
Abstract
Purpose
To assess the usefulness of the novel CARWL index in predicting radiation-induced tooth loss (RITL) rates in locally advanced nasopharyngeal cancer (LA-NPC) patients undergoing concurrent chemoradiotherapy (C-CRT).
Methods
The study retrospectively examined data from 323 LA-NPC patients. The patients were divided into two groups based on cutoff values for CAR and weight loss (WL). The ideal cutoff for RITL was 3.0 g/dL [AUC: 83.0%, sensitivity: 83.6%, specificity: 81.4%, J-index: 0.650]. CARWL index was created by combining pretreatment CAR and WL status (WL ≤ 5.0% vs > 5.0%, resulting in four groups: Group 1: CAR < 3.0 and WL ≤ 5.0%, Group 2: CAR < 3.0 and WL > 5.0%, Group 3: CAR ≥ 3.0 and WL ≤ 5.0%, and Group 4: CAR > 3.0 and WL > 5.0%.
Results
RITL was diagnosed in 67.2% of patients. Since the RITL rates of Groups 2 and 3 were statistically indistinguishable, we combined them and created the three-tiered CARWL score groups: CARWL-0: CAR < 3.0 and WL ≤ 5.0%; CARWL-1: CAR < 3.0 and WL > 5.0%, or CAR ≥ 3.0 and WL ≤ 5.0%; and CARWL-2: CAR > 3.0 and WL > 5.0%. Comparative analysis revealed that the RITL rates gradually and significantly increased from CARWL-0 to CARWL-2 score groups (49.4% vs 64.7% vs 83.0%; P <0.001) despite similar baseline disease and patient characteristics. Results of the multivariate analysis showed that higher CARWL score groups were independent and significant predictors of increased RITL rates (p < 0.001).
Conclusion
Present results suggest that the novel CARWL index is a reliable biomarker for predicting RITL incidence in LA-NPC patients.
Introduction
Platinum-based definitive concurrent chemoradiotherapy (CCRT) with intensity-modulated radiotherapy (IMRT) has replaced radiation alone or sequential chemoradiotherapy regimens in the treatment of medically fit locally advanced nasopharyngeal carcinoma (LA-NPC) patients. This treatment approach has significantly improved locoregional disease control and overall survival rates. 1 Notably, advancements in this field have also substantially reduced severe toxicities affecting the skin, muscles, oral mucosa, esophagus, bone, and salivary glands. However, despite these advancements, treatment-related side effects continue to affect many such patients. Radiation-induced dental problems, including tooth decay and tooth loss, are frequently observed in individuals with LA-NPC following radiotherapy (RT), imposing a significant impact on their overall well-being. 2 Statistics suggest that approximately 30% of patients undergoing RT for head and neck tumors experience radiation-induced cavities, either as a direct consequence of RT or indirectly due to xerostomia and periodontitis.3,4 If left untreated, tooth loss may lead to malnutrition, hasten cancer cachexia, and diminish the body's capacity to tolerate oncological therapy, all of which can have a negative impact on the disease's prognosis. 5
The main factors contributing to radiation-induced tooth loss (RITL) include receiving a high radiation dose to the jaw (≥60 Gy), poor oral hygiene, severe periodontitis, undergoing concurrent chemotherapy, smoking habits, and chronic local or systemic inflammation.6,7 In recent years, the impact of inflammatory biomarkers on RITL has received significant attention. For instance, a study of 193 LA-NPC patients by Yılmaz et al 8 found that patients with high hemoglobin to platelet ratio (HPR) had a higher incidence of post-CCRT tooth loss compared to those with lower HPR levels (81.7% vs 85% for HPR > 0.48). Furthermore, a study on a group of 246 patients with LA-NPC discovered a strong correlation (p = 0.001) between the need for tooth extraction following CCRT and elevated levels of the systemic immune inflammation index (SII) measured before treatment. 9 Similarly, Somay et al 5 studied the effectiveness of the novel GLUCAR index in predicting tooth extraction rates after definitive CCRT in 187 LA-NPC patients. The authors defined the GLUCAR index as ‘GLUCAR = Fasting Glucose × CRP/Albumin Ratio’ and divided the patients into two groups based on a cutoff value of 31.8. The study results revealed that the need for tooth extraction was higher in the group with a high GLUCAR value than in the group with a low GLUCAR value (84.4% vs 47.4% for GLUCAR ˂ 31.8; odds ratio (OR): 1.82; p < 0.001).
