
Abstract
Colorectal cancer (CRC) remains a formidable global health challenge, with the majority of patients exhibiting microsatellite stable (MSS) and proficient mismatch repair (pMMR) tumors that are largely unresponsive to immune checkpoint inhibitors (ICIs). The management of MSS/pMMR CRC remains a clinical challenge due to the intrinsic resistance to ICIs. The innovative strategy of combining cetuximab, an EGFR-targeting monoclonal antibody with immunomodulatory properties, offers a promising strategy to enhance the immunotherapeutic response in MSS/pMMR CRC. This combination therapy is rooted in the complementary therapeutic mechanisms of cetuximab and ICIs, which may synergistically improve overall response rates and durability of response. Although some preclinical and clinical data have suggested additional promising results, there are still some challenges and questions that need to be addressed. Further large-scale, randomized, phase III clinical trials are required to confirm the efficacy and safety of this combination therapy. The ongoing clinical trials evaluating the safety and efficacy of cetuximab-ICI combinations are eagerly anticipated to pave the way for a new era in personalized immunotherapy for MSS/pMMR CRC.
Keywords
Introduction
Colorectal cancer (CRC) remains a significant global health challenge and becomes the second leading cause of cancer-related deaths worldwide. 1 With an estimated median age of onset at 67 years, approximately 10% of patients experience the disease onset before the age of 50 years. 2 The 5-year survival rate for stage I CRC is > 90%, whereas it declines to 11%–15% for stage IV disease. 3 About 29% of patients with stage IV rectal cancer and 49% of those with stage IV colon cancer receive surgical treatment, often along with radiotherapy and/or chemotherapy. For unresectable stage IV CRC, treatment strategies may include an initial induction chemotherapy regimen followed by maintenance, continuation of the induction regimen, or observation. 4 Over the past several decades, advances in surgical approaches and precision medicine have greatly increased survival, even leading to long-term remission in some selected metastatic colorectal cancer(mCRC) patients who have tumors with specific molecular profiles (eg, microsatellite instability; KRAS/NRAS/BRAF wild-type tumors or those with BRAF V600E sequence variations).5,6 However, mCRC is an incurable disease in most cases, and the prognosis is still poor. 7 A personalized, comprehensive therapeutic strategy based on understanding the complex genetic and environmental bases of CRC is needed to achieve long-term control of the disease with better quality and quantity of life.
Current status of Immunotherapy in CRC
The journal Science named cancer immunotherapy as one of the top 10 breakthroughs of the year in 2013. 8 Due to the success of ICIs, immunotherapy has become a new mainstay of cancer treatment next to surgery, radiotherapy, chemotherapy, and targeted therapies. 9 ICIs such as programed cell death protein 1 (PD-1), programed cell death ligand 1 (PD-L1), and cytotoxic T lymphocyte antigen 4 (CTLA-4) have considerably improved the clinical benefit of various cancers by blocking immunoinhibitory signals and enabling an effective antitumor response in patients. 10 Le et al reported that immunotherapy resulted in a high overall remission rate (ORR) in MSI-high (MSI-H) CRC, which opened a new era of immunotherapy for CRC. 11 Subsequent studies, such as CheckMate-142, KEYNOTE-177 and KEYNOTE-164, explored the value of first-line and later-line treatment for deficient mismatch repair (dMMR) or MSI-H mCRC, respectively.12–14 The CheckMate-142 study enrolled 76% of patients with mCRC after progression of second- or later-line chemotherapy and/or targeted therapy, with ORR and disease control rate (DCR) up to 69% and 84%, respectively, and a complete remission rate of 13%. 12 The KEYNOTE-177 study, with a median follow-up of 32.4 months, showed that progression-free survival (PFS, 16.5 months vs 8.2 months) and quality of life were better in the pembrolizumab monotherapy group than in the chemotherapy group. 13 These significant research findings may be attributed to the fact that MSI-H/dMMR tumors exhibit a high neoantigen burden, which can trigger robust T cell activation. Upon activation, T cells upregulate PD-1 expression on their surface, and the subsequent interaction between PD-1 and PD-L1 on tumor cells results in the suppression of T cell function. The elevated mutational load and consequent immune activation likely render the tumor microenvironment (TME) more susceptible to PD-1 blockade, thereby promoting the recruitment of immune cells, such as T cells and dendritic cells, into the TME.15,16 Pembrolizumab enhances anti-tumor immune responses by effectively blocking the PD-1/PD-L1 pathway, which in turn increases immune cell infiltration within the tumor.17,18 Accordingly, the Food and Drug Administration(FDA)issued approval for pembrolizumab as the first-line treatment option for patients with MSI-H/dMMR mCRC. 19
