
Abstract
Objective
To investigate the optimal radiotherapy regimen for synchronous bilateral breast cancer (SBBC) by utilizing dosimetric and radiobiological indicators, and to assess the impact of applying an optical surface monitoring system(OSMS) on the precision of SBBC radiotherapy treatment.
Methods
Nine patients with SBBC who underwent breast-conserving radiotherapy were retrospectively selected. Four treatment plans were designed for each patient using the Versa HD (Elekta, Stockholm) accelerator: single-isocenter intensity-modulated radiotherapy/volumetric modulated arc therapy(IMRT-ISO1/VMAT-ISO1) and dual-isocenter IMRT/VMAT(IMRT-ISO2/VMAT-ISO2), with a prescription dose of 42.4 Gy in 16 fractions. Dosimetric parameters and radiobiological impact were measured for the target and organs at risk(OARs). The monitoring log files of three SBBC patients were analyzed to quantitatively assess real-time delta shifts encompassing six degrees of freedom (DOFs) during intrafraction and interfraction treatment processes.
Results
Compared to both the IMRT techniques, the VMAT techniques offered superior target conformity, uniformity, and dose fall-off capability. Among the four treatment plans, VMAT-ISO1 exhibited optimal performance by significantly reducing radiation exposure volume to OARs while maintaining exceptional precision in dose delivery and execution efficiency. The tumor control probability (TCP) was exceeded by 98.5% for all four modalities. According to the OSMS logs, the maximum absolute error in translational motion during the treatment of three SBBC patients was predominantly manifested along the vertical(VRT) axis, with an mean value of 2.2 mm. Additionally, it was observed that the coronal plane (YAW) exhibited the largest error in terms of rotational angle, with an mean deviation of 1.1°.
Conclusions
The VMAT-ISO1 technique demonstrates apparent dosimetric and radiobiological advantages in SBBC radiotherapy, ensuring precise dose delivery and shortening treatment durations. The accuracy of SBBC radiotherapy is ensured by OSMS through pre-treatment positioning correction and real-time monitoring throughout the treatment process.
Keywords
Introduction
Breast cancer is the most prevalent malignancy among women, with approximately 2.3 million new cases reported annually. 1 Synchronous bilateral breast cancer (SBBC) is a rare subtype characterized by simultaneous tumor occurrence in both breasts. 2 Although it represents only 2% to 11% of all breast cancers, 3 the detection rate of SBBC is increasing with advancements in imaging technology. 4 Compared to unilateral breast cancer, SBBC has a comparatively lower survival rate. 5 As a crucial treatment modality for breast cancer, radiotherapy has demonstrated its effectiveness in enhancing tumor control and patient survival rates in recent years. 6 Therefore, precise investigations on radiation dosimetry for SBBC are imperative to improve treatment efficacy and minimize potential complications.
The target volume geometry of SBBC often resembles a large C shape, making the design of radiotherapy plans time-consuming and complex. With the advent of modern radiotherapy technology, intensity-modulated radiotherapy (IMRT) and volumetric modulated arc therapy (VMAT) have emerged as effective techniques for controlling beam shape and intensity to accommodate complex anatomical structures and tumor locations. These techniques are widely used in the design of intricate clinical plans.7–10 For instance, Alhefny et al reported that IMRT showed the superior target conformity compared with 3-dimensional conformal radiotherapy(3D-CRT) and VMAT in SBBC radiotherapy. 11 Cheng et al published that VMAT reduced beam delivery time while maintaining an acceptable dose for organ at risk (OARs). 12
Given the influence of respiratory motion on the mammary gland and the prolonged treatment times for SBBC patients, real-time monitoring of the patient's target volume movement during treatment is a critical consideration for ensuring treatment accuracy in clinical practice. To our knowledge, few studies have reported real-time motion during treatment in SBBC patients. AlignRT (VisionRT, London) is a commercially available optical surface monitoring system (OSMS) that provides real-time visual feedback on patient motion by continuously monitoring the patient's surface region of interest(ROI) during treatment process. Although it has been widely used in the setup 13 and deep inspiration breath hold (DIBH) treatment 14 of unilateral breast cancer, its application remains limited in SBBC.
Our study introduced a novel approach by conducting an integrated evaluation of single- and dual-isocenter IMRT and VMAT plans for SBBC, complemented by empirical measurements of dose delivery precision. We harnessed the capabilities of an OSMS in conjunction with advanced radiotherapy techniques, offering a comprehensive assessment of treatment plans and real-time patient motion monitoring during treatment process. The primary aim of this study was to propose an optimal clinical management strategy for SBBC patients, achieved through a detailed analysis of dosimetric and radiobiological outcomes, and the practical application of OSMS.
