
Abstract
Keywords
Introduction
Primary liver cancer (PLC) is the second leading cause of cancer-related death worldwide. 1 Hepatocellular carcinoma (HCC), a common malignancy with increasing worldwide incidence, especially in nondeveloped countries, 2 accounts for more than 90% of PLC cases, 3 appearing almost completely within the setting of chronic liver disease. Most cases of HCC are attributed to chronic hepatitis B in developing countries as well as to nonalcoholic fatty liver disease (NAFLD) and chronic hepatitis C in developed countries. 4 Worryingly, no obvious symptoms appear in the early stages of the disease—the best treatment for which is liver transplantation [Barcelona Clinic Liver Cancer (BCLC) stage 0-A] if the cancer is diagnosed accidentally— but usually in intermediate or late stages when the patient has already lost the opportunity for surgery.
Even though there is a chance for transplantation, patients still suffer from a lack of living donor livers, resulting in hepatectomy bocoming the main treatment for early HCC. According to the latest European Society for Medical Oncology (ESMO) guidelines, with adequate size and function of the remnant liver, resection is recommended for single tumor of any size, and thermal ablation can also be considered for small HCC lesions far from the bile duct. 5 However, the treatment of HCC with Child-Pugh B cirrhosis is still controversial. It is clear that the risk of hepatectomy in HCC patients with Child-Pugh B cirrhosis is significantly higher than in patients that with Child-Pugh A cirrhosis. For that reason, not all patients with resectable HCC and Child-Pugh B cirrhosis are willing to undergo hepatectomy. In addition, there are other reasons for this lack of willingness, such as intolerance of hepatectomy, financial concerns, and religious beliefs (not being able to remove body parts). Therefore, it is essential to search for alternatives to surgical resection for patients with resectable HCC in Child-Pugh B cirrhosis. EASL clinical practice guidelines indicate that ablation is recommended in HCC patients with BCLC stage 0 or A who are not candidates for surgery. 6 Because the long-term outcomes after percutaneous ablation are similar to those after surgical resection, ablation has been proposed as a first-line therapy for HCCs that are <2 cm in size.7,8
Recently, various local ablation techniques, such as radiofrequency ablation, microwave ablation, high-intensity focused ultrasound (HIFU), and cryoablation, have been employed to treat patients with HCC. 9 Compared with other ablation methods, HIFU is the only new noninvasive technique for the treatment of solid tumors. HIFU is performed in vitro and is focused on target tumor tissues in the human body. HIFU results in instantaneous temperature elevation and the induction of coagulative necrosis in tumor cells, which results in the death of target tissues mainly due to the thermal effects, cavitation effects and mechanical effects produced by ultrasonic waves at the target. Some studies have shown that transcatheter arterial chemoembolization (TACE) can reduce the recurrence and metastasis rates of tumors in patients with HCC.10,11 TACE has been widely used in patients with good liver function and patients with tumors that cannot be surgically excised. Obviously, TACE has been the first choice for the nonsurgical treatment of HCC. Certain therapeutic effects can be achieved when HIFU and TACE are used in combination for HCC.12,13 Considering the enhanced efficacy of the combination therapy of TACE and HIFU, it is unclear whether it can also achieve the efficacy of surgical resection in single HCCs with large diameters. Nevertheless, there is increasing interest in the combination of HIFU and TACE for the treatment of HCC, but the effect of combined therapy still needs to be further evaluated. The objective of this study was to compare the treatment effect of surgical resection and TACE combined with HIFU for single HCC with Child-Pugh B cirrhosis. Then, we chose to compare the efficacy of the treatments in small HCC subgroup analysis to explore whether the diameter of HCCs suitable for local combination therapy as the first-line recommended treatment can be expanded to 3 cm.
Materials and Methods
General Information
In this study, we retrospectively analyzed data from 146 patients with single HCC with Child-Pugh B cirrhosis who underwent surgical resection and treatment with TACE combined with HIFU from July 2010 to July 2018, and compared the efficacy and long-term survival rates. Patients were selected according to the following

Flow chart showing the screening procedure for patients with Child-Pugh B cirrhosis single hepatocellular carcinoma (HCC).