However, despite the remarkable efficacy of immunotherapy in patients with MSI-H/dMMR mCRC, the population of patients with CRC who can benefit from immunotherapy is still very limited because patients with MSI-H/dMMR account for only 10%–15% of CRC cases. 20 Most CRCs (approximately 85%–90%) are characterized by MSS/pMMR status. In these patients, tumors with low numbers of neoantigens, low immune infiltration in the TME, and poor expression of major histocompatibility complex (MHC) molecules exhibit a lack of sensitivity to ICIs.20,21 Receiving immunotherapy as monotherapy is largely ineffective. 22 To date, the results of clinical trials with ICIs alone have been unsatisfactory with no approved agents for MSS/pMMR mCRC. The KEYNOTE-016 and KEYNOTE-028 included 18 and 22 patients with MSS mCRC, respectively, but almost no response to immunotherapy was observed.11,22 In addition, the antitumor effect of ICIs to these selected patients who initially respond to ICIs usually fail therapy because of acquired resistance. 23 Therefore, ways to improve the efficacy of the population with the MSS/pMMR status, which accounts for the majority of CRCs, along with immunotherapy-resistant patients with CRC are urgently required. Currently, many studies are investigating the use of combinations of ICIs with molecular targeting agents to transform the immune-exclusive TME of MSS/pMMR tumors.24–26 Among these strategies, immunotherapy in combination with cetuximab is one of the most promising approaches and may be a potential path toward treating MSS/pMMR CRC.
Mechanism and Application of Cetuximab in CRC
Cetuximab is a chimeric mouse-human immunoglobulin G (IgG) 1 monoclonal antibody (mAb), which can target the extracellular domain of the epidermal growth factor receptor (EGFR) and competitively inhibit the binding of EGFR to ligands such as epidermal growth factor, thus blocking the downstream signal transduction to exert antitumor effects. 27 Additionally, cetuximab is an immunomodulating agent that promotes T-cell infiltration into the CRC TME and upregulates ICIs. 28 The mechanisms of the anti-tumor effects of cetuximab are depicted in Figure 1, which mainly include: (1) Increased levels of cyclin-dependent kinase inhibitory proteins p21 and p27 and decreased levels of cyclin D1, inhibiting tumor cell proliferation, 29 (2) downregulated expression of the apoptosis suppressor B-cell lymphocyte-2 gene and upregulated expression of the proapoptotic Bcl-2-associated X protein gene, activating caspase-8 to induce apoptosis in tumor cells through the caspase cascade reaction, 30 and (3) simultaneous binding of cetuximab to the corresponding antigen via its allosteric fragment crystallizable (Fc) segment that binds to the Fc receptors of effector cells (such as natural killer [NK] cells, neutrophils, macrophages, and platelets) to kill tumor cells through antibody-dependent cell-mediated cytotoxicity (ADCC). 31

Mechanisms of Action of Cetuximab in Anti-Tumor Effects.
Due to the fact that combination therapy with cetuximab and chemotherapy in patients with RAS/BRAF wild-type (WT) mCRC can alleviate and stabilize the disease, improve PFS, ORR and overall survival (OS), it has been approved for clinical use as the standard first-line treatment for patients with RAS WT mCRC. 32 Nevertheless, cetuximab is effective only in a subset of CRCs. Approximately 45%–50% of patients with RAS-mutant (MUT) CRC do not benefit from the anti-EGFR therapy.33,34 Moreover, most patients with RAS WT CRC experience disease progression within 3-12 months after starting treatment with cetuximab. This progression is primarily due to the abnormal activation of downstream EGFR signaling pathways, including genetic alterations in components of the EGFR-RAS-RAF-MEK-MAPK pathway and amplification of receptor tyrosine kinases. 35 This could explain the ineffectiveness of anti-EGFR treatment in >70% of CRC cases. It has been shown that cetuximab has its clinical limitations and does not fully exert the immunomodulatory effect, especially in the induction of the ADCC response. 36 So how can we overcome the dilemma of primary and secondary drug resistance? The combination of cetuximab with ICIs might present innovative solutions.