Materials and Methods
Patient Selection and Volume Delineation
From February 2021 to February 2022, CT image datasets of nine patients who underwent bilateral breast-conserving radiotherapy at the Radiotherapy Department of Peking Union Medical College Hospital were retrospectively selected. We have de-identified all patient details. The median age of the patients was 51 years (range: 43-69 years). In the supine position, the patients were stabilized in a breast board in free-breathing mode, with their arms raised above their head. Patient characteristics are shown in Table 1.
Patient and Tumor Characteristics (9 Patients, 18 Lesions).
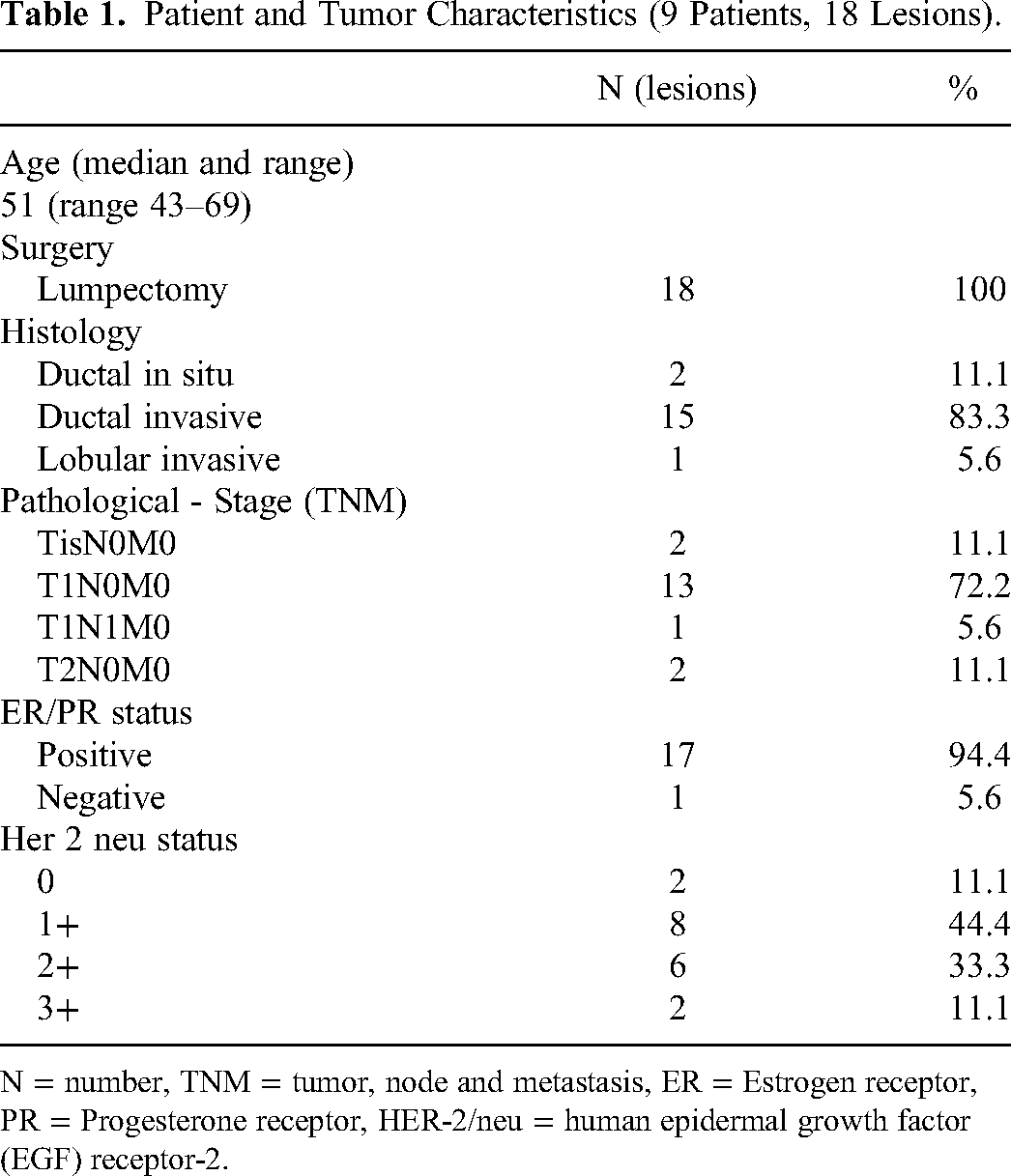
N = number, TNM = tumor, node and metastasis, ER = Estrogen receptor, PR = Progesterone receptor, HER-2/neu = human epidermal growth factor (EGF) receptor-2.