This retrospective study was approved by the Research Ethics Committee of the Second Affiliated Hospital of Chongqing Medical University (2019-281). Written informed consent was obtained from all recruited patients to ensure better cooperation. According to the inclusion and exclusion criteria mentioned above, 146 patients were recruited, including males and females aged 23 to 77 years with an average age of 52.0 ± 11.9 years. After disproving relevant taboos and informing the patients and their families of the advantages and disadvantages of the two above treatment methods, the patients voluntarily chose one of the treatment schemes. Patients refused hepatectomy and chose TACE combined with HIFU for various reasons, such as high risk, financial concerns, and religious beliefs. Specifically, 40% of the patients who refused hepatectomy were worried about risk, 25% were intolerant to hepatectomy, 20% had financial concerns, and 15% had contraindicating religious beliefs. Thus, the 146 patients were divided into two groups: 49 patients were treated with TACE combined with HIFU (the combined group), and 97 patients were treated with surgical resection (the resection group). Among them, 27 and 45 patients, respectively, had small HCC tumors (small HCC). Here, small HCC tumors were defined as those measuring less than or equal to 3 cm in diameter with no vascular invasion or metastatic invasion.
Instruments and Methods
Before treatment, all patients underwent relevant examinations, and relevant contraindications were eliminated. The combined group underwent HIFU 4 to 41 days (median 10 days) after TACE, and both treatments were completed in one hospital stay.
TACE was performed through right femoral artery puncture using the Seldinger technique after local anesthesia, and the diameter, number of hepatic tumors and hepatic artery blood supply were determined using digital subtraction angiography (DSA). To intubate the artery supplying the tumor, a catheter was inserted into the opening of the hepatic artery. According to the blood supply of the tumor, the microcatheter was inserted into either the right hepatic artery or left hepatic artery. After the catheter was successfully inserted, chemotherapeutic drugs (loplatin, raltitrexed, bleomycin, mitomycin, pirarubicin, etc) were diluted and infused slowly through the catheter for more than 20 min. For chemoembolization, superlipidated lipiodol and chemotherapeutic agents, in the form of an emulsion, gelatin sponge or polyvinyl alcohol particles, were inserted into the blood supply of the tumor using microcatheters and then embolized with the target vessels.
HIFU was performed using the focused ultrasound tumor treatment system at the HIFU Center, Second Affiliated Hospital of Chongqing Medical University. Under general anesthesia, the tumor tissue was located by B-mode ultrasonography, the target tissue was outlined and transmitted to the computer, and the three-dimensional shape of the tumor was reconstructed to accurately determine its location, size and depth. The lesions was then divided into successive 5 mm sections according to each 5 mm layer, from deep to shallow, until the target area was completely covered (frequency 0.8 MHz, focal length 135.0 mm and 160.0 mm, linear scan 3 mm/s, power 120-240 W, and time 85-300 min). (Figure 2 to 4)

Focused ultrasound tumor therapy system (Type JC): ① Bed of treatment (including ultrasonic positioning system and treatment system); ② Ultrasonic monitor screen; ③ Therapeutic interface.

Image of ultrasound treatment interface.

Image of operation interface.
Surgery was performed after general anesthesia intubation, with the patient in the supine position, head high and feet low, either laparoscopically or open. According to the location and size of the tumor, left or right liver or local liver resection was performed. During the operation, part of the peripheral hepatic toughness band was cut off to fully disentangle the liver. When necessary, intraoperative ultrasound was used to locate the lesion, and a pretangent line was made at a location ≥2 cm from the edge of the tumor with an electric knife. An occlusion band was placed on the first hilum of the liver, which could be occluded if necessary. The lesion was completely removed along the pretangent line with an ultrasonic knife and an electric knife, and any blood vessels and bile ducts encountered were ligated reliably. Electrocoagulation and hemostasis were performed on the remnant liver surface, and the abdominal cavity was irrigated with normal saline. Drainage tubes were placed on the ramnant liver surface, and the incision was sutured layer by layer.