The CARWL score, a unique combination of C-reactive protein-to-albumin ratio (CAR) and significant weight loss (WL > 5%), has recently been introduced as a novel prognostic scoring system for stage IIIC non-small cell lung cancer (NSCLC) patients who underwent radical CCRT. 10 Notably, the components of the CARWL score have also demonstrated effectiveness in predicting RT-induced toxicities in head and neck cancer patients.5,11 For instance, Yoshihara and colleagues found a significant association between hypoalbuminemia, missing teeth over a 5- or 10-year period, and the risk of root caries and related tooth loss. 12 Moreover, a study examining the impact of a high CRP/albumin ratio on oral squamous cell cancer patients revealed that those with tooth loss exhibited a significantly higher CRP/albumin ratio compared to those without tooth loss. 13 Malnutrition, a significant cause of WL, results in the deprivation of essential nutrients crucial for bodily functions. Furthermore, it weakens teeth, rendering them susceptible to both tooth decay and periodontal disease, consequently leading to tooth loss regardless of the patient's irradiation status. Motivated by such compelling data and the absence of similar studies, this retrospective cohort analysis aimed to test the utility of novel CARWL scores in stratifying LA-NPC patients into RITL risk groups following definitive CCRT.
Patients and Methods
Ethical Statement
Before any patient data was collected, the ethical council of Baskent University Medical Faculty authorized the present retrospective study design (Project no: DKA 20/58). As was the standard institutional norm, all patients provided signed informed consent for the analysis of blood samples, clinical and treatment data, and publication of their outcomes before the dentistry evaluations and commencement of the CCRT, either directly or through lawfully approved caregivers.
Demographic Features of Patients
The reporting of this study conforms to STROBE guidelines. 14 The Dentistry Clinics at Baskent University's Adana Research and Treatment Center examined the medical records of patients with LA-NPC who underwent CCRT and received oral and dental examinations before and after the treatment—the study period spanned from February 2010 to January 2024 retrospectively. To be eligible for participation, patients were required to meet specific criteria: they had to be at least 18 years old, possess histopathologic confirmation of squamous cell carcinoma, exhibit locally advanced disease according to the eighth edition of the American Joint Cancer Committee (AJCC) cancer staging criteria, have no prior history of other cancers, not have received systemic chemotherapy or head and neck RT, and have accessible complete blood count and biochemistry test results before CCRT. Eligibility for participation in the study was predicated on the availability of dental and panoramic radiography examination records before and after CCRT. Exclusion criteria encompassed patients presenting with tumor or lymph node invasion in the mandible, previous diagnosis of osteoradionecrosis of the jaws or a history of jaw surgery, concurrent use of steroids or other immune modifiers, and receipt of blood transfusions within 30 days preceding the initiation of CCRT. The study excluded patients with active systemic inflammatory diseases, including rheumatological, nephritic, and respiratory disorders, viral hepatitis, immune suppressive conditions, collagen vascular diseases, chronic inflammatory diseases, and glucose storage diseases. These restrictions were put in place to reduce the potential for biased effects caused by preexisting inflammatory and immunological illnesses, as well as the use of medications.
Baseline Oral Examination
All patients underwent a comprehensive dental evaluation by a skilled oral and maxillofacial surgeon (ES) before CCRT per the guidelines of the American Dental Association (ADA) and the US Food and Drug Administration (FDA). 15 Radiographic examinations were conducted using panoramic scans as part of standard dental care for every head and neck cancer patient, following the provided instructions by the manufacturer (J Morita, Veraviewepocs 2D, Kyoto, Japan). Dental caries were assessed in all teeth using the World Health Organization criteria with illuminated and explorer mirrors. 16
The periodontal assessment encompassed the evaluation of plaque levels, gingival inflammation, probing depth, and periodontal attachment loss. Plaque levels were ascertained using a previously delineated method 17 and appraised on natural teeth’ buccal surfaces. Gingival inflammation was assessed through two methods: employing the Gingival Index 18 to rate inflammation from 0 (indicating normal gingiva) to 3 (indicating severe inflammation) for each tooth and determining a bleeding-on-probing score, entailing the insertion of a periodontal probe no more than 2 mm into the sulcus at the gingival margin, then moving it along the buccal surface to the distobuccal line angle of each tooth. After examining each tooth in a quadrant, bleeding presence (1) or absence (0) was noted. The bleeding-on-probing score was determined by adding up the total number of teeth that showed bleeding. Probing depth and loss of attachment were evaluated using a UNC-15 periodontal probe at six specific locations on each tooth: the mesiobuccal, buccal, distobuccal, mesiolingual, lingual, and distolingual sites. Two measurements were taken at each probing location. First, the distance between the free gingival margin and the cementoenamel junction was measured. Then, the distance between the free gingival margin and the pocket base was measured to determine the periodontal pocket depth. The loss of attachment was calculated by subtracting the initial measurement from the subsequent measurement when the free gingival margin was positioned above the cementoenamel junction. Conversely, the two measurements were summed when the free gingival margin was below the cementoenamel junction. The examinations were conducted by a periodontist (SB) with assistance from a data recorder. Participants were examined while seated in a dental chair and exposed to illumination from a dental examination light.