The clinical target volume (CTV) included bilateral mammary glands and the tumor bed. The planning target volume (PTV) was generated by expanding the CTV with a 5 mm margin in the left and right directions, a 10 mm margin in the superior and inferior directions, a 5 mm margin in the posterior direction, and no expansion in the anterior direction. The PTV was shrunk to 5 mm below the skin on the skin side. The reporting of this study conforms to STROBE guidelines. 15
Planning Techniques
Previous studies have indicated that hypofractionation can be considered as a viable therapeutic approach for SBBC. 16 The prescribed dose for patients was 42.4 Gy in 16 fractions, with the objective of encompassing at least 95% of the target volume while ensuring target conformity and uniformity, as well as minimizing the dose received by OARs. All treatment plans were designed using the Versa HD accelerator, with a spatial resolution of 5 mm and 6 MV photon energy, and variable dose rate up to 600 MU/min.
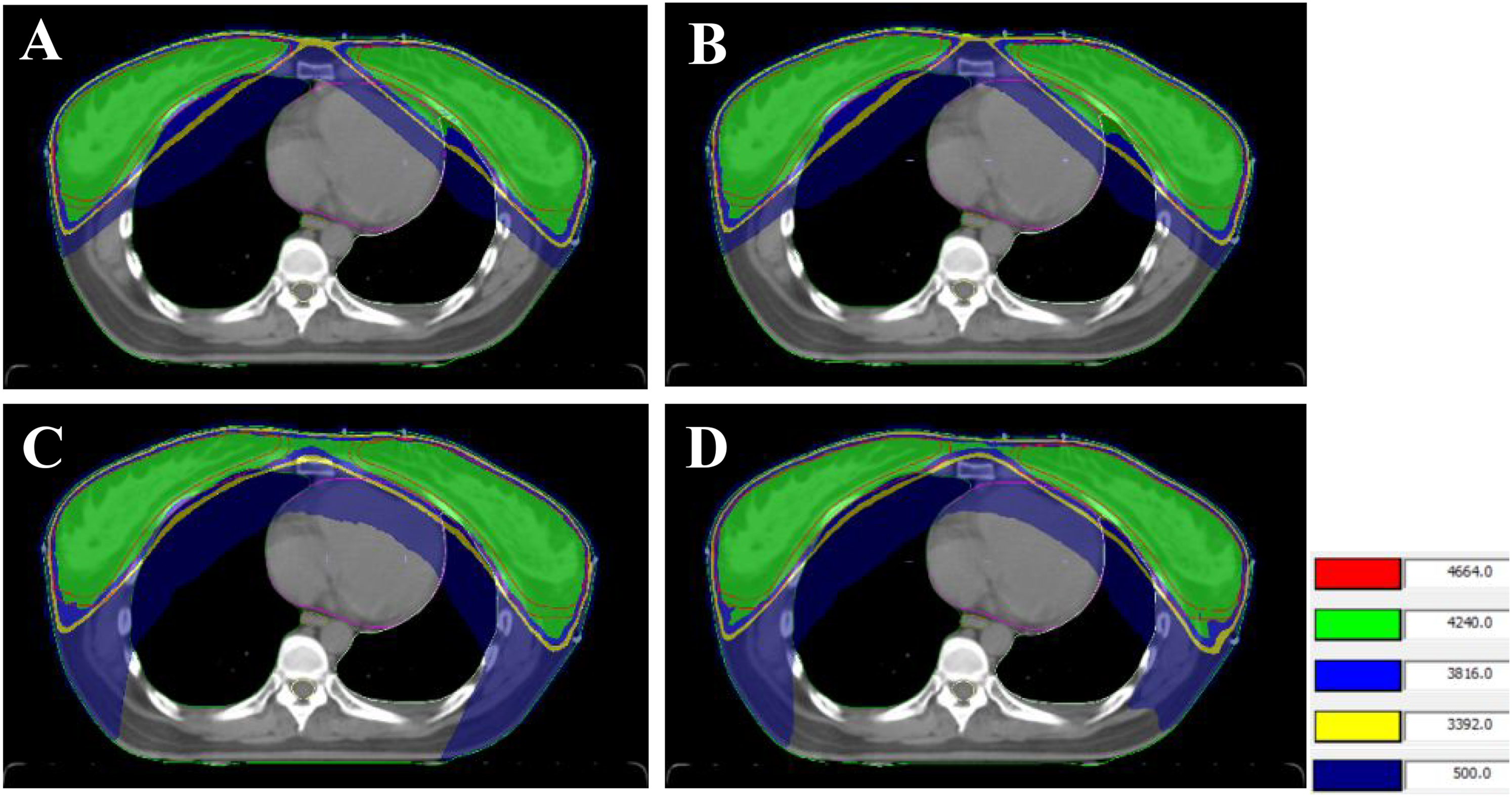
Four planning techniques (Figure 1) were implemented for each patient: single-isocenter IMRT (IMRT-ISO1), dual-isocenter IMRT (IMRT-ISO2), single-isocenter VMAT (VMAT-ISO1), and dual-isocenter VMAT (VMAT-ISO2).The isocenter of the single-isocenter plan was placed under the middle of the sternum, and the two isocenters of the dual-isocenter plan were shifted 5 cm to the left and right relative to the isocenter of the single-isocenter plan, and were consistent in anterior–posterior and superior–inferior directions. The IMRT-ISO1 plan utilized a total of eight fields, distributed within an approximate range of 240°-120°.Each breast was treated with four fields using fixed tungsten jaws. A suitable pair of tangent angles were selected based on the patient's target anatomy, and an additional above 5° was applied to the remaining two fields based on the tangent fields.IMRT-ISO2 plan used two isocenters, with the same field angle as IMRT-ISO1 plan. For the VMAT-ISO1 plan, a single beam consisting of two arcs was utilized with the gantry starting angle of 200° and rotating by 315°. For the VMAT-ISO2 plan, two beams were applied: the left beam used the left isocenter and fixed tungsten jaws to cover only the left breast, with the gantry starting at an angle of 300° and rotating by 220°. while the right beam utilized the right isocenter and fixed tungsten jaws containing only the right breast, starting at an angle of 200° and rotating by 220°. Each beam underwent one clockwise rotation followed by one counterclockwise rotation. Both IMRT and VMAT were coplanar plans with the collimator and treatment couch angles set at 0°.

Beam arrangements and isocenter position in (A) IMRT-ISO1, (B) IMRT-ISO2, (C) VMAT-ISO1, (D) VMAT-ISO2. The gray cross is isocenter point.
Dosimetric and Radiobiological Evaluation
