
Abstract
Objectives
To investigate risk factors for the early recurrence (ER) of hepatocellular carcinoma (HCC) after radical resection based on preoperative contrast-enhanced ultrasound (CEUS) and clinical features to provide guidance for clinical treatment.
Methods
The retrospective analysis selected 130 HCC patients who underwent radical tumor resection from October 2019 to November 2021. All patients underwent preoperative routine ultrasound examination and CEUS, and the pathology was confirmed as HCC after surgery. The patients were divided into two groups based on whether there is an ER, namely the ER group and the non-ER group. The general clinical, routine and CEUS data of patients were collected, and the factors were selected by using the least absolute shrinkage and selection operator (LASSO) regression. Multivariate logistic regression was used to screen the independent influencing factors of ER. Then a nomogram model was established to predict the risk of ER, and the application value of nomogram through internal validation was evaluated.
Results
Multivariate logistic regression identified several independent factors influencing ER after radical HCC resection. Significant factors included early wash-out phase (95%CI = 0.003-0.206, P = 0.001), liver cirrhosis (95%CI = 2.835-221.224, P = 0.004), incomplete envelope (95%CI = 5.247-1056.130,P = 0.001), multiple lesions (95%CI = 1.110-135.424,P = 0.041), Albumin <40 g/L (95%CI = 2.496-127.223,P = 0.004), and Golgi Protein 73 (GP73) ≥ 85 ng/mL (95%CI = 1.594-30.002, P = 0.010), with all P-values <0.05. The nomogram prediction model constructed based on the results of multivariate logistic regression, demonstrated a ROC curve AUC of 0.879, a sensitivity of 93.5%, a specificity of 66.7%, and a C-index of 0.602, indicating superior diagnostic efficiency compared to independent influencing factors. The ER nomogram prediction model confirmed good discrimination and calibration in internal validation.
Conclusion
The CEUS-Clinical combined model effectively monitors the risk of ER in high-risk populations following radical resection of HCC, timely interventions to improve patient prognosis.
Advances in Knowledge
This study employed CEUS as a non-invasive diagnostic examination aid in assessing the risk of ER after surgical resection of HCC, enhancing the model's reliability and stability.
Introduction
The latest statistics of global tumor epidemiology indicate that hepatocellular carcinoma (HCC) is one of the most common fatal malignant tumors worldwide, with its incidence and mortality rank among the top five in China.1,2 Hepatectomy and liver transplantation are the primary treatment options for patients with HCC. 3 However, due to the shortage of liver donors, radical surgical resection has a wider range of clinical applications. With the continuous improvement of medical technology, postoperative complications and mortality have shown a downward trend over the years, while the postoperative early recurrence (ER) rate remains high. 4 Therefore, the severe problems that clinicians and patients are faced with are the high ER rate after radical HCC resection and the difficulty of secondary surgery.. 5 ER refers to the rediscovery of HCC lesions within two years after radical HCC resection. 6 Chan AWH et.al. suggested that tumor characteristics such as tumor diameter more than 5 cm, incomplete envelope, microvascular invasion are independent risk factors of ER. 4 Accurately predicting the risk of ER before surgeryis crucial for reducing the ER rate following radical HCC resection.
Conventional ultrasound examination and improved ultrasound technology have been more widely used in the diagnosis and treatment of liver cancer due to their advantages of non-invasive, economical and radiation-free. 7 However, conventional ultrasound may ignore tumor heterogeneity information and provide relatively few characteristic indicators. Compared with conventional ultrasound, contrast-enhanced ultrasound (CEUS) detects some clues as to residual active lesion such as rapid wash-in and wash-out characteristics of CEUS in HCC with high LI-RADS grading, rapid portal phase signal regression, and low differentiation are associated with ER after radical HCC resection. 8
Most previous studies combined clinical features to construct liver cancer risk assessment models, such as the PAGE score based on age, sex, and the platelet count in the Caucasus region; THRI model based on PAGE score adding cirrhosis etiology in the Toronto area; and the Korean model added albumin levels based on PAGE scores.9–11 The clinical research of the combination of CEUS and clinical factors to predict ER after radical HCC resection has not been reported. Therefore, we conducted a retrospective study based on serological level and tumor characteristics shown by preoperative ultrasound and CEUS to explore potential risk factors for ER after radical HCC resection. This will help improve treatment plans and patient prognosis.