Teeth lacking periodontal support, manifesting extensive decay beyond rehabilitative measures, and demonstrating substantial apical lesions unsuitable for root canal therapy were surgically extracted. Superficial dental caries were remediated through the application of fillings. Patients received comprehensive oral hygiene instructions and underwent dental scaling to enhance oral health practices.
Assessment of C-Reactive Protein-to-Albumin Ratio and Weight Loss (CARWL)
The pretreatment CAR for each patient was calculated by dividing the CRP level by the albumin level measured on the first day of C-CRT. 10 In addition, the percentage difference between the weight measurements taken on the first day of C-CRT and the weight reported by the patient for their measurement six months prior to starting C-CRT was calculated. Significant WL was defined as greater than 5% over the past 6 months, based on the Delphi criteria outlined by Fearon and colleagues. 19
Chemoradiotherapy Protocol
As previously described, the RT technique used for all patients was simultaneous integrated boost intensity-modulated RT (SIB-IMRT). 20 Co-registered imaging modalities, including computed tomography (CT), 18-fluorodeoxyglucose-positron emission tomography/CT (18-FDG-PET-CT), and magnetic resonance imaging (MRI), were used to delineate target volumes. The RT doses were as follows 20 : high-risk planning target volumes (PTV) received 70 Gy, intermediate-risk PTV received 59.4 Gy, and low-risk PTV received 54 Gy. These doses were delivered in 33 daily fractions, with no weekend treatment. In addition to RT every 21 days, patients were also advised to undergo three cycles of concurrent chemotherapy using cisplatin and 5-fluorouracil. After C-CRT, all patients were recommended to undergo two additional cycles of the same chemotherapy protocol as adjuvant therapy. Supportive care, including antiemetics, dietary recommendations, and other necessary assistance, was provided as needed.
Follow-Up Dental Examination
The procedure described in the “Baseline oral examination” section was followed, and additional oral and dental exams were conducted according to the scheduled timeline or as necessitated by clinical indications. The patients’ clinical and radiological examination findings were documented at 1, 3, 6, 9, and 12 months, and then at every scheduled 6-month interval or as needed following the completion of definitive C-CRT. Treatment plans for each patient were established and presented based on the principles outlined in the previously mentioned “Baseline oral examination” section (Figure 1).