The evaluation of the plans was based on cumulative dose-volume histogram (DVH) analysis. The parameter VxGy represents the volume that receives a dose equal to or higher than X Gy, relative to the total volume of that organ. DX% represents the irradiated dose of X% of the volume of the organ. For PTV, the evaluation indexes were as follows: maximum dose Dmax, mean dose Dmean, D2%, D98%. The conformal index (CI) and the homogeneity index (HI) and the gradient index (GI) of the PTV were calculated according to the following formula:


For OARs comparison, the following dosimetric parameters were evaluated: V5Gy、V10Gy、V20Gy、V30Gy、V40Gy、D20%、Dmean of left lung and right lung; V5Gy、V10Gy、V20Gy、V30Gy、V40Gy、Dmean of heart and liver; D0.1cm3 of the spinal cord (exposure dose of 0.1 cm3 volume).
Radiobiological indicators are measurable parameters that predict cellular responses to radiation, essential for evaluating treatment plans’ effectiveness in tumor control and normal tissue protection.
19
We designed a Python program using equations 4 and 5 to calculate the tumor control probability (TCP) and the normal tissue complication probability (NTCP) based on equivalent uniform dose (EUD) to assess the radiobiological impact during SBBC irradiation.
20


Patient-Specific Quality Assurance
The planar dose distribution of all plans was validated using ArcCheck(Sun Nuclear Corporation, Melbourne, FL), which enables measurement and analysis of deviations in dose transmission by comparing with the planned dose. The global gamma pass rates were used to evaluate the difference between the planar dose distribution generated by TPS and the actually measured dose distribution. The selected criteria for analysis included 2%/2 mm, 3%/2 mm, and 3%/3 mm with a threshold set at 10%. 22
The execution efficiency was assessed by quantifying the number of Monitor Units (MU) and beam on time for each plan.
Optical Surface Monitoring System
The AlignRT system consists of a computer workstation and three ceiling-mounted camera pods, each containing one projector and two cameras. The stereo camera system reconstructs a real-time 3D surface image by detecting visible light speckles from a projector. Rigid registration is performed by precisely determining the position of the patient's ROI and aligning it with the reference body surface, the matching results are real-time displayed in the form of 6 degrees of freedom(DOFs) errors. 23 Moreover, OSMS in conjunction with the linac, enables real-time monitoring of the patient's surface during beam delivery and interrupts the beam when a preset threshold is exceeded, thus ensuring the accuracy of the dose delivery.
In this study, the ROI delineation range of SBBC included bilateral mammary glands and the middle sternal region, up to the subclavicle, down to the ribs, and laterally to the midaxillary line. The real-time surface of the patient was captured before treatment to qualitatively assess the positional accuracy and perform position correction. OSMS continuously monitored the patient's surface throughout the entire treatment session. Subsequently, real-time data from the OSMS monitoring logs were analysed for quantitative evaluation of target motion during both intrafraction and interfraction treatment processes of SBBC patients.