Rationale for the Combination of Cetuximab and ICIs
Both combination therapies have shown promise individually but at the same time have limitations. The rationale behind combining targeted therapies and immunotherapies in cancer treatment is based on their complementary mechanisms of action and potential for synergistic interaction. 37 The exact mechanisms of the combination of cetuximab and ICIs are not completely understood, and the possible mechanisms are as follow: (1) Enhancing NK cell-mediated ADCC:Cetuximab effectively induces ADCC activity against various tumor cell lines in a manner dependent on EGFR expression levels, highlighting its potential to enhance NK cell-mediated cytotoxicity through high-affinity binding to the extracellular domain of EGFR, regardless of EGFR mutation status. 38 (2) Increasing expression of major histocompatibility complex (MHC) II:Cetuximab enhances the expression of MHCII molecules by recruiting T cells into the TME, thereby promoting an anti-tumor immune response. 39 (3) Facilitating the immunomodulatory effect of dendritic cells on cancer cells:Cetuximab facilitates the immunomodulatory effect of dendritic cells on cancer cells by enhancing the infiltration of immune cells (such as CD3+, CD8+, and CD56 + cells) into the tumor microenvironment, promoting inflammatory responses, and inducing immunogenic cell death, thereby augmenting anti-tumor immunity. 28 Over pass few years, preclinical studies have shown that cetuximab induces tumor-specific immune responses and immunogenic apoptosis, which is mediated by functional adaptive immunity. 40 The immune system can be able to play a critical role in modulating response to cetuximab in cancer. The ability of cetuximab to activate ADCC can lead to increased killing of EGFR + CRC cells. The immunological impact of cetuximab is noticeable irrespective of the presence of RAS/RAF gene mutations in CRC. 41 When cetuximab is administered in conjunction with immunotherapy, it has been demonstrated to facilitate the mobilization of T lymphocytes and NK cells to distant tumor locations. 42 Thus,induction of pro-inflammatory cytokines (ie, IFN-γ, TNFα) and cytotoxic T cells in the initiating TME may activate innate and adaptive immune responses.43,44 However, the intrinsic immune stimulation is followed by induction of immunosuppressive mechanisms, such as recruitment of Treg and MDSCs in TME and increased expression of PD-1, PD-L1 and CTLA-4 on tumor and immune cells.In other words,evidence in favor of these combination regimens,the synergy between cetuximab and ICIs may be based on a two-step process in which cetuximab contribute to new immune cells recruitment in TME and ICIs allow to disinhibit cells already present; Thus, they complement each other, this may lead to the creation of the most promising treatment to overcome resistance to ICIs in MSS/ pMMR CRC.45,46 Cetuximab in combination with ICIs could hold the key to improving ORRs and durability of response in challenging indications such as MSS/pMMR CRC. Mechanisms of synergy between cetuximab and ICIs in MSS/pMMR CRC is depicted in Figure 2. Further evidence from currently ongoing clinical trials that are evaluating this hypothesis is under way.
