen, a dose-escalated, image-guided intensity-modulated radiotherapy (IG-IMRT) protocol of 60–66 Gy in 20–30 fractions significantly improved pain relief rates in SM patients (1-month: 73.69% vs 34.29%, P = .006; 3-month: 73.69% vs 41.38%, P = .028). 26 Our study observed an 84.62% (22/26) ORR-P following RT, exceeding the 60%–70% efficacy observed with cEBRT, while demonstrating analgesic outcomes comparable to those reported in some SBRT studies.20,27-31 The superior efficacy of our protocol may be attributed to dose escalation strategies targeting the PTV_boost, delivering a BED₁₀ of either 56 Gy or 67.2 Gy. Notably, 16.0% of patients failed to achieve adequate pain relief, highlighting the need for a multifactorial analysis that considers tumor biology, lesion topography, and individual radiosensitivity. However, considerable controversy remains regarding the relationship between dose escalation and analgesic efficacy. The RTOG 94-17 trial demonstrated comparable 3-month pain relief rates between a single-fraction 8 Gy regimen (70%) and a multifraction 30 Gy/10-fraction regimen (62%) (P = .59). 32 The RTOG 0631 trial demonstrated inferior 3-month analgesic efficacy with stereotactic radiosurgery (16-18 Gy single-fraction) compared to cEBRT (8 Gy single-fraction) in patients with SM (41.3% vs 60.5%). 16 Emerging evidence indicates that dose intensification may not inherently improve analgesic efficacy and could paradoxically disrupt pain modulation pathways, 33 thereby underscoring the complexity of clinical management in SM.
Numerous studies have examined neurological outcomes after RT for MSCC. A retrospective analysis of re-irradiation with SBRT (25 Gy in 5 fractions) reported a 53% neurological improvement rate (8 of 15 patients). 34 In Ryu et al's study, patients with mild spinal cord compression were treated using a single SBRT fraction of 12–20 Gy, achieving an 81% neurological improvement rate. 35 Rades et al analyzed 504 breast cancer patients with MSCC treated with RT, reporting that 34% had motor improvement, 56% had no change, and 10% experienced deterioration. 36 Our study demonstrates the clinical efficacy of the individualized dose-escalation RT regimen, achieving a neurological function ORR-N of 72.73%, including a PR-N rate of 45.45% and a CR-N rate of 27.27%. Although CR-N was not attained in some patients, symptom reduction significantly improved daily functionality and quality of life. Notably, 27.27% of patients showed no neurological improvement; among these, three individuals with pre-existing paralysis failed to regain ambulatory function, likely attributable to irreversible neuronal damage from chronic spinal cord compression. One patient experienced neurological function deterioration, declining from Frankel Grade C to B, associated with rapid tumor progression. These outcomes underscore the multifactorial determinants of neurological function recovery, including tumor aggressiveness, baseline neurological deficits, individual variability, and comorbidities, underscoring the need for personalized therapeutic strategies—particularly in high-risk populations. However, our study employed the Frankel grading system to evaluate both motor and sensory functions, whereas Rades et al study focused solely on motor function. Future prospective, multicenter, randomized cohort studies employing standardized assessment protocols are warranted to elucidate the differential impacts of various RT regimens on neurological function recovery.