Statistical Analysis
The DVH was outputted in text format and imported into Origin 2018 software to generate average DVH for the PTV and OARs. Data statistics have been demonstrated as mean±standard deviation (SD). GraphPad Prism8 was used for plotting, and statistical significance of parameters was analyzed using the Wilcoxon matched-pairs signed rank test with a significance level of 0.05.
Results
Dose Comparisons for PTV
Figure 2 shows the dose distributions across the same cross-section of the four treatment regimens in one representative case, and the coverage of the prescription dose and low dose zones can be visually seen. Figure 3 depicts the mean DVH of PTV of four different plans in nine SBBC patients. The DVH curves for the same radiation technique(IMRT or VMAT) exhibited a high degree of overlap, while the volume encompassing the high-dose region in VMAT was found to be lower compared to IMRT. Table 2 presents the dosimetric results of the PTV. The IMRT-ISO1 exhibited the highest Dmax (46.73±0.54 Gy) and Dmean(44.38±0.26 Gy) and D2% (45.59±0.35 Gy) compared to the other three methods. The Dmean and D2% of VMAT-ISO1 and VMAT-ISO2 were lower than those of IMRT-ISO1 and IMRT-ISO2. Among the four planning methods, VMAT-ISO2 exhibited the lowest Dmax (46.43±0.32 Gy), Dmean (43.77±0.22 Gy), and D2% (44.91±0.3 Gy), as well as the largest D98% (41.15±0.23 Gy).
Dose distributions across the same cross-section of four treatment regimens in one representative case. A:IMRT-ISO1; B:IMRT-ISO2; C:VMAT-ISO1; D:VMAT-ISO2.

Mean DVH of PTV for four different plans in nine SBBC patients.
Dosimetric Parameters of PTV in Four Treatment Regimens.

a: IMRT-ISO1 versus IMRT-ISO2; b: VMAT-ISO1 versus VMAT-ISO2; c: IMRT-ISO1 versus VMAT-ISO1; d: IMRT-ISO2 versus VMAT-ISO2.
Dose Comparisons for OARs
Figure 4 presents the mean DVH curves of the left lung, right lung, heart, and liver in four treatment regimens of nine SBBC patients. It was noteworthy that a distinct intersection point can be observed between the VMAT-ISO1 and VMAT-ISO2 curves and the IMRT-ISO1 and IMRT-ISO2 curves for both the left lung and right lung. In the high-dose zone beyond this intersection point, VMAT showed significantly better OARs sparing compared to IMRT, while IMRT performed excellently in the low-dose zone prior to the intersection point. The four DVHs of the heart and liver differed slightly, IMRT performed better in reducing coverage of the low-dose region, while the DVHs of VMAT-ISO1 and VMAT-ISO2 displayed nearly identical profiles.
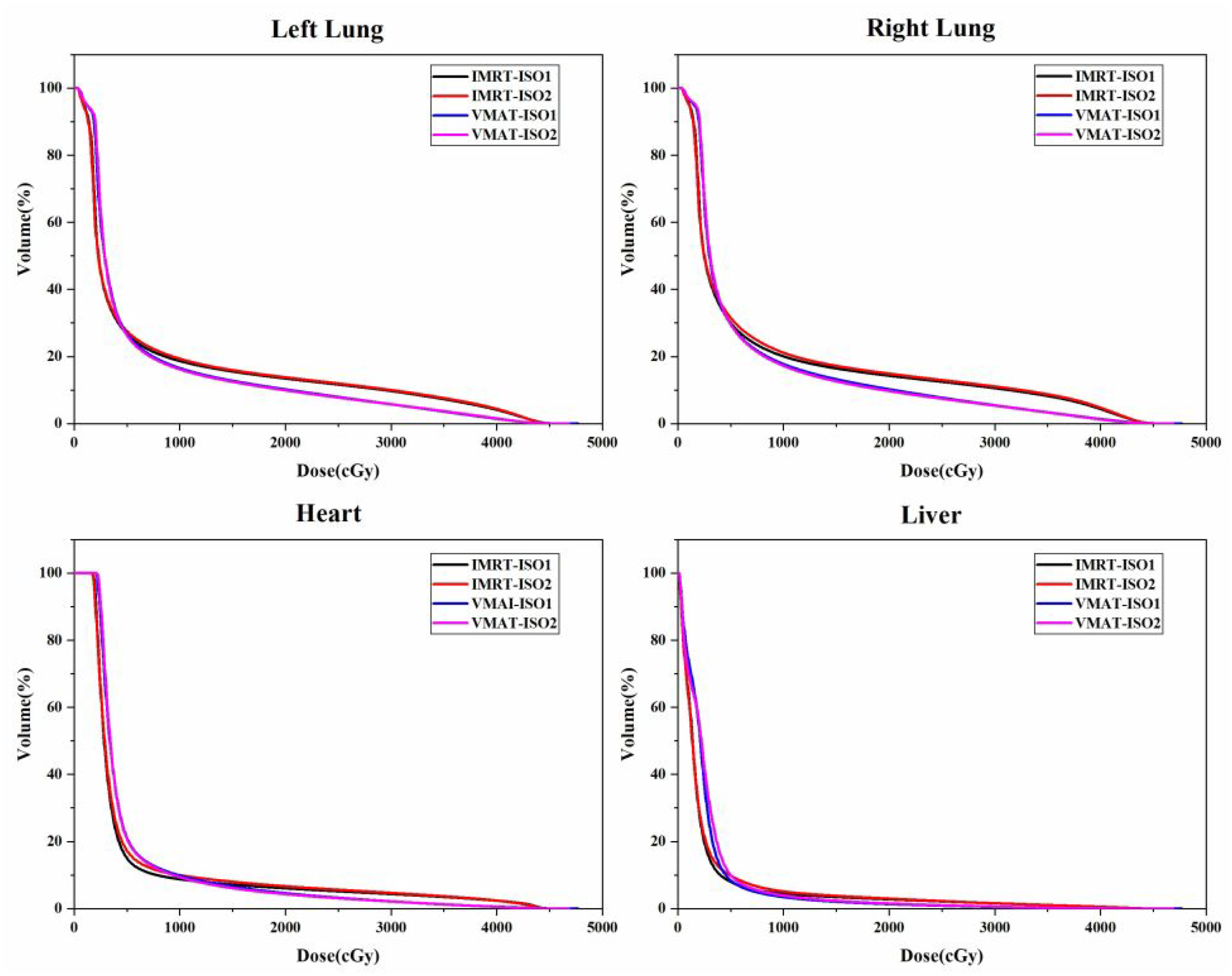
Mean DVH of OARs for four different plans in nine SBBC patients.