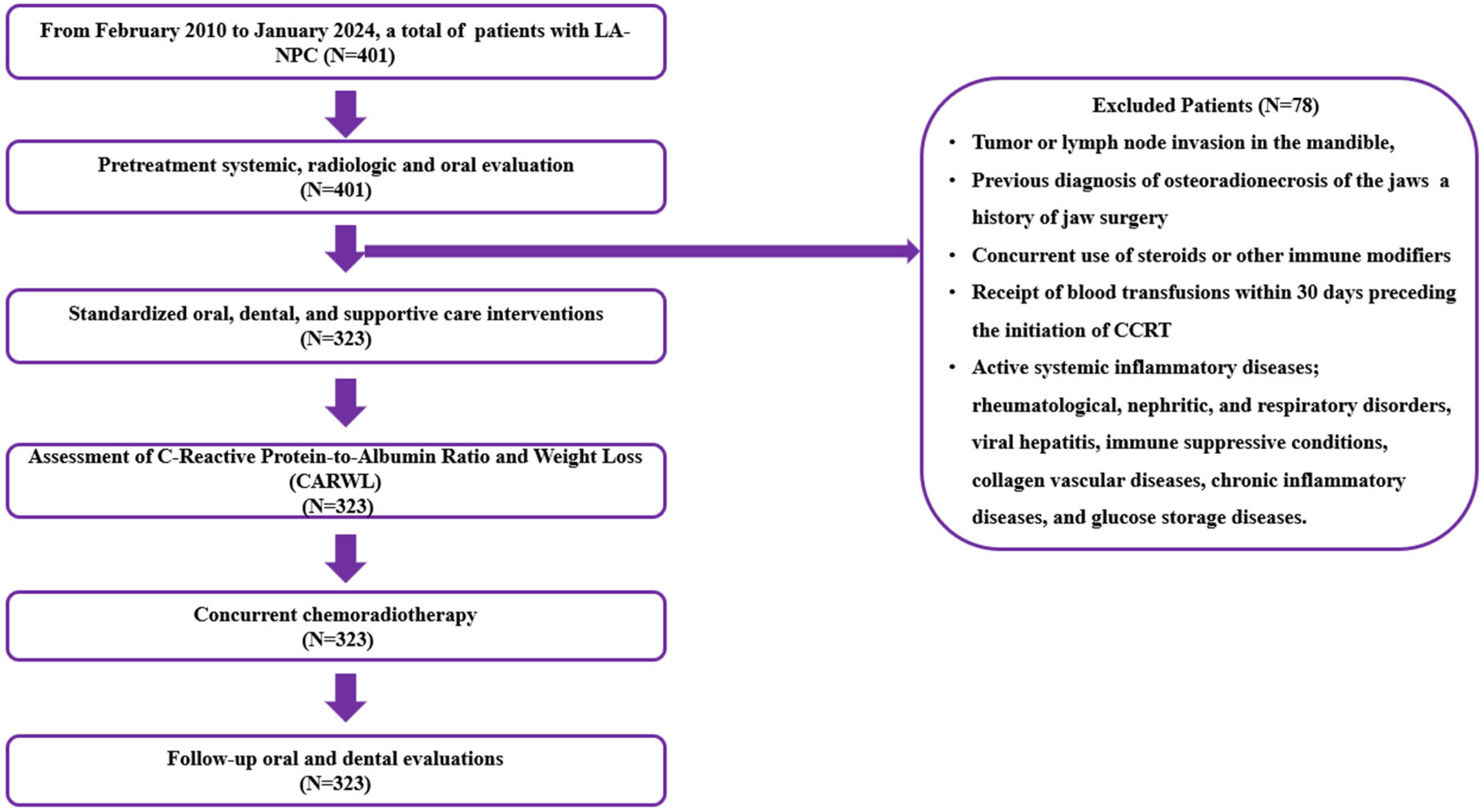
The flowchart depicts the process of selecting patients. Abbreviations: LA-NPC; locally advanced nasopharyngeal cancer, CCRT; concurrent chemoradiotherapy.
Statistical Analysis
The statistical analyses and calculations were performed using IBM SPSS Statistics 26.0 (IBM Corp., 2019) software. The study's primary endpoint was the connection between pretreatment CARWL index values and the requirement for tooth extractions during the post-C-CRT follow-up. Continuous variables were described using medians and ranges, while categorical variables were presented as percentage frequency distributions. Appropriate statistical analyses such as the Chi-square test, Student's t-test, or Spearman correlation were used to compare different patient groups. We utilized receiver operating characteristic (ROC) curve analysis to identify the pre-C-CRT cutoff(s) that could divide the entire research cohort into two groups with distinct outcomes. A logistic regression analysis was conducted to ascertain the variables with multivariate significance. All comparisons were two-tailed, and a p-value of ≤0.05 was considered significant.
Results
This retrospective analysis examined 323 patients diagnosed with LA-NPC who underwent CCRT and had oral health examinations. The baseline patient and disease characteristics for the entire cohort were as shown in Table 1. The age range of the study population spanned from 18 to 78 years, with a median age of 55. The preponderance of participants was male (67.2%), with the majority exhibiting T3–4 tumors (53.1%) and N2–3 nodal (78.9%) disease. A history of smoking or alcohol consumption was present in 64.4% and 59.1% of patients, respectively. In the period before CCRT, 96.9% of patients required tooth extraction. The median number of teeth extracted during the pretreatment phase was 3 (range: 0-11), and the median interval between tooth extractions and the initiation of CCRT was 16 days (range: 10-24 days). Patients exhibiting significant weight loss (>5%) accounted for 48.6% of the study population.
Baseline and Treatment Characteristics.

Abbreviations: CAR; C-reactive protein to albumin ratio, WL; weight loss, pre; pretreatment, C-CRT; concurrent chemotherapy, mo; month, post; posttreatment.