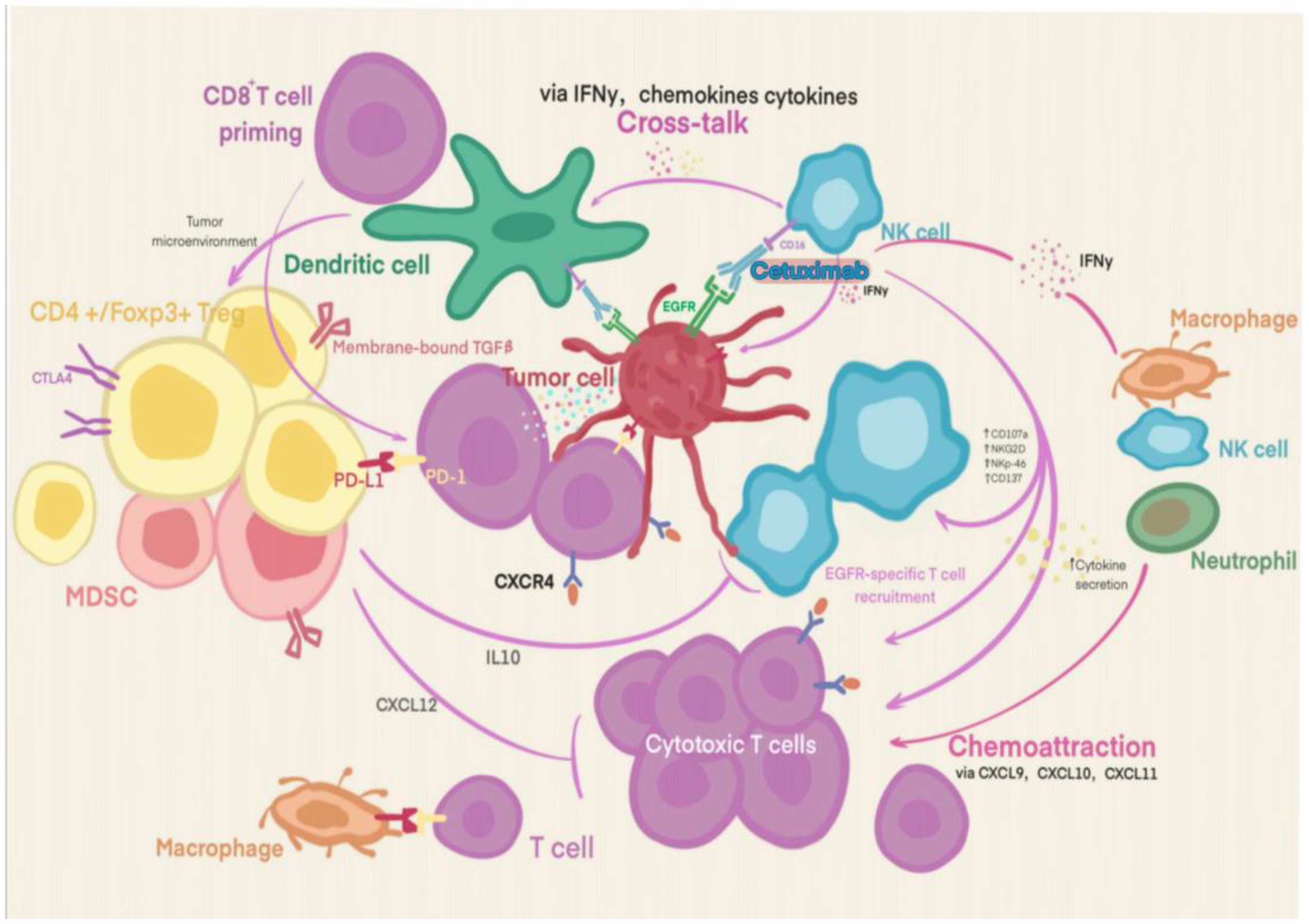
Mechanisms of Synergy Between Cetuximab and ICIs in MSS/pMMR Colorectal Cancer. Cetuximab Binds to the Epidermal Growth Factor Receptor (EGFR) on Tumor Cells, Blocking the Interaction Between EGFR and its Ligands Such as Epidermal Growth Factor. This Inhibition of Signal Transduction Within Tumor Cells Restricts Their Growth and Spread. Meanwhile, Cetuximab can Bind to Natural Killer (NK) Cells and Mediate Antibody - Dependent Cellular Cytotoxicity (ADCC). Through Various Chemokines Like CXCL9, CXCL10, CXCL11, and Cytokines Like IFN - γ and IL - 10, Cetuximab Promotes the Recruitment of CD8+ T Cells in the Tumor Microenvironment, Enabling Them to More Effectively Recognize and Attack Tumor Cells. Under the Action of Dendritic Cell Antigen Presentation (Mediated by Membrane - Bound TGF - β Interacting with Treg), T Cells are Activated, and their Immune - Modulating Effect on Cancer Cells is Enhanced. Cetuximab Can Enhance the Anti-Tumor Immune Response Through These Interactions.