All patients were followed up until death or until December 2020. When a patient was lost to follow-up, PFS and OS were calculated to the date of last follow-up. Follow-up ranged from 4 to 109 (median 39) months.
Statistical Analysis
SPSS version 22.0 statistical analysis software was used for the statistical analyses. Continuous data are represented as (
Results
The overall complications using the Clavien-Dindo classification in the two groups are shown in Table 1. The overall rate of complications was 56.7% in the resection group and 38.8% in the combined group, and the difference was significant (P = .041). The rate of grade I complications was 24.5% in the combination group, which was similar to the 25.8% in the resection group (P = .866). However, the rate of complications above grade I was significantly higher in the resection group (30.9%) than in the combined group (14.3%) (P = .029). The mean operative time in the resection group was 201.3 ± 68.4 min, which was significantly longer than that in the combined group (92.5 ± 40.8 min; P = .015). Additionally, the duration of general anesthesia in the resection group was longer than that in the combined group (201.3 ± 68.4 min vs 38.3 ± 35.5 min: P = .001).
Complications in two groups with Clavien-Dindo Classification

In the combined group, the local recurrence rate was 18.4%, and the de novo HCC rate was 71.4%, while in the resection group, the local recurrence rate was 5.2%, and the de novo HCC rate was 82.5%. The recurrence patterns indicated that the local recurrence rate of the combined group was significantly higher than that of the resection group (P = .039).
Single HCC Tumor Cohort
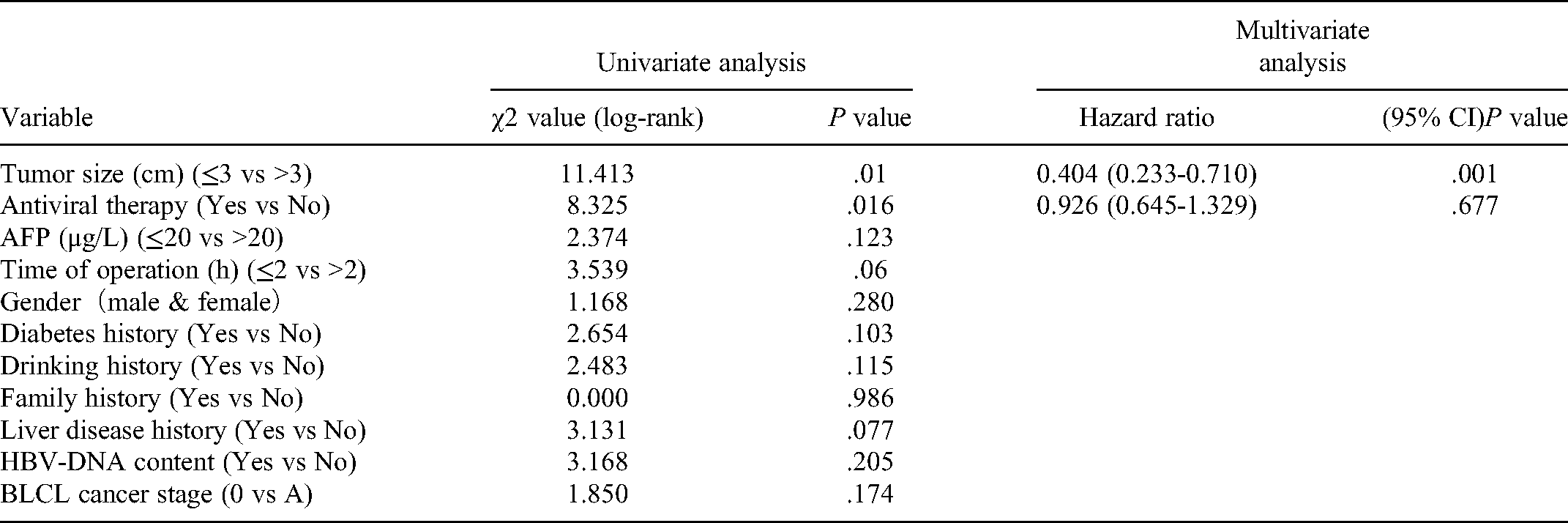
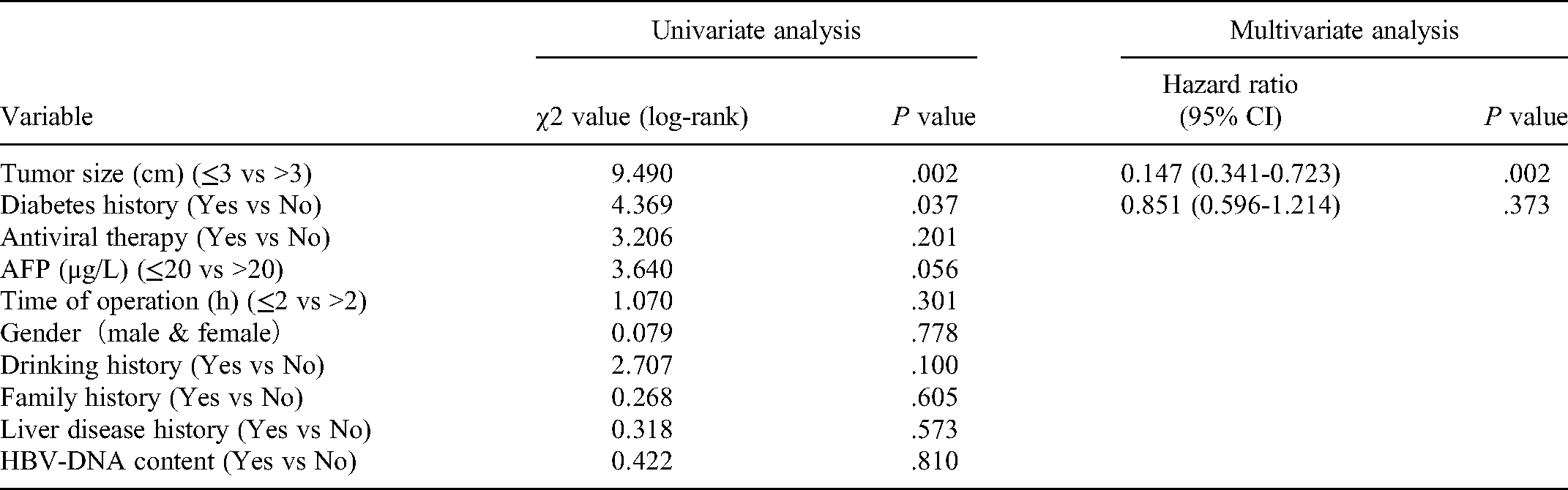
A total of 146 patients (n = 49 in the combined group and n = 97 in the resection group) were included in the study. The combined and resection groups were demographically similar in terms of age, sex, BCLC stage, Child-Pugh classification, tumor diameter, family and personal history of liver disease, diabetes, and alcohol intake, among others (Table 2). There was no significant difference in the OS between the two groups (HR = 0.6379; 95% CI = 0.3737-1.089; P = .0995) (Figure 5a); however, the resection group showed an obviously greater PFS than the combined group (HR = 0.3545; 95% CI = 0.2176-0.5775; P < .0001) (Figure 5b). Univariate analysis revealed that tumor size and antiviral therapy were significant factors for OS from single HCC after treatment, while tumor size and diabetes history were significant factors for PFS. In multivariate analysis, tumor size was an independent prognostic factor for OS (HR = 0.404; 95% CI: 0.233-0.710; P = .001) and PFS (HR = 0.147; 95% CI: 0.341-0.723; P = .002), as shown in Table 3 and Table 4.