Materials and methods 12
Patients
A total of 189 patients who underwent radical HCC resection initially from October 2019 to November 2021 was retrospectively selected. Preoperative diagnosis of HCC was based on the criteria of the American Association for the Study of Liver Diseases. 13 All patients received routine ultrasound and CEUS before operation. Inclusion criteria were: (1) initial tumor detection; (2) completion of preoperative CEUS and abdominal computed tomography (CT) examination; (3) patients were received surgical treatment within 2 weeks after CEUS without adjuvant therapy before and after surgery; (4) postoperative pathology confirmed HCC; (5) Child-Pugh grade ranked A to B. Exclusion criteria were: (1) absence of clinical and CEUS data; (2) failed to achieve R0 resection (the lesion was completely removed, no tumor cells could be found on the incision margin under the microscope and the naked eye or microscope); (3) patients suffering from other neoplastic diseases; (4) patients lost follow-up or died.
According to the exclusion criteria, this study included 130 patients who were divided into ER group (31 cases) and non-ER group (99 cases) based on ER (Figure 1). This study has been approved by the Ethics Committee (approval no.2023-SR-818), and all patients signed written informed consent prior to CEUS examination.

Inclusion and exclusion criteria flow charts.
Data Collection
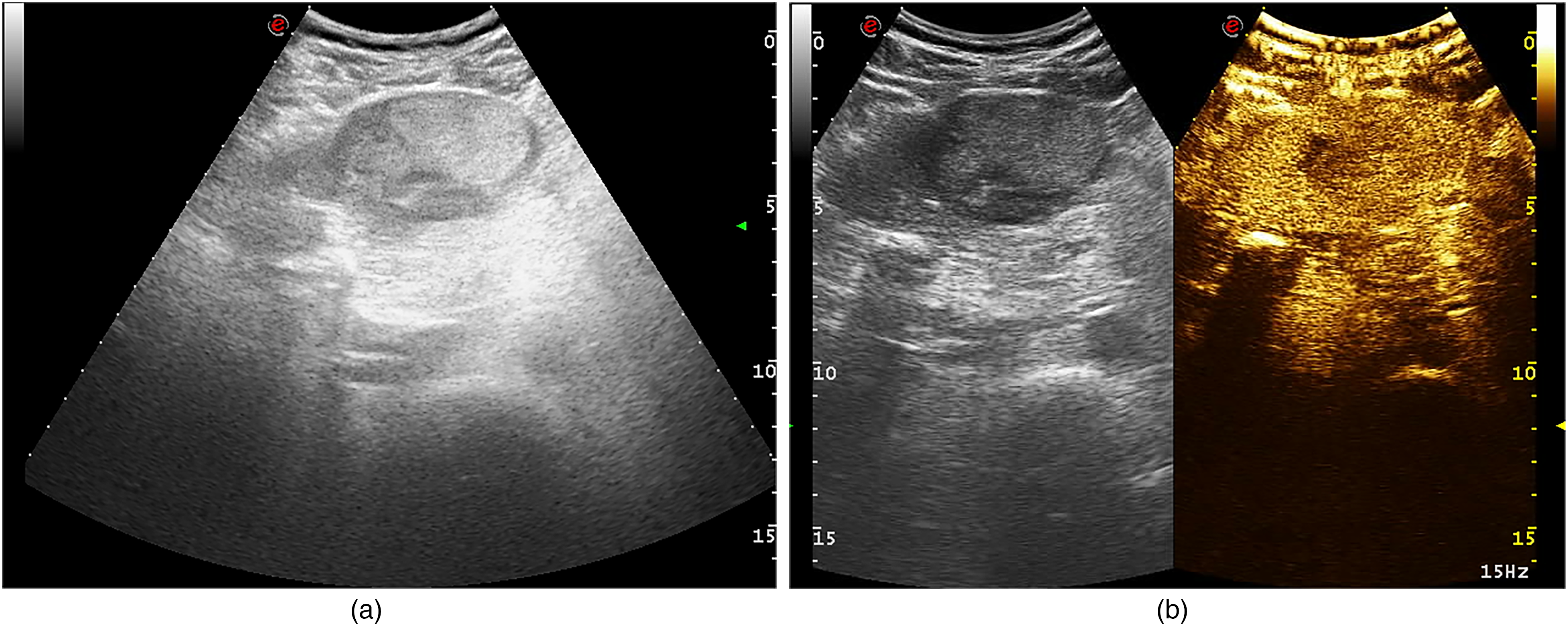
Male patient, 65-year-old, preoperative 2D ultrasound revealed solitary lesion in the left lobe of the liver, with complete capsule and no evidence of liver cirrhosis, and CEUS indicated late wash-out phase.