Table 3 shows the dosimetric parameters of OARs. The overall indicators of IMRT-ISO1 were better than those of IMRT-ISO2. For the left and right lungs, VMAT-ISO1 results were slightly higher than VMAT-ISO2. The lung parameters of VMAT-ISO1 and VMAT-ISO2 exhibited significantly lower values compared to those of IMRT-ISO1 and IMRT-ISO2, with the advantage becoming increasingly pronounced as the dose escalated. The mean dose of VMAT-ISO2 was lowest in the left lung (6.69±0.57 Gy) and the right lung (6.87±0.77 Gy). In terms of the heart, the V5Gy (15.08±7.66%), V10 (8.72±5.33%), and Dmean (5.33±1.76 Gy) values achieved with IMRT-ISO1 were lower compared to those obtained with IMRT-ISO2, VMAT-ISO1, and VMAT-ISO2. The V5Gy of the liver were higher for VMAT-ISO1 and VMAT-ISO2. The standard deviations of VMAT were smaller than those of IMRT, suggesting that VMAT exhibited greater robustness in terms of the geometric variabilities of various patients’ OARs.
Dosimetric Parameters of OARs in Four Treatment Regimens.

a: IMRT-ISO1 versus IMRT-ISO2; b: VMAT-ISO1 versus VMAT-ISO2; c: IMRT-ISO1 versus VMAT-ISO1; d: IMRT-ISO2 versus VMAT-ISO2.
Radiobiological Parameters
Through the calculation of DVH, EUD and TCP of PTV and EUD and NTCP of OARs are shown in Table 4. Based on formulas (4) and (5), it can be seen that TCP and NTCP are the increase functions based on EUD. The higher the value of EUD, the larger the TCP and NTCP. The TCP of all four treatment modalities exceeded 98.5%. An very excellent tumor control effect can be achieved using any of these methods. The NTCP was below 0.05% for all cases, resulting in a substantial reduction in the incidence rate of potential complications. The EUD value of VMAT in both lungs was significantly lower than that of IMRT, and NTCP approached 0.
Results of Radiobiological Indicators for the Four Treatment Regimens.

a: IMRT-ISO1 versus IMRT-ISO2; b: VMAT-ISO1 versus VMAT-ISO2; c: IMRT-ISO1 versus VMAT-ISO1; d: IMRT-ISO2 versus VMAT-ISO2.
Delivery Parameters
The results of dose delivery accuracy verification for four treatment modalities in 9 SBBC patients using Arccheck are presented in Table 5, along with the MU and estimated beam delivery time calculated for each plan in TPS. The gamma pass rates exceeded 96% for all four plans, with IMRT-ISO1 demonstrating the highest level of dose delivery accuracy while VMAT-ISO2 exhibited the lowest. Among them, VMAT-ISO1 had the lowest MU and beam on time. Compared to the other three planning methods, a reduction of 16%, 15%, and 22% was observed in MU, respectively, accompanied by a decrease in time by 106%, 113%, and 42%.