Extensive international studies have investigated the therapeutic efficacy of various dose fractionation regimens. A large-scale retrospective analysis by Rades et al evaluated 1304 patients with MSCC treated with RT. Participants were stratified into five cohorts based on fractionation schemes: 1 × 8 Gy (n = 261), 5 × 4 Gy (n = 279), 10 × 3 Gy (n = 274), 15 × 2.5 Gy (n = 233), and 20 × 2 Gy (n = 257). All regimens demonstrated comparable tolerability, with no statistically significant differences in post-treatment ambulatory function improvement or preservation of walking capacity across groups (P > .05). However, significant variations emerged in 2-year in-field recurrence rates—24%, 26%, 14%, 9%, and 7% for the respective cohorts (P < .01)—with the latter three fractionation schedules (10 × 3 Gy, 15 × 2.5 Gy, and 20 × 2 Gy) exhibiting superior local control. 17 Similarly, Rades et al conducted a comparative analysis of radiation regimens in 159 patients with oligometastatic breast cancer-related MSCC, evaluating three therapeutic approaches: 1 × 8 Gy/5 × 4 Gy (n = 60), 10 × 3 Gy (n = 40), and 15 × 2.5 Gy/20 × 2 Gy (n = 59). The study demonstrated that higher radiation doses significantly enhanced local control, offering critical insights for optimizing dose selection in the palliative RT management of MSCC. 37 In a prospective, nonrandomized trial, Rades et al compared short-course RT (1 × 8 Gy or 5 × 4 Gy) with long-course regimens (10 × 3 Gy, 15 × 2.5 Gy, or 20 × 2 Gy), reporting 1-year LCR of 61% versus 81% (P = .005). 18 In a retrospective matched-pair analysis, patients treated with 15 × 2.5 Gy or 20 × 2 Gy had superior 2-year local control (92% vs 71%; P = .012), progression-free survival (90% vs 68%; P = .013), and OS (68% vs 53%; P = .032) compared to those receiving 10 × 3 Gy. These findings suggest that in patients with favorable prognoses, dose-fractionation escalation significantly improves tumor control and survival outcomes. 38 A multicenter study by Chang et al, involving 60 patients (72 SM) treated with SBRT (median dose of 24 Gy), reported 1- and 2-year OS rates of 90% and 76%, respectively. 39 In this study, we evaluated clinical outcomes in SM patients treated with the individualized dose-escalation RT protocol. The observed LCRs at 3, 6, 12, and 24 months post-treatment were 97.06%, 90.19%, 90.19%, and 90.19%, respectively. The corresponding CSS rates were 96.97%, 96.97%, 86.96%, and 56.83%, respectively. These results indicate that individualized dose-escalation RT provides durable local tumor control in SM, with LCR comparable to or exceeding previous reports. Although CSS rates declined over time, this trend likely reflects the systemic progression of SM, where OS is predominantly determined by systemic disease status. Nevertheless, localized intensified RT plays a crucial role in maintaining quality of life by effectively controlling local disease progression. Overall, the individualized dose-escalation RT regimen offers an effective and feasible treatment option for SM patients, balancing therapeutic efficacy and safety.
Regarding the toxicity profiles of different treatment regimens, cEBRT is generally well tolerated, with common acute reactions such as mild dermatitis and mucositis. Advanced techniques such as intensity-modulated radiotherapy (IMRT) and VMAT enable precise spinal cord dose control, minimizing the risk of severe injury. In the RAMSES-01 study, treatment regimens of 15 × 2.633 Gy or 18 × 2.333 Gy resulted in only 4% of patients experiencing grade 3 adverse events. No late toxicities were reported. 40 However, SBRT, due to its high single-dose delivery, requires careful monitoring for bone-related complications. The literature reports vertebral compression fracture rates ranging from 4% to 39% after SBRT, necessitating strict limits on the maximum spinal cord dose and vertebral exposure volume. 41 In this study, most adverse reactions were mild to moderate; however, six patients experienced grade 3–4 myelosuppression (four grade 3 and two grade 4). Further analysis revealed that all six patients underwent concurrent chemotherapy during RT, suggesting that the hematologic toxicity was likely related to the combined regimen. Treatment-related toxicities were effectively managed with symptomatic and supportive care. The actual spinal cord doses delivered to the 34 patients were 29.60 ± 3.58 Gy (mean ± SD; range, 11.20 - 32.54 Gy). By the end of follow-up, no severe late-onset radiation-related complications—such as pathological fractures, radiation-induced myelitis, or osteonecrosis—occurred.