Postoperative Monitoring and Evaluation
In the first month after surgery and every 3 months thereafter, the review includes AFP levels and liver ultrasonography. If any abnormalities are detected in the above examinations, abdominal dynamic enhanced CT or magnetic resonance imaging (MRI) scan will be further conducted to confirm the diagnosis of recurrence. The follow-up period starts from the date of surgery and the end point was tumor recurrence or two years after surgery. Early recurrence of HCC was defined as the reappearance of HCC lesions within 2 years after radical HCC resection, with new lesions identified through CEUS, enhanced CT, or enhanced MRI showing typical imaging findings of HCC. The data was reviewed on February 14, 2024.
Statistical Analysis
R 4.3.2 and MedCalc18.2.1 were used as statistical software. Factors were selected by using the least absolute shrinkage and selection operator (LASSO) regression. Based on the characteristics of non-zero coefficient in LASSO regression model, multivariate logistic regression was applied to screen the independent influencing factors of postoperative ER in order to construct CEUS-Clinical joint risk prediction nomogram model. The C-index and calibration curve were used to evaluate the discrimination and calibration of the nomogram. To quantify the discriminability of the nomogram model, the original data row Bootstrap method (repeated sampling 1000 times) was included for internal validation to calculate the C-index, and DCA curve was plotted to determine the clinical usability of the nomogram. Furthermore, MedCalc18.2.1 was used to compare with each independent influencing factor. P < 0.05 was considered to be statistically significant.
Results
Patient Characteristics