As illustrated in Table 1, 79.7% of the patients underwent 2–3 cycles of concurrent chemotherapy during the CCRT course, and 62.4% received an additional 1 or 2 cycles of adjuvant chemotherapy following the CCRT. Furthermore, 67.2% of the patients underwent tooth extraction post-CCRT, with a median of 1 tooth extracted (range: 0-6). The median duration from CCRT to tooth extraction was 8 months (range: 0-24 months).
We used ROC curve analysis to find the cutoff value for CAR that can distinguish between the post-CCRT RITL status of the patients. The ideal cutoff value we found for RITL was 3 g/dL, which divided the whole cohort into two groups: Group 1 (CAR < 3) with 136 patients and Group 2 (CAR ≥ 3) with 187 patients [Area under the curve (AUC): 83.0%, sensitivity:83.6%, specificity: 81.4%, J-index: 0.650] (Figure 2). Comparing the two CAR groups, we found that patients with a CAR ≥ 3 had significantly higher RITL rates than their CAR < 3 counterparts (77.0% vs 53.7%, p = 0.006). Previously, Fearon and colleagues established the cutoff for significant WL as > 5% within the last 6 months in the international consensus guideline. 19 This criterion, employed in the initial CARWL study by Topkan et al, 10 was similarly adopted in our current study. Accordingly, the study cohort was stratified into two groups: Group 1 (WL < 5%), comprising 166 patients, and Group 2 (WL ≥ 5%), comprising 157 patients. Comparative analysis revealed that patients experiencing significant WL exhibited a higher incidence of RITL compared to those without (75.8% vs 62.7%; p = 0.012) (Table 2). Based on our findings, we categorized patients into four possible groups using their pretreatment CAR and WL status: Group-1: CAR < 3.0 and WL ≤ 5.0%, Group-2: CAR < 3.0 and WL > 5.0%, Group-3: CAR ≥ 3.0 and WL ≤ 5.0%, and Group-4: CAR > 3.0 and WL > 5.0%, respectively. However, since the RITL rates of Groups 2 and 3 were not statistically different from each other (Figure 3), we combined them into one group and created the three-tiered CARWL score: CARWL-0: CAR < 3.0 and WL ≤ 5.0%; CARWL-1: CAR < 3.0 and WL > 5.0%, or CAR ≥ 3.0 and WL ≤ 5.0%; and CARWL-2: CAR > 3.0 and WL > 5.0%. As shown in Figure 3 and Table 2, comparisons between the three groups revealed that the RITL rates gradually and significantly increased from CARWL-0 to CARWL-2 score groups (49.4% for CARWL-0, 64.7% for CARWL-1, and 83.0% for CARWL-2) despite similar distributions of baseline disease and patient characteristics across the groups.

The results of a receiver operating characteristic (ROC) curve analysis investigating the relationship between pretreatment C- reactive protein to albumin ratio values and radiation-induced tooth loss rates after concurrent chemoradiotherapy (AUC: 83.0% sensitivity: 83.6% specificity: 81.4% J Index: 0.650). Note: The blue line represents Receiver Operating Curve; the Red line represents no discrimination line.
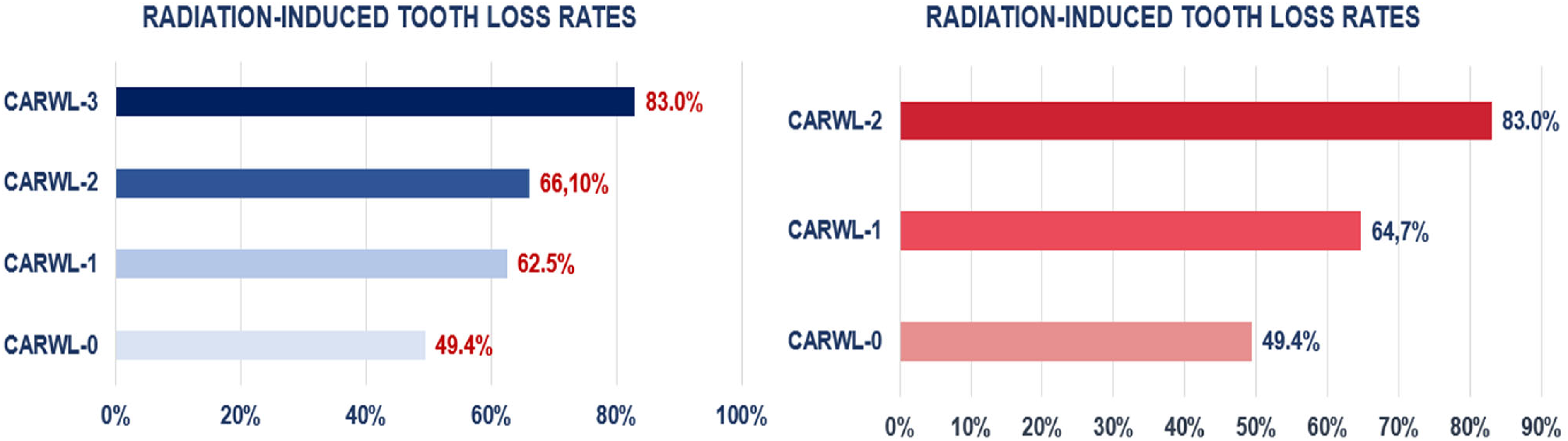
The CARWL Index groups per radiation-induced tooth loss rates.