(a) Overall survival (OS) of patients with single HCC (P = .650); (b) Progression free survival (PFS) of patients with single HCC (P = .001); (c) Overall survival (OS) of patients with small HCC (P = .763); (d) Progression free survival (PFS) of patients with small HCC (P = .143).
Baseline demographic and clinical characteristics of the patients with single HCC
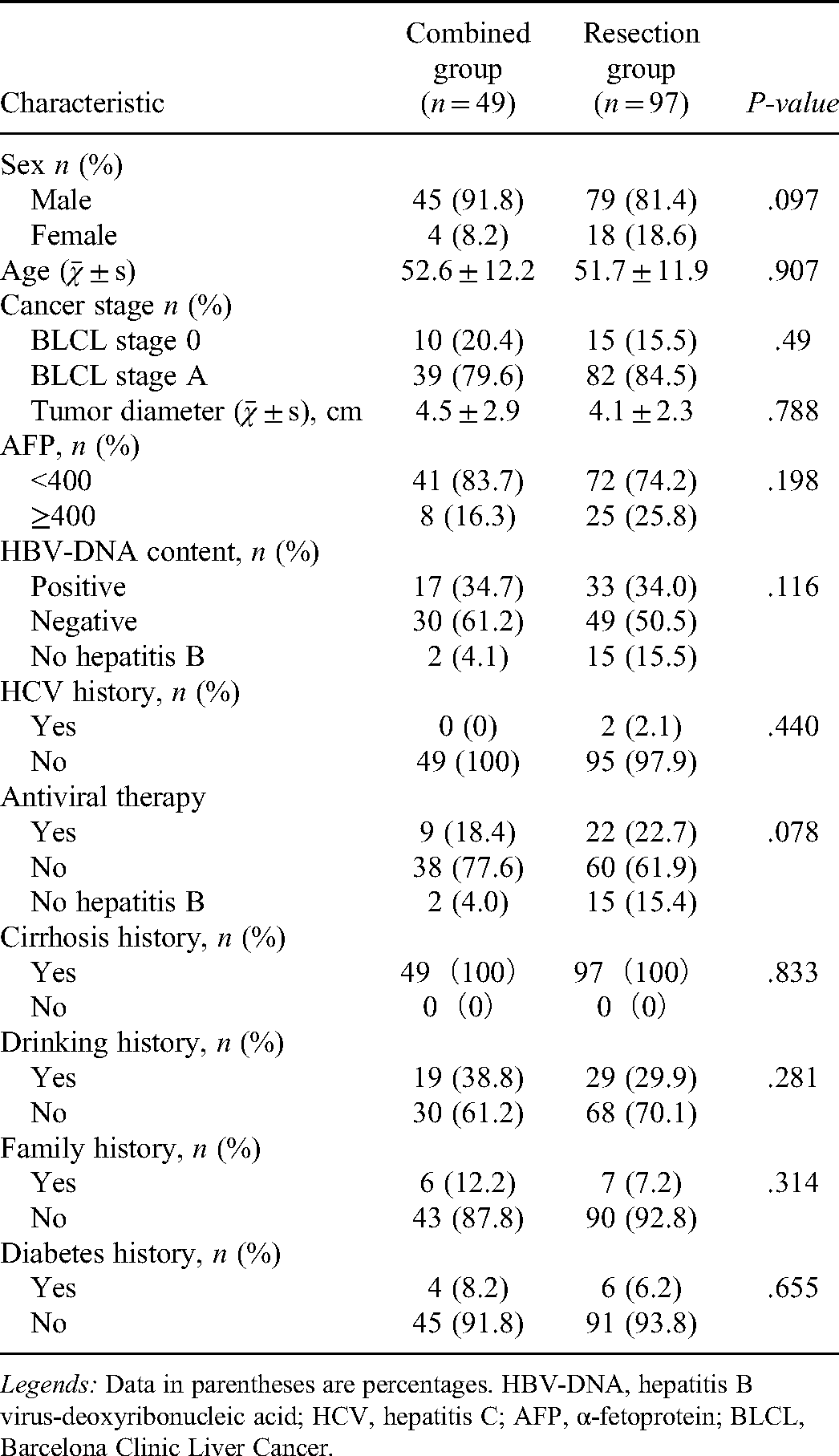
Legends: Data in parentheses are percentages. HBV-DNA, hepatitis B virus-deoxyribonucleic acid; HCV, hepatitis C; AFP, α-fetoprotein; BLCL, Barcelona Clinic Liver Cancer.