In this study, 31 patients (23.8%) had the status of ER after surgery, and 99 patients (76.2%) were not subjected to have ER after surgery. The clinical and CEUS characteristics of the patients are presented in Tables 1–3.
Comparison of Clinical Characteristics Between the ER Group and non-ER Group

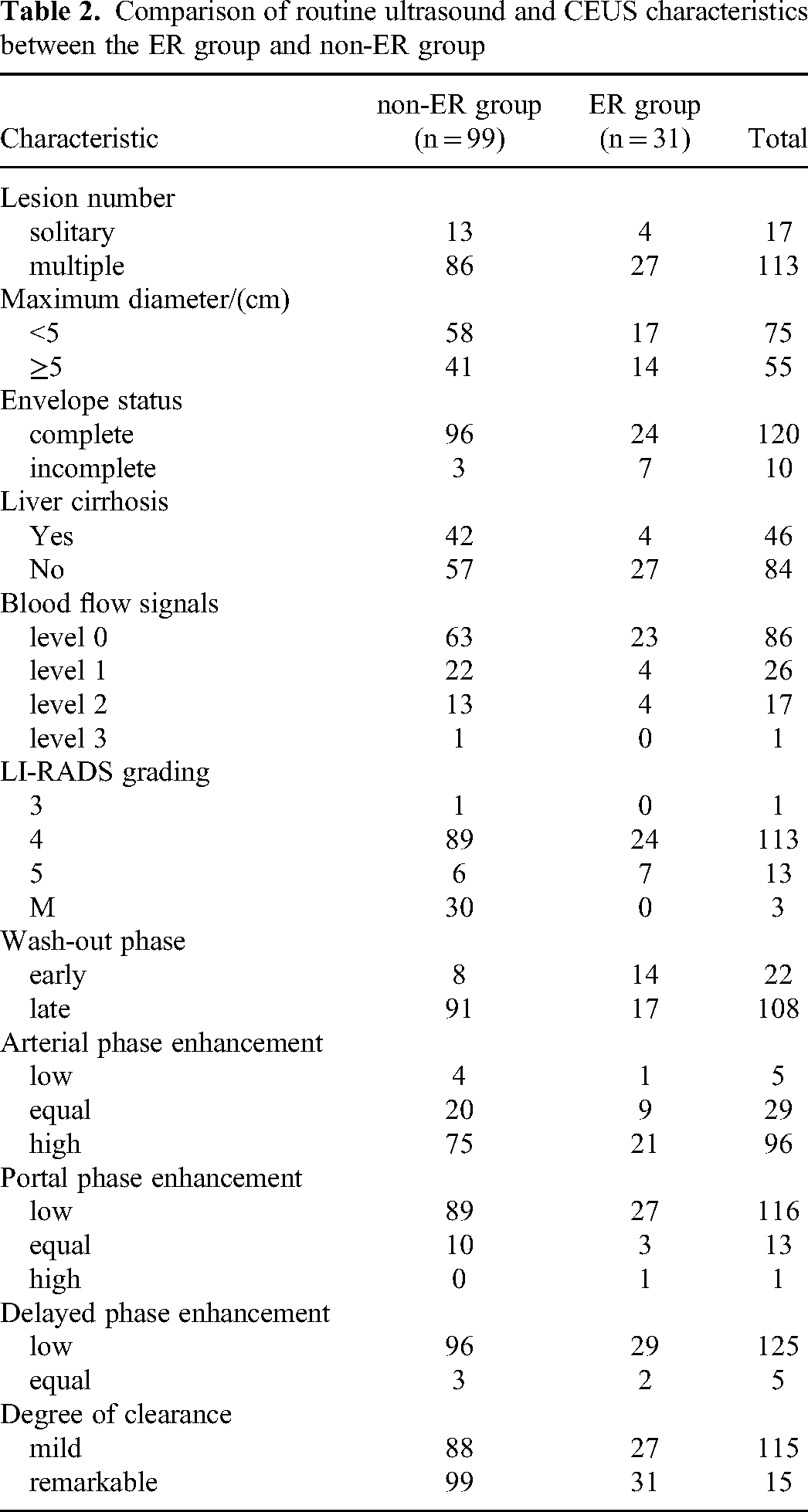
Comparison of routine ultrasound and CEUS characteristics between the ER group and non-ER group
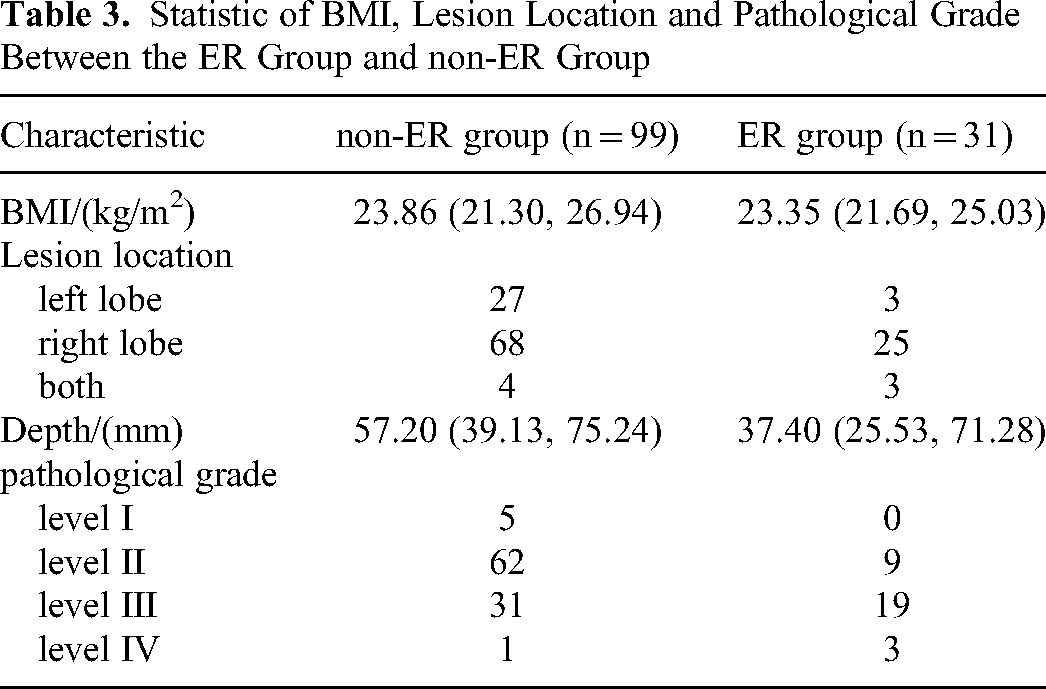
Statistic of BMI, Lesion Location and Pathological Grade Between the ER Group and non-ER Group
Features Selection
Among the clinical and CEUS features of patients, 13 factors showed non-zero coefficients in LASSO regression (Figure 3), including Albumin, PLT, GP73 and AFP level, age, gender, lesion number, envelope status, liver cirrhosis, LI-RADS grading, wash-out phase, arterial phase enhancement, portal phase enhancement. The results of multivariate logistic regression analysis indicated that cirrhosis during the early wash-out phase (95%CI = 0.003-0.206, P = 0.001), liver cirrhosis (95%CI = 2.835-221.224, P = 0.004), incomplete envelope (95%CI = 5.247-1056.130, P = 0.001), multiple lesions (95%CI = 1.110-135.424, P = 0.041), Albumin < 40 g/L (95%CI = 2.496-127.223, P = 0.004), and GP73 ≥ 85 ng/mL (95%CI = 1.594-30.002, P = 0.010) were independent influencing factors of ER after radical HCC resection (Table 4).

Selection of feature parameters. a: Select the optimal parameter (λ) in the LASSO model by the minimum criteria using 5-fold cross-validation. Plot the partial likelihood deviation (binomial deviation) against the logarithm (λ). Draw a vertical dashed line at the entry value corresponding to a standard error (1 + SE) of the minimum quasi difference and minimum standard deviation. b: Plot a coefficient curve for 17 characteristics in LASSO. Use a logarithmic(λ) sequence and draw a vertical line at the value selected through 5-fold cross-validation, resulting in 13 features with non-zero coefficients.