Results of Univariate and Multivariate Analysis Revealing the Significance Level of Factors on Radiation-Induced Tooth Loss Rates.

Abbreviations: RITL; radiation-induced tooth loss, CAR; C-reactive protein to albumin ratio, WL; weight loss, HR; hazard ratio.
Note: * a; p- value for CARWL-0 versus 1, b; p-value for CARWL-1vs 2, c; CARWL-0 VS 2.
In univariate analysis, we found a statistically significant link between smoking status (54.8% vs 74.0% for yes, p = 0.008), alcohol consumption status (58.3% vs 73.3% for yes, p = 0.003), number of concurrent chemotherapy cycles (56.7% vs 69.9% for 2-3, p = 0.014), CAR group (53.7% vs 77.0% for ≥ 3 g/dL, p = 0.006), significant WL status (62.7% vs 75.8% for WL ≥ 5%, p = 0.012), and CARWL groups (49.4%, 64.7%, 83.0% for CARWL-1, 2, and 3 p˂0.001) and RITL rates. The results from the multivariate analysis confirmed that the connection between RITL rates and smoking status (p = 0.011), alcohol consumption status (p = 0.005), number of concurrent chemotherapy cycles (p = 0.022), significant weight loss status (p = 0.021), CAR group (p = 0.007), and CARWL groups (p ˂ 0.001 for each comparison) remained significant (Table 2).
Discussion
The primary objective of this investigation was to determine the potential of the recently introduced CARWL index in accurately predicting the rates of RITL in LA-NPC patients undergoing radical CCRT and categorizing them into RITL risk groups. Our findings demonstrated that the innovative CARWL index was capable of stratifying these patients into three distinct risk groups with significantly different RITL rates: 49.4%, 64.7%, and 83.0% for the CARWL-0, CARWL-1, and CARWL-2 groups (P < 0.001), respectively.
In addition to introducing the novel CARWL index as a predictor of RITL, the present study identified three risk factors significantly associated with increased RITL rates after definitive CCRT in LA-NPC patients. The first of these was smoking, indicating that patients with a smoking habit had a higher rate of RITL compared to those without (74.0% vs 54.8% for non-smokers, p = 0.011). This finding aligns with the research by Mai and colleagues, which showed that former smokers were more likely to lose teeth than never-smokers (OR = 1.34). 21 When RT-related inflammation combines with smoking-induced inflammation, it is posited to cause compromised oxygenation and hindered healing processes. Due to their synergistic detrimental effects on periodontal and bone tissues, these factors are thought to contribute to complications such as post-CCRT tooth loss.6,22 Alcohol consumption was the second risk factor to be linked to a notably higher RITL rate (73.3% vs 58.3% for non-consumers; p = 0.005) in our study. Alcohol consumption significantly increases the risk of tooth decay and loss. Patients who drink excessively are three times more likely to experience tooth loss due to the formation of more dental plaque compared to those who do not drink excessively. 23 Dasanayake et al 23 suggested that the potential impact of alcohol on tooth loss could be contingent upon alcohol-induced dry mouth, inadequate oral hygiene, insufficient oral care, consumption of a cariogenic diet, and elevated oral acidity resulting from vomiting.