Univariate and multivariate analysis of the relative risk of overall survival for single HCC.
Univariate and multivariate analysis of the relative risk of progression-free survival for single HCC.
Small HCC Tumor Cohort
A total of 67 patients (n = 22 in the combined group and n = 45 in the resection group) had small HCCs in this study. The combined and resection groups were demographically similar regarding age, sex, BCLC stage, Child-Pugh classification, tumor diameter, family and personal history of liver disease, diabetes, and alcohol intake, among others (Table 5). The OS was similar in the two groups (HR = 0.8808; 95% CI = 0.3295-2.355; P = .06396) (Figure 5c). However, the PFS was significantly different (HR = 0.4273; 95% CI = 0.1927-0.9473; P = .0363) (Figure 5d). Univariate and multivariate analyses revealed that there were no risk factors for OS from small HCC after treatment, while liver disease history (HR = 0.128; 95% CI: 0.128-0.951; P = .045) and diabetes history (HR = 0.286; 95% CI: 0.095-0.856; P = .025) were significant factors for PFS, as shown in Table 6 and Table 7.
Baseline demographic and clinical characteristics of the patients with small HCC
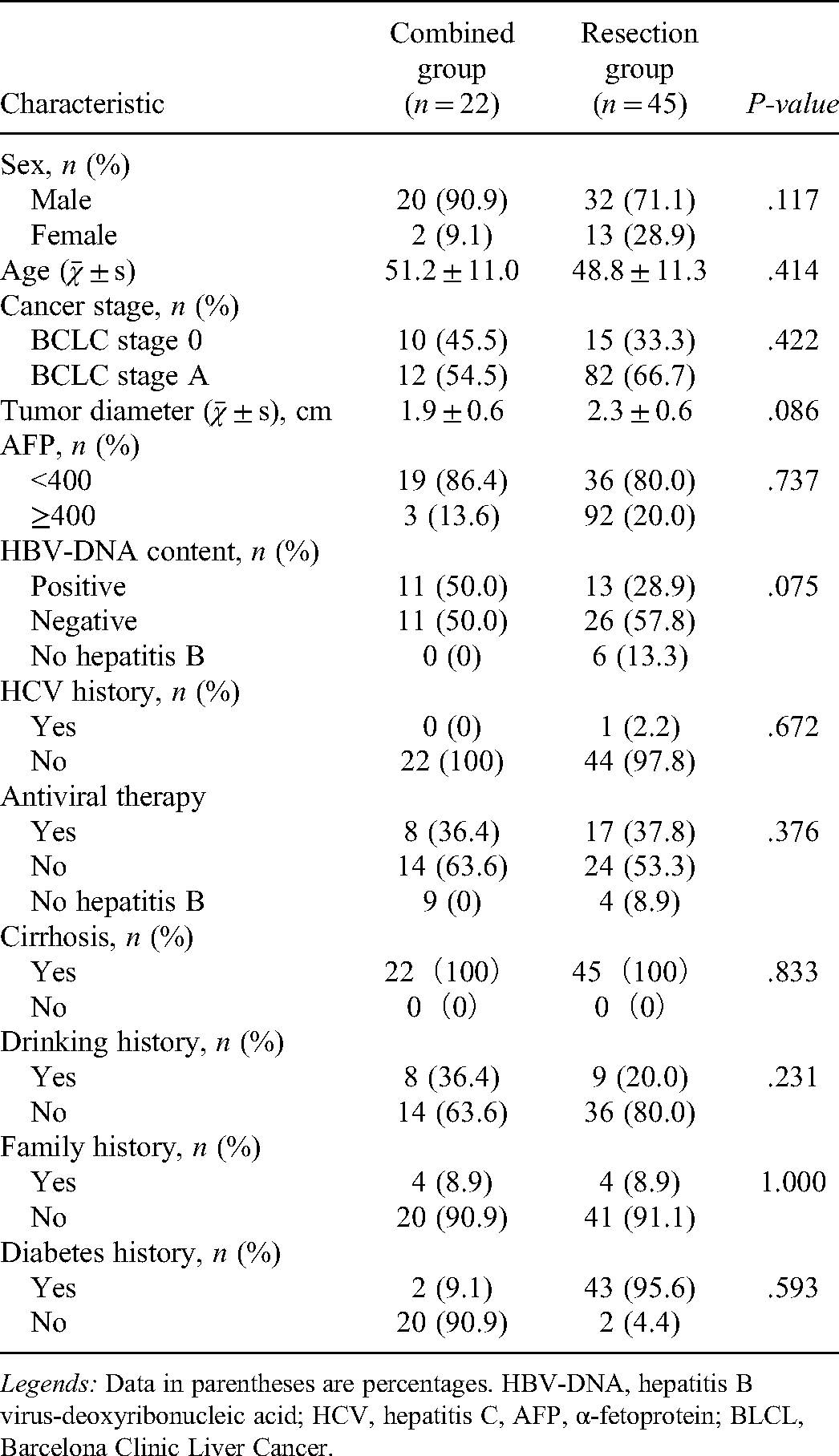
Legends: Data in parentheses are percentages. HBV-DNA, hepatitis B virus-deoxyribonucleic acid; HCV, hepatitis C, AFP, α-fetoprotein; BLCL, Barcelona Clinic Liver Cancer.
Univariate and multivariate analysis of the relative risk of overall survival for small HCC.

Univariate and multivariate analysis of the relative risk of progression-free survival for small HCC.
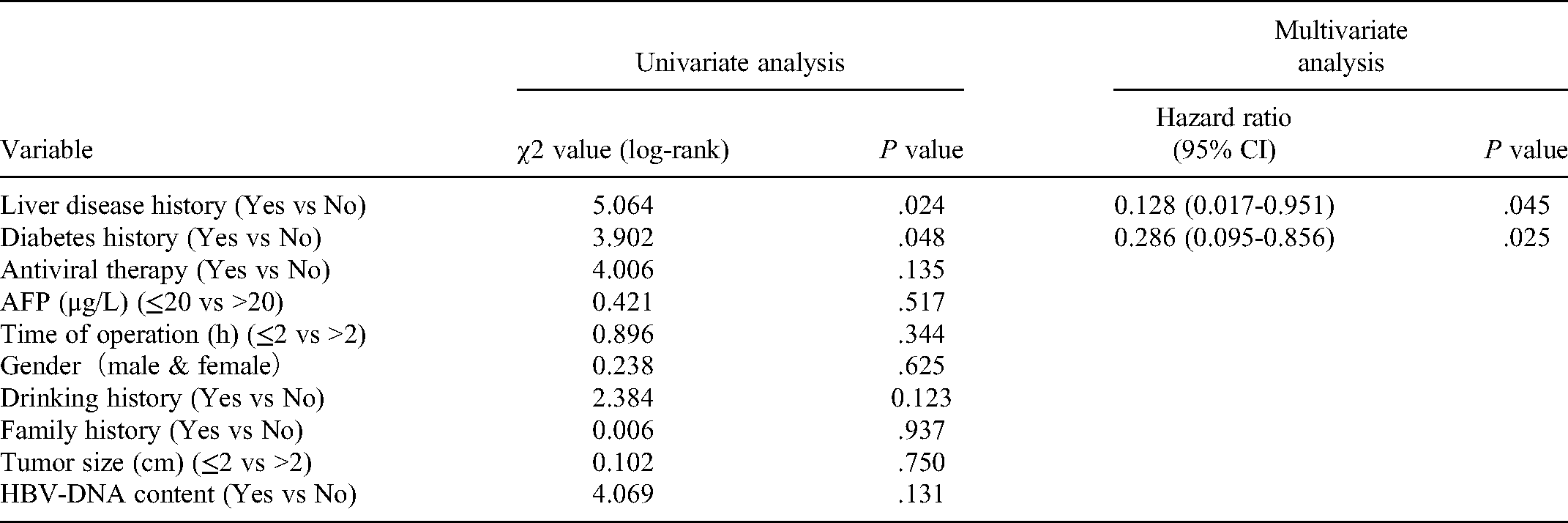
Figure 6 and Figure 7 show the T1W and arterial and portal phase MRI in patients with small HCC before and 6 years after TACE combined with HIFU, respectively. There was no obvious enhancement of the tumor after treatment.