Multivariate Logistic Regression Analysis of Independent Risk Factors for ER After Radical Resection of HCC

Nomogram Model Construction and Clinical Validation
The results of the multivariate logistic regression analysis revealed that wash-out phase, liver cirrhosis, envelope status, lesions number, Albumin, and GP73 level were independent influencing factors. A nomogram was constructed using above 6 factors to predict the probability of ER occurrence. Each predictor was proportionally assigned to a score based on its OR value from the primary multivariate logistic regression analysis, and its total score was used to determine patient's risk of developing ER (Figure 4). The C-index of the predicted nomogram model was 0.602, with AUC of 0.879, a sensitivity of 93.5%, a specificity of 66.7%, indicating superior diagnostic efficiency compared to independent influencing factors (Table 5). In the internal validation, the nomogram obtained a high C-index after 1000 Bootstrap preharvest, indicating a good degree of differentiation. There is no significant deviation between the predicted probability and the probability of actual occurrence of the calibration chart. DCA results demonstrate that the nomogram predicts ER with the net benefit generated, making it valuable for clinical decision-making (Figure 5).

A nomogram model for predicting the risk of er after radical HCC resection.

Clinical validation of the nomogram model. a-b: AUC of ROC curve of CEUS-Clinical model and each individual risk factor. c: The calibration diagram shows that the probability of ER predicted by the nomogram is in good agreement with the actual results. d: The DCA curve shows that the nomogram model produces a net benefit in predicting ER occurrence.