Moreover, alcohol increases levels of inflammatory cytokines in the circulation and contributes to local and systemic inflammation, a well-established cause of periodontitis and tooth loss. 24 Given that alcohol-induced hyperinflammation may exacerbate the adverse effects of RT and CCRT on teeth and associated structures, 25 it is rational to anticipate heightened incidences of RITL following CCRT among individuals who consume alcohol. The final factor that was observed to increase RITL rates was the higher concurrent chemotherapy cycles in our research (69.9% for 2-3 cycles vs 56.7% for 1 cycle p = 0.014). Chemotherapy may elicit adverse effects on the oral mucosa, salivary glands, and tooth enamel, leading to conditions such as xerostomia, dental caries, and a spectrum of dental complications, ultimately culminating in tooth loss. Therefore, considering these actions together with the additional tissue-sensitizing effects of the chemotherapy, it is not surprising that a higher number of chemotherapy cycles may result in more severe and long-lasting tooth problems, leading to increased rates of RITL.
Our research yielded a significant outcome that has not yet been documented in the existing literature. We presented the first evidence that the novel CARWL index efficiently stratifies LA-NPC patients into three RITL risk groups following CCRT (p < 0.001). Accordingly, the rates of RITL incidence were 83.0%, 64.7%, and 49.4% in the CARWL-2 (P < 0.001), CARWL-1 (P = 0.005), and CARWL-0 (P = 0.003) groups, respectively. Despite the need for confirmatory research results, this finding suggests that when both the CAR and significant WL are unfavorable, more than 80% of those patients experience detrimental RITL at some point during the follow-up period. Given the potential for RITL to adversely impact dental functions, increase the risk of osteoradionecrosis, diminish the quality of life, contribute to malnutrition, and negatively influence survival rates in HNC patients, it is imperative to prioritize more frequent dental examinations, proactively implement preventive measures, and deliver comprehensive oral hygiene education to individuals within the CARWL-1 and CARWL-2 groups, who are particularly susceptible to RITL.3,6
Although it is challenging to determine the exact cause of the strong connection between the CARWL groups and RITL rates following CCRT in LA-NPC patients without similar research, analyzing the individual impact of CRP, albumin, their combination CAR, and significant WL on RITL incidence can provide some reasonable insights. The CRP serves as a significant indicator in various medical conditions, revealing both inflammatory and nutritional states. 26 Elevated CRP levels signify widespread inflammation throughout the body, which may contribute to the onset of several chronic illnesses, including periodontal diseases. 27 Persistent inflammation is pivotal in advancing periodontal disease, culminating in tooth loss. Correlations have been drawn between elevated CRP levels and severe periodontitis, indicating that systemic inflammation can potentially exacerbate localized inflammatory responses in the periodontal tissues. 28 It has been reported that patients with 3 mm or more attachment loss have a higher proportion of CRP levels above 3 mg/L compared to patients with 2–3 mm attachment loss and those with no attachment loss (38.0% vs 23.7% vs 16.9%; P < 0.001). 29 This finding suggests that both the loss of attachment supporting the teeth and increased inflammation, a significant factor in tooth loss, may lead to a higher rate of tooth loss in patients with high initial CRP. Additionally, this inflammation may become more aggressive with RT, leading to higher rates of RITL. 30 Likewise, decreased albumin levels, the second component of CAR, indicate compromised nutritional status and exacerbated chronic inflammation. 31 Albumin also has the potential to inhibit or lessen tooth decay owing to its molecular weight, which closely resembles that of protective pellicle proteins. Due to their substantial size, the cystatin, statherin, histatin, and proline-rich pellicle proteins cannot permeate the enamel pores. Instead, they adhere to hydroxyapatite, promoting mineral ingress for remineralization while preventing efflux, thus stabilizing the hydroxyapatite crystals within the enamel. It is widely acknowledged that individuals with elevated albumin levels demonstrate reduced incidence of tooth decay, presumably due to the structural similarities shared between these protective molecules and albumin. Consequently, it is reasonable to postulate that hypoalbuminemia may similarly augment RITL rates in head and neck cancer patients.32,33 A low albumin level also implies an impaired nutritional status, which can weaken the immune response and tissue repair mechanisms, leading to increased susceptibility to infections and periodontal diseases. 