Results of Delivery Accuracy and Efficiency Indicators for the Four Treatment Regimens.

a: IMRT-ISO1 versus IMRT-ISO2; b: VMAT-ISO1 versus VMAT-ISO2; c: IMRT-ISO1 versus VMAT-ISO1; d: IMRT-ISO2 versus VMAT-ISO2.
Real-Time Monitoring Results of OSMS
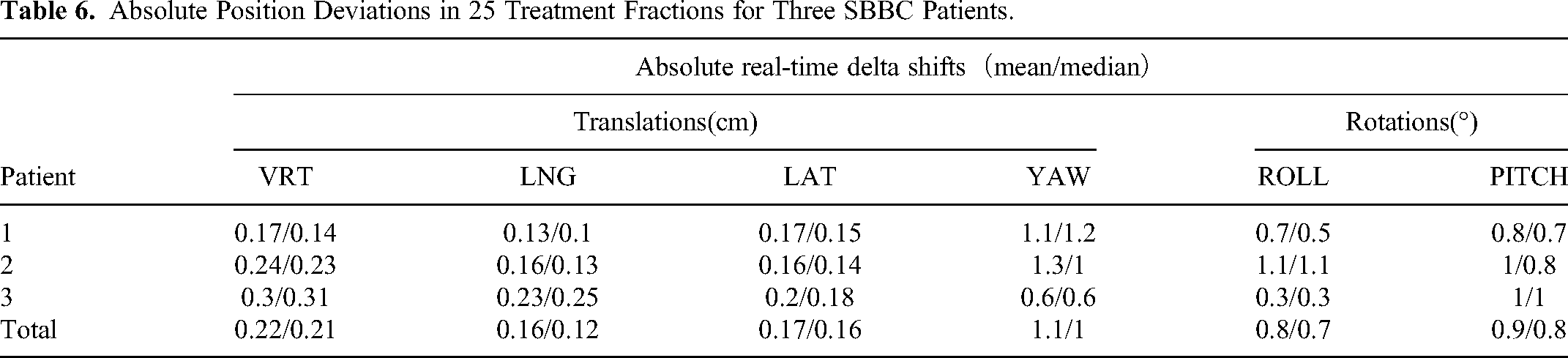
Figure 5A displays the monitoring interface of OSMS during the treatment process of a SBBC patient using VMAT-ISO1 technique. The green surface represented the real-time body surface captured prior to patient treatment via the Capture function, while the magenta surface represented the imported reference body surface for alignment. The precise alignment of the abdomen, thorax, bilateral axilla and arms can be achieved by employing real-time surface imaging to accurately correct the patient's position. The real-time delta shifts of 6 DOFs were represented by the values on the left-hand side, with a translation error threshold set at 3 mm and a rotation error threshold set at 3°. Figure 5B illustrates the coordinate system for 6 DOFs data analysis, with the arrow pointing in a positive direction. The 6 DOFs shifts recorded by OSMS real-time monitoring during the patient's initial treatment fraction are displayed in the form of a scatter plot in Figure 5C. The duration was approximately 300 s, with translation errors within 2 mm and rotational errors within 1°.The changes in median values of translational and rotational shifts recorded by OSMS during 13 treatment fractions for the patient are depicted in Figure 5D. It was evident that the translational displacement remained within a limit of 3 mm, and the rotational angle did not exceed 2°. The mean and median values of absolute displacement in 25 treatment fractions for three SBBC patients are presented in Table 6. It can be observed that the maximum deviation in patient positioning occurs in the VRT and YAW directions during the treatment process, with mean values of 2.2 mm/1.1° and a median of 2.1 mm/1°. The histograms of real-time monitored intrafractional displacements for the three patients during 25 treatment fractions are presented in Figure 5E.

OSMS real-time monitoring results. A: The monitoring interface of OSMS during treatment for SBBC patients. The green surface represented real-time surface during treatment, while the magenta surface represented the reference surface. B: 6 DOFs coordinate system. The arrow direction was positive. C: Real-time monitoring errors during the first treatment fraction of a SBBC patient using VMAT-ISO1 technique. D: Median translation and rotation shifts during 13 treatment fractions for the SBBC patient. E: Histograms of 6 DOFs displacements for three SBBC patients within 25 treatment fractions.
Absolute Position Deviations in 25 Treatment Fractions for Three SBBC Patients.