Comparison of the Nomogram Model with the AUC for Each Independent Influencing Factor

Discussion
Currently, there is no international consensus on the predictive model of ER risk stratification after surgical resection of HCC. Most HCC relapse scoring software, such as SLICER score and PLAN-B model, did not have a comprehensive understanding of primary HCC lesions due to the lack of imaging examination. 14 Therefore, clinicians lack accurate judgment of patient prognosis, resulting in affecting further treatment. Although AJCC and TNM stages, as the postoperative prediction model for recurrence, are widely recognized, they over-rely on microvascular invasion which can only be obtained through surgical pathology. 15 At present, most studies evaluate the prognosis of HCC patients after HCC resection through CT and MRI examination, and few clinical studies have reported the application of CEUS to predict the recurrence of HCC after treatment. 16 Although the diagnostic efficacy of enhanced CT and MRI is slightly higher, CEUS provides a low-risk profile for allergies, nephrotoxicity and other side effects. Therefore, this study aims to evaluate the application value of CEUS combined with clinical features in the risk of ER after surgical resection of HCC. The results appear that CEUS combined model has good performance in predicting ER of HCC before operation.
The study by Wang demonstrated that “wash-out phase” is an independent risk factor for ER after HCC surgery. Our findings are consistent with these results. 17 SonoVue contrast agent is a pure blood pool contrast agent, and its clearance is associated with the microcirculation perfusion of the lesion. Hepatic arterial blood supply is dominated and portal vein blood supply is minor in low/undifferentiated HCC, resulting in faster removal of contrast agents from hepatic veins and thus faster clearance than in highly differentiated and moderately differentiated HCC. Our study revealed that most HCC patients with ER had low pathological differentiation (according to postoperative pathology, grade III and IV accounted for 71.0% of pathological differentiation in this study, Table 3), abundant internal hepatic arterial blood supply, rapid regression of contrast agents in HCC, and short clearance time. Meanwhile, non-ER patients have a high degree of pathological differentiation (according to postoperative pathology, grade I and II accounted for 67.7% of pathological differentiation in this study, Table 3), and the portal vein remains the primary blood supply to the tumor due to insufficient angiogenesis. Additionally, there is a significant presence of liver blood sinuses within the tumor in non-ER patients, which exhibits slow regression or even persist into the portal and delayed stages, leading to prolonged clearance time. For patients with high BMI, CEUS may be affected by the depth of the lesion, but relevant studies have demonstrated that CEUS can be used with a deep scanning ultrasound probe, and the diagnostic efficacy of evaluating the lesion by detecting the wash-out time is significant. 18 Therefore, SonoVue has a great performance for the non-invasive diagnosis and prognosis for early postoperative recurrence of HCC. If the LI-RADS grade is high and the early wash-out phrase occurs, it indicates high-risk lesions.
The results of routine ultrasound indicated that multiple lesions, incomplete tumor envelope and presence of liver cirrhosis were independent risk factors for ER after radical resection of HCC. Preoperative ultrasound examination of the liver can accurately determine the number and location of the tumor, providing visual representation of tumor, as well as dynamic and repeated observation of the location, depth, shape, boundary, size, number and envelope of the tumor. HCCs located at the right hepatic dome, near the caudate lobe or inferior vena cava, or on the surface of the left lateral segment are more likely to be missed on routine ultrasound. Therefore, CEUS should be employed to target these suspected areas. For patients with high BMI or when tumors are situated at greater depths, an intercostal scan with the patient in a prone position may be beneficial. 19 Most studies generally suggest that the prognosis of HCC patients is related to the number of tumors or biological behavior. Multiple HCC lesions are more likely to have satellite or occult metastases due to their extensive involvement. Even after surgical resection of the primary lesion, there is persistent growth and emergence of new lesions, resulting in ER. 20 When the number of HCC lesions exceeds 3, ablation, chemotherapy or targeted therapy should be considered. The completeness of the tumor envelope is associated with the extent of invasion. An incomplete margin suggests more aggressive biological behavior of the tumor cells, including rapid growth and increased invasion. When the outward growth of the tumor breaks through the envelope, it leads to invasion of the surrounding healthy liver tissue and portal system, thus increasing the probability of recurrence. The most common cause of cirrhosis in East Asia is hepatitis B virus infection. According to the World Health Organization, cirrhosis originates in an environment of chronic inflammation and liver tissue damage. It changes the structure of the liver and blood vessels, gradually forming stunted nodules that have the potential to turn into malignant tumors. 21