Clinical Application of the Combination of Cetuximab and ICIs
Researchers believe that the synergistic and complementary activity of cetuximab and ICIs is the basis for the effect of the combination. Multiple clinical trials combining cetuximab and ICIs have confirmed the benefit of this therapy to several cancers. 46 Table 1 outlines various clinical trials that explore the synergistic impact of cetuximab combined with immunotherapy on patients with MSS/pMMR CRC.47–55 The CAVE trial, a non-randomized, multicenter phase II study, assessed the efficacy of the combination of cetuximab and avelumab in patients with RAS wild-type mCRC who had previously not responded to at least two standard treatment regimens. Among the 71 CRC patients with MSS status, the mOS was 11.6 months, the mPFS was 3.6 months, and the ORR was 8.5%. 47 The AVETUX trial, a non-randomized, multicenter, phase II study, aimed to evaluate the efficacy and safety of the combination therapy consisting of avelumab, cetuximab, and mFOLFOX chemotherapy in previously untreated patients with RAS/BRAF wild-type mCRC. The findings indicated that the one-year PFS rate reached 40%, with a median PFS of 11.1 months. 49 The AVETUXIRI study tested a similar approach for patients with MSS mCRC who didn't respond to standard treatments, avelumab combined with cetuximab and irinotecan were used. This study divided patients into two groups based on RAS status and BRAF V600E status. Group A had RAS WT, and Group B had RAS MUT. The DCR was 60% for Group A and 61.5% for Group B. PFS was 4.2 months for Group A and 3.8 months for Group B. OS was 12.7 months for Group A and 14.0 months for Group B. 50 In the most recent study, Xu et al reported a concept-validation, single-arm, phase 2 trial that evaluated a combined therapy consisting of cetuximab, tislelizumab, and irinotecan in 33 patients with MSS and RAS WT mCRC who had undergone at least two prior lines of treatment. The primary outcome was achieved, showing a verified ORR of 33%. Secondary outcomes included a DCR of 79%, and mPFS and OS of 7.3 months and 17.4 months, respectively. 52
Clinical application on the combination of cetuximab and ICIs in MSS/pMMR metastatic colorectal cancer.

ICI, immune checkpoint inhibitors; MSS/pMMR, microsatellite stable/proficient mismatch repair; mCRC, metastatic colorectal cancer; PFS, progression-free survival; mPFS, median PFS; OS, overall survival; mOS, median OS; ORR, overall remission rate; DCR, disease control rate; FOLFOX6, folinic acid + fluorouracil + oxaliplatin; FOLFOXIRI, folinic acid + fluorouracil + oxaliplatin + irinotecan; NR, not reported.
Although most of these studies achieved significant efficacy, some did not meet the primary study endpoint. For instance, in a phase Ib/II trial, cetuximab was combined with pembrolizumab to treat patients with RAS wild-type mCRC who had received at least one prior therapy for advanced disease. A total of forty-four patients were assessed for treatment effectiveness. The trial did not meet its primary efficacy goal [ORR: 2.6%, 6-month PFS: 31%; P = .52]. The mPFS was 4.1 months [95% confidence interval (CI): 3.9 to 5.5 months]. 48 Meanwhile, some studies have terminated recruitment, although the reasons for stopping recruitment have not been disclosed.53–55 Furthermore, the advantage of adding ICIs to cetuximab has not been confirmed in large-sample real-world studies. Thus,Optimizing current treatment regimens or developing new therapeutic combinations based on the combination cetuximab and ICIs is necessary. In the latest research, the BEACON study and the BREAKWATER study have demonstrated the outstanding efficacy of Encorafenib + cetuximab in treating BRAF V600E-mutant metastatic colorectal cancer.56,57 At the same time, the SEAMARK study explored the efficacy of cetuximab and encorafenib plus pembrolizumab for MSI-H/dMMR BRAF V600E-mutant mCRC. 58 Based on these research findings, it is reasonable to anticipate the initiation and exploration of the efficacy of cetuximab and encorafenib plus pembrolizumab for MSS/pMMR BRAF V600E-mutant CRC. Moreover, the combination of immunotherapy and local therapy in the treatment of MSS/pMMR mCRC enhances the anti-tumor immune response, 59 it is worth considering the initiation of clinical study to evaluate the combination of cetuximab with ICIs followed by brachytherapy or interstitial radiotherapy for the treatment of MSS/pMMR CRC. Collectively, the outcomes, which include both achievements and setbacks, from the aforementioned clinical studies will significantly contribute to refining this therapeutic pairing. Moving forward, the validation of this combined strategy will require a greater number of globally conducted, randomized, phase III trials. These trials should compare this combination therapy with conventional treatments to ascertain the efficacy of immunotherapy in conjunction with cetuximab as a potential treatment for patients with MSS/ pMMR CRC.