With advancements in surgical techniques and expanded multidisciplinary collaboration, surgical treatment strategies for SM have been continually refined. The surgical objectives include stabilizing the spine compromised by mechanical instability, decompressing the spinal cord, and resecting epidural lesions to improve subsequent RT outcomes.42,43 The choice of surgical approach is determined by multiple factors, including tumor invasiveness, the extent of spinal segment involvement, the degree of cord compression, patients’ life expectancy, physical condition, and individual preferences. Current surgical options include palliative decompression, separation surgery, vertebroplasty, en bloc or partial spondylectomy, and various minimally invasive techniques. Despite ongoing advancements in RT, surgical intervention remains indispensable. Surgical objectives have evolved from basic decompression and stabilization to a synergistic integration with RT. Separation surgery involves resecting the tumor component that compresses the spinal cord, thereby decompressing both the spinal cord and nerve roots while establishing a safe margin between the tumor and adjacent neural structures for subsequent RT. Postoperatively, high-dose precision RT is administered to the residual tumor without compromising neurological function, thereby minimizing radiation-induced damage to the spinal cord and nerves, and ultimately reducing the risk of local tumor recurrence. 44 Additionally, radiofrequency ablation (RFA) has garnered increasing attention as an option for managing metastatic spinal pain. A systematic review of 15 studies demonstrated that RFA significantly reduced pain scores while enhancing functional status and quality of life over a short-term follow-up period (3-6 months). 45 Minimally invasive techniques are pivotal in managing SM, offering benefits such as small incisions, minimal blood loss, rapid postoperative recovery, and low complication rates.46-48 The integration of these technologies provides patients with more personalized and precise therapeutic options. Clinical findings confirm that a multimodal approach combining separation surgery, RFA, and cement augmentation for thoracolumbar metastases offers synergistic therapeutic benefits, including effective pain relief, restoration of neurological function, improved mobility, and enhanced daily activities, achieved through a patient-centered strategy. 49
Revolutionary advances in systemic therapies, particularly targeted agents and immunomodulatory approaches, have revitalized multimodal treatment paradigms. Preclinical studies have shown that osimertinib promotes regression of bone metastases and restores skeletal integrity in EGFR-mutant murine models, an effect associated with improved long-term survival. 50 Clinical validation by Kanaoka et al has demonstrated the efficacy of osimertinib in reducing tumor burden in lung cancer patients with bone metastases, achieving an ORR of 82%. 51 Likewise, Miyagi reported a 94% ORR and evidence of osteosclerotic remodeling in lung cancer patients with osseous metastases treated with gefitinib. 52 In renal cell carcinoma, Park et al identified a synergistic therapeutic effect between RT and targeted therapies, with the combination group exhibiting a significantly higher 1-year local progression-free rate (LPFR) than RT alone (P = .019). 53 Advances in immuno-oncology continue to broaden therapeutic horizons. Immune checkpoint inhibitors (ICIs), such as pembrolizumab, nivolumab, and atezolizumab, have shown clinically significant suppression of bone metastasis progression, achieving a 72.4% disease stabilization rate in advanced lung cancer. 54 Emerging evidence indicates a synergistic interaction between RANKL pathway modulation and ICIs, wherein RANKL inhibition enhances antitumor immunity while reducing skeletal-related events. 55 These advancements mark the emergence of precision multimodal therapies for SM, integrating molecular targeting, immunomodulation, and locoregional interventions.