Some small lesions may go unnoticed by imaging in HCC patients, resulting in ER after surgical resection. High levels of GP73 and AFP serve as biological markers indicating high invasive capacity in HCC. This study demonstrates that GP73 and AFP are high risk factors for ER, with GP73 being an independent risk factor after radical HCC resection. GP73 also called Golgi phosphoprotein-2, is a trans-membrane protein frequently active in liver cancer cells, holds greater diagnostic value for HCC prognosis compared to other tumor types. 22 The dynamic changes in GP73 reflect the impact of HCC resection and TACE, serving as a predictor for ER or liver disease progression. 23 When the tumor recurred, there is a notable increase in the surface expression of epithelial cell-associated GP73, leading to significantly elevated serum levels which can be utilized as a novel serum tumor marker for detecting ER. Additionally, Liu et al revealed GP73 competed with prolyl hydroxylase-2 in the inhibitory pathway through fundamental studies that, which is anticipated to become a novel target for anti-angiogenic immunotherapy in patients with HCC. 24 The higher AFP level, the more aggressive the tumor is. Preoperative serum AFP level correlates with the likelihood of tumor infiltration into blood vessels to form MVI, thus playing a crucial role in differentiating tumor differentiation and predicting prognosis. 25 Thus, clinical investigators are actively seeking and validating the combination of AFP vaccine and immune checkpoint inhibitors to slow the progression of HCC. 26 Clinicians can assess treatment efficacy by monitoring trends in AFP levels: patients with preoperative AFP >1000 ng/mL face heightened risk for ER. The level of prothrombin induced by vitamin K absence or antagonist-II (PIVKA-II) is extensively correlated with pathological features representing tumor cell distribution and adverse prognosis. 27 Des-Gamma-Carboxyprothrombin (DCP) is associated with early HCC recurrence after liver transplantation. 25 Subsequent studies will integrate potential biological markers such as AFP-L3, PIVKA-II, and DCP to enhance the efficacy of clinical models in predicting ER after surgical resection or liver transplantation.
The study demonstrates that Albumin is an important component of the mPAGE-B, aMAP, and PLAN-B models. Serum Albumin levels have been levels have been improved to have prognostic significance in HCC. Furthermore, the previous finding suggests that Albumin is an independent risk factor for ER after surgical resection of HCC. 28 As a functional protein synthesized by the liver, for one thing, Albumin reflects the differentiated function of hepatocyte. For another, its expression level is negatively correlated with the invasive parameters of HCC. Low levels of Albumin indicate poor differentiation and higher aggressiveness of HCC, while normal levels signify well-differentiated, slow growth. Therefore, Albumin not only serves as an important prognostic factor for HCC patients but also has the potential to modulate the biological behavior of HCC.
Limitations
This was a single-center retrospective analysis conducted in China with most patients having chronic hepatitis B, leading to unavoidable selection bias. Future research will involve multi-center studies and external data validation to confirm the universality and stability of these results. Additionally, future work will focus on developing radiomics or combining other imaging methods to more comprehensively predict recurrence risk and MVI occurrence.
Conclusions
In conclusion, this study established a comprehensive model based on preoperative CEUS in assessing the risk of ER after surgical resection of HCC, which is expected to be used as a reference to effectively screen out high-risk recurrence groups and develop more accurate individualized treatment plans for patients.
Footnotes
Abbreviations
Acknowledgment
The authors wish to thank the medical writers, proof-readers and editors, for their assistance in preforming the ultrasounds used in this publication.
Data Availability
The datasets generated and analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Ethical Approval
This study was approved by the Ethics Committee of the First Affiliated Hospital of Nanjing Medical University (Jiangsu Provincial People's Hospital) on December 19, 2023, with the approval no.2023-SR-818, and all patients signed written informed consent prior to CEUS examination.