Discussion
SBBC is a rare condition. The wide coverage and significant shape variations of the target area in SBBC patients pose challenges for achieving uniform dose distribution and minimizing high radiation doses to OARs. Currently, there are still no standardized guidelines for radiation therapy in SBBC. 7
In our study, four treatment regimens of SBBC, IMRT and VMAT in single-isocenter and dual-isocenter were designed. All four treatment options were clinically acceptable in terms of PTV coverage. The CI values of VMAT-ISO1 and VMAT-ISO2 were closer to 1, higher than those of IMRT-ISO1 and IMRT-ISO2, with slightly lower HI and GI values than IMRT-ISO1 and IMRT-ISO2. This reflected the advantages of VMAT in improving target conformity and increasing dose uniformity. The results were consistent with those reported by Nicolini et al, who found that VMAT produced higher quality and more reliable plans compared to IMRT. 24 Similarly, Fiorentino et al also reported that the application of VMAT for SBBC was safe and feasible. 8 Cheng et al compared the dosimetric characteristics of helical tomotherapy (HT), VMAT and IMRT in treating SBBC. They revealed VMAT had a shorter treatment time and achieved clinically acceptable dose distribution, 12 which is also consistent with our results.
Furthermore, there are also studies dedicated to evaluating the dose differences introduced by single-center and dual-center approaches. Amoush A reported that the plan quality of single-isocenter technique using four-field mixed IMRT was comparable to that of dual-isocenter technique. 25 In our study, based solely on the dosimetric values, both single-center and dual-center plans are clinically acceptable. Although there were significant differences in certain OARs (such as lung V20), this may not necessarily imply clinical differences due to the small sample size. In practical clinical decision-making, considering the uncertainties in positional accuracy introduced by the moving treatment couch with dual-isocenter and the prolongation of treatment time, we recommend using a single-center plan, which is consistent with Banaei et al's study. 26
One issue that needs to be addressed in SBBC treatment is the correction of rotational errors. In this study, the OSMS was innovatively used to enable real-time monitoring of the complete treatment process for SBBC patients, thereby visualizing positional deviations resulting from intrafraction and interfraction motion. By improving positioning accuracy and providing real-time monitoring, OSMS has the potential to significantly enhance treatment precision, thereby demonstrating the feasibility and inherent advantages of its application in SBBC.
There are some limitations to the study. Firstly, the research was undertaken with the patients at our disposal. The present study is constrained by its small sample size, a reflection of the inherent rarity of SBBC. While the statistical analysis of our small sample size may not be fully representative of clinical outcomes, it does suggest a trend that warrants further investigation. Further clinical observation based on large groups of patients is needed to confirm our findings. Another limitation of this study is that four treatment regimens for SBBC patients were conducted while the patients were in the free breathing state, and there were still dose deviations caused by respiratory motion. The advantages of DIBH in reducing lung and heart radiation dose in unilateral breast cancer have already been demonstrated.27,28 Tamilarasu S et al investigated how the use of DIBH technique affects early-stage SBBC and concluded that it effectively decreases radiation dose to OARs. 29 However, a separate study conducted by S. Gaal et al suggested that the improvement in heart dose with DIBH was not uniform, and approximately one-third of patients did not benefit from it. 30 Taking into account our patients’ compliance and lengthy treatment duration, we opted for utilizing free-breathing mode in this research. In the future, we will utilize the OSMS to manage respiratory motion during DIBH in SBBC patients and further reduce radiation toxicity while improving treatment accuracy.
Conclusion
Based on the dosimetric analysis, VMAT-ISO1 demonstrated advantages in improving dose distribution and minimizing radiation exposure to OARs for SBBC. The technique provided superior dose delivery accuracy and a shorter treatment duration compared to other treatment regimens in this study. Furthermore, the integration of an OSMS may enhance patient positioning and motion monitoring, contributing to the precision of radiotherapy delivery.
Our findings contribute to the body of evidence that may support the optimization of radiotherapy regimens for SBBC. While this study provides valuable insights, it also highlights the need for further research to explore the long-term clinical outcomes and broader application of these techniques. Given the limited sample size of patients with SBCC in this study, it is essential to include a larger cohort of patients in order to obtain statistically robust results.
Footnotes
Acknowledgements
Not applicable.
Authors’ Contributions
ZZ conducted data analysis and wrote the manuscript. TD, BW and HZ assisted with part of the data acquisition. BY. and ZW were responsible for experimental design and supervision. WL and TD performed optical monitoring data acquisition. JQ revised the manuscript. All authors contributed to the study and critically reviewed the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Statement
This study was approved by the Research Ethics Committee of Peking Union Medical College Hospital, Chinese Academy of Medical Sciences (approval number: I-23PJ2133) on December 15, 2023 in Beijing, China. Patient informed consent was not required for this retrospective study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Key Research and Development Program of China, National High Level Hospital Clinical Research Funding, (grant number No.2022YFC2404606, 2022-PUMCH-B-116).