Precision therapeutics for SM require personalized treatment regimens tailored to patient-specific characteristics in order to maximize both efficacy and safety. Treatment outcomes are influenced by both dose fractionation patterns and tumor histopathology. Substantial evidence highlights significant histology-dependent variations in radiotherapeutic response: radiosensitive tumors, such as prostate cancer and lymphoma, exhibit longer durations of local control compared with radioresistant subtypes, such as renal cell carcinoma. 56 A quantitative analysis by Gerszten et al reported 100% post-RT local control rates in breast and lung malignancies, whereas efficacy was lower in renal cell carcinoma (87%) and melanoma (75%). 27 Notably, although histopathological classification significantly influences therapeutic outcomes, existing data have not established a clear correlation between tumor biology and the optimal fractionation regimen. Anatomic tumor localization further influences therapeutic decision-making. Cervical spine irradiation presents a heightened risk of radiation-induced esophagitis due to anatomical constraints, whereas thoracic spine treatment is complicated by the potential for pulmonary toxicity. Critical weight-bearing regions, such as the lumbar and sacral spine, require careful consideration for both pain management and spinal cord protection. In clinical practice, it is essential to comprehensively integrate objective parameters—including primary tumor characteristics, extent of metastatic involvement, histopathological classification, and molecular characteristics. Equally important is the consideration of patients’ functional status, treatment goals, psychosocial factors, and pertinent local healthcare policies. Multidisciplinary teams should formulate personalized, evidence-informed precision treatment strategies to optimize clinical outcomes and long-term prognosis. 7
Conclusion
As an exploratory, single-arm study with a limited sample size, this investigation has inherent limitations. Nevertheless, preliminary findings suggest that individualized dose-escalation RT may effectively alleviate clinical symptoms in patients with SM, indicating a favorable balance between efficacy and safety. Future large-scale, multicenter, prospective randomized controlled trials are essential to validate the long-term efficacy and safety of this therapeutic approach and provide high-quality evidence to guide clinical decision-making and the optimization of personalized treatment strategies in this patient population.
Footnotes
Ethics Approval and Consent to Participate
The study was approved by the Research Ethics Committee of Peking University Third Hospital ((2025- Medical Ethics Review No. 347-01 and 347-02). The requirement for written informed consent was waived due to the retrospective nature of the study.
Authors’ Contributions
Software, Hui Xiao and Xiuwen Deng;
Formal analysis, Hui Xiao and Shuhua Wei;
Investigation, Hui Xiao, Qiman Han and Shuhua Wei;
Resources, Junjie Wang and Ping Jiang; data curation, Fuxin Guo and Nan Zhang;
Visualization, Ang Qu and Qiman Han;
Supervision, Junjie Wang and Chunxiao Li;
Project administration, Ping Jiang and Junjie Wang;
Funding acquisition, Shuhua Wei, Junjie Wang and Ping Jiang;
Validation, Hui Xiao, Fuxin Guo, Ang Qu, Nan Zhang, Shuhua Wei, Qiman Han, Xiuwen Deng, Chunxiao Li, Junjie Wang and Ping Jiang;
Writing—original draft preparation, Hui Xiao;
Writing—review and editing, Hui Xiao, Fuxin Guo Ang Qu, Nan Zhang, Shuhua Wei, Qiman Han, Xiuwen Deng, Chunxiao Li, Junjie Wang and Ping Jiang;
Approval of the final version, Hui Xiao, Fuxin Guo Ang Qu, Nan Zhang, Shuhua Wei, Qiman Han, Xiuwen Deng, Chunxiao Li, Junjie Wang and Ping Jiang.
All authors have agreed to be accountable for all aspects of the work by ensuring that any questions related to the accuracy or integrity of any part thereof are investigated and resolved appropriately.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China (82073335 to J.Wang), National Key Research and Development Program (2022YFC2404606 to P.Jiang), the Key Specialty program of Natural Science Foundation of Beijing Municipality (Z20008 to P.Jiang), Clinical scientist training program of Peking University (BMU2023PYJH009 to P.Jiang), Innovation and Translation project of Haidian District (HDCXZHKC2021215 to P.Jiang), the China Postdoctoral Science Foundation (2023M730124 to S.Wei), the Special Fund of National Clinical Key Specialty Construction Program of China (2021) and the Bethune Charitable Foundation (J202305E038 to P.Jiang).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of Data and Materials
All data are available in this manuscript.