33 For instance, Jhon et al 34 found that patients with low albumin levels had higher rates of periodontal attachment loss in a cohort of 50 HNC patients, a leading cause of tooth loss in the population, including the HNC patients. Furthermore, Yoshihara et al 11 noted a high incidence of tooth loss in older adults with hypoalbuminemia at the outset, suggesting a relationship between low albumin levels and subsequent tooth loss in their study. In addition, a study conducted by Majon et al 35 showed that patients with low serum albumin levels had more teeth with a depth of 6 mm in the periodontal pocket and increased tooth mobility compared to patients with normal serum albumin levels, suggesting a direct and robust relationship between albumin levels and tooth loss. Although CAR, a combination of CRP and albumin, has not been investigated for its association with RITL in head and neck cancer patients, recently Somay et al 36 demonstrated that the novel GLUCAR index, which combines fasting glucose and CAR measures, effectively predicted tooth loss after CCRT in a similar group of patients included in our current study. Providing indirect support for the impact of CAR on RITL rates, the authors showed that post-CCRT tooth extractions were more prevalent in the group with higher GLUCAR measures compared to the group with lower GLUCAR measures (84.4% vs 47.4%; p < 0.001). Also, significant WL, an essential component of the CARWL index, affects tooth loss. Malnutrition, one of the considerable causes of WL, causes insufficient intake of the nutrients required to maintain the health of teeth and periodontal tissues. It has been reported that teeth become weaker, the likelihood of tooth decay and periodontal disease increases, and severe tooth decay that progresses over time may lead to tooth loss. 10 As this is the first study of its kind in this field, we are unable to compare our results with those of similar studies. However, despite the necessity for confirmatory research, our findings indicate that the CARWL index is a comprehensive measure that effectively captures the combined influence of CAR and WL on RITL rates in radically treated LA-NPC patients.
The current research is subject to several limitations. First, it was based on data obtained from retrospective analyses within a single institution and had a study population of relatively small size. This characteristic presents the potential for inadvertent selection biases commonly associated with research of this nature. Second, the absence of a validation cohort may have constrained our capability to explicate our findings comprehensively, highlighting the need for further research in this area. Third, given that our study exclusively examined data obtained at a specific juncture, specifically the initial day of C-CRT, it is crucial to recognize that the current CAR cutoff value may not accurately delineate the optimal cutoff for effectively stratifying the risk of LA-NPC patients. This is because albumin and CRP levels can vary significantly during and after C-CRT. And fourth, we may have overlooked the opportunity to establish reliable cause-and-effect relationships between a group exhibiting a higher CARWL score and the levels of cytokines/chemokines, nutritional status, and immune-inflammatory indicators, such as IL-1, IL-6, and TNF-α. As a result, it is imperative to acknowledge that the conclusions presented in this study should be considered hypothetical and not as definitive recommendations until further well-designed, multi-center, and large-scale research studies addressing these crucial topics offer substantiating evidence. Nevertheless, the elements of the CARWL index are readily obtainable, easily calculable, cost-effective, and exhibit consistent characteristics, rendering this index a feasible biomarker for regular clinical utilization. Thus, notwithstanding the previously outlined limitations, the recently devised CARWL index can stratify LA-NPC patients into risk categories based on their likelihood of experiencing RITL. If subsequent research substantiates its efficacy, the widespread adoption of this approach may facilitate the meticulous monitoring of high-risk individuals and the prompt implementation of preventive interventions to mitigate tooth loss at earlier stages.
Conclusion
Our research findings indicate that the recently created CARWL index is a reliable biomarker that effectively forecasts the incidence rates of RITL in patients with LA-NPC. If subsequent research corroborates the findings delineated in this study, this innovative biological marker may herald a significant advancement in the identification of individuals at elevated risk, potentially improving current practices one step further and paving the way for the formulation of efficacious preventive strategies and post-assessment protocols.
Footnotes
Abbreviations
Acknowledgements
None
Author Contributions
E.S., E.T., S.B., D.O., S.S., N.K.D., and U.S. wrote the main manuscript text, and: E.S., E.T., S.B., D.O., S.S., N.K.D., and U.S. prepared figures. All authors reviewed the manuscript.
Availability of Data and Materials
For researchers who satisfy the criteria for access to sensitive data, the datasets utilized and/or analyzed during the current study are accessible from the B.U. Department of Radiation Oncology Institutional Data Access.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval and Consent to Participate
Before acquiring any information from the patient, the study design has been approved by the Institutional Review Board of Baskent University School of Medicine and has complied with the Declaration of Helsinki (DKA:20/58). We ensured that all patients signed an informed consent form before the beginning of the evaluation, either themselves or their legally authorized representatives for the acquisition and analysis of the patient's sociodemographic, dental, and medical records; blood samples, and publication of the outcomes.