Challenge and Perspectives
In summary, the existing mCRC multimodal therapies have greatly improved in recent years. The antitumor mechanisms of cetuximab and ICIs are different. Furthermore, the effects of ICIs and cetuximab are complementary, which theoretically improve treatment efficacy. Additionally, some relevant clinical results have supported this hypothesis. However, these studies have some limitations. The single-arm nature and small sample size are the main limitations. Next, chemotherapeutic drugs or other targeted drugs were included in some of these studies. These factors may lead to biased results. Therefore, large-scale, multicenter prospective clinical studies are necessary to confirm the aforementioned findings. Nevertheless, the clinical application of this combination has the following problems: (1) The exact mechanism underlying the activation of ICIs and cetuximab for treating MSS/pMMR CRC remains unclear and needs further elucidation. (2) The optimal duration of this treatment for patients who respond to the combination of ICIs and cetuximab is a crucial factor. (3) Disease management after the development of resistance to this combination strategy is also a point of concern because once acquired resistance develops further, the levels of immunosuppressive cells and associated immune checkpoints increase and exhibit their functions in the TME, which are the key mechanisms for tumor progression and even hyperprogression. Therefore, acquired drug resistance is our next research topic. (4) Even though most small studies showed that side effects from using this combination of treatments were manageable, there are still concerns about side effects. Thus, safety data and counter strategies should be obtained before large-scale clinical application.
Since combining cetuximab and immunotherapies for treating MSS/pMMR CRC are mainly limited to Phase I-II clinical studies with small sample sizes, there is still insufficient evidence for clinical practice. However, it still presents great potential for clinical application. An increasing number of cetuximab combinations with various immunotherapies are emerging. Currently, significant advancement has been made in chimeric antigen receptor (CAR)-T cell therapies for CRC, 29 offering a potentially powerful means to target EGFR and eliminate cancer cells selectively. Meanwhile,recent researches have focused on targeting CCR8+ Tregs applying anti-CCR8 antibodies in CRC mouse models.60,61 These results suggest that anti-CCR8 antibodies hold significant promise for CRC either as monotherapy or in combination with other targeted drugs,such as cetuximab. Additionally,targeting CXCR2 is a promising strategy for modulating the TME, several early-phase clinical trials assessing the safety and efficacy of CXCR2 inhibitors are under way. 62 Combining cetuximab with CXCR2 inhibition may enhance overall therapeutic effect and potentially improve MSS/pMMR colorectal cancer patient outcomes.
Conclusion
In conclusion, the combination of cetuximab and ICIs is a promising therapeutic strategy against MSS/pMMR CRC. This strategy is expected to be clinically beneficial, and the likelihood of applying it as a potential therapeutic approach in clinical practice for treating MSS/pMMR CRC is expected to increase.As we stand on the precipice of a new era in cancer treatment, this combined treatment strategy will offer new hope for colorectal cancer patients with MSS/pMMR.
Footnotes
Acknowledgements
The authors acknowledge that this work was supported by the partly supported by the Natural Science Foundation of Enshi Tujia and Miao Autonomous Prefecture Government (D20220060), the Beijing Bethune Public Welfare Foundation(2023-YJ-041-J-005) and the 2020 annual funding for discipline construction, Zhongnan Hospital of Wuhan University (YYXKNLJS2024010).
Author Contributions/CRediT
BP: Searched and analyzed the published literature, drafted the manuscript. SP:assisted in the revision of the figures,searched and analyzed the published literature,polished the manuscript.WC: Concept or design. LL: reviewed and edited the manuscript. FZ: reviewed and edited the manuscript. All authors contributed to the article and approved the submitted version.
Funding
This work was supported by the partly supported by the Natural Science Foundation of Enshi Tujia and Miao Autonomous Prefecture Government (D20220060), the Beijing Bethune Public Welfare Foundation(2023-YJ-041-J-005) and the 2020 annual funding for discipline construction, Zhongnan Hospital of Wuhan University (YYXKNLJS2024010). 2020 annual funding for discipline construction, Zhongnan Hospital of Wuhan University, Beijing Bethune Public Welfare Foundation, Natural Science Foundation of Enshi Tujia and Miao Autonomous Prefecture Government (grant number YYXKNLJS2024010, 2023-YJ-041-J-005, D20220060).
Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.