Arterial and portal phases MRI in patients with small HCC before TACE combined with HIFU therapy (preoperative). a: T1WI; b: Arterial phase; c: Portal phase. Black arrow: tumor.

Arterial and portal phases MRI in patients with small HCC 6 year after TACE combined with HIFU therapy (postoperative). (a) T1WI; (b) Arterial phase; (c) Portal phase. Black arrow: tumor.
Discussion
In addition to liver transplantation, hepatectomy is generally accepted as the best treatment for BCLC stage A HCC. However, local ablation is increasingly used for single HCCs that cannot be treated surgically for physical or social reasons. Many studies have confirmed that for small HCC in particular, local ablation therapy is the best treatment option.18–20 In addition, the effect of local ablation combined with TACE is better than that of single treatment.21,22 There are few studies on the role and effects of HIFU as a new noninvasive local ablation method for HCC. As early as 2009 and 2010, studies confirmed the superiority of HIFU combined with TACE for the treatment of large HCC.23,24 Kim et al. showed that combination therapy with HIFU and TACE was more effective than TACE monotherapy for treating HCC tumors < 5 cm in diameter. 25 In the past two years, there has been a gradual recognition of the role of HIFU combined with TACE as a combined minimally invasive procedure. 26 Nevertheless, few studies have compared the curative effect of combination therapy (combined TACE with HIFU) with that of surgical resection in single HCC or single small HCC. To the best of our knowledge, no studies have compared these two treatment methods for single HCC or single small HCC with Child-Pugh B cirrhosis.
The results of the present trial showed that the OS of the resection group was not superior to that of the combined group for either single or small HCC, while the PFS of the resection group was significantly longer than that of the combined group for both single and single small HCC. The therapeutic effect of HIFU can be enhanced after TACE due to hepatic blood inflow occlusion with reduced heat loss. Nevertheless, there may not be a sufficiently wide ablative margin for tumors larger than 3 cm in diameter. This may explain why patients in the resection group had a better PFS than patients in the combined group in the present trial and and why the local recurrence rate of the combined group was significantly higher than that of the resection group.
However, the combined group had an absolute advantage in terms of the duration of operation and of general aneathesia, which is good news for elderly patients with poor tolerance to general anesthesia. HCC lesions are supplied by both the hepatic artery and portal vein, and thus, the blood supply cannot be completely blocked by TACE, which often leads to HCC recurrence. Moreover, after the hepatic artery is blocked in TACE, the portal vein blood supply has been shown to increase in a compensatory manner, and the hepatic artery branch itself has been shown to form extensive communicating branches with the portal vein branch, which is also an important reason explaining the presence of residual tumor cells after TACE. Therefore, TACE alone cannot achieve satisfactory results, and TACE monotherapy cannot be used as the first-line treatment regimen. HIFU utilizes focused ultrasound as energy in the body and converts sound waves into heat energy. Coagulation necrosis of tumor cells is induced by heating the target tissue. Blockage of the blood supply by TACE can compensate for the “heat sink” effect in HIFU; thus, TACE combined with HIFU has a synergistic effect. Luo et al. found that the iodized oil used in TACE exerts a synergistic effect on HIFU, and it can also significantly reduce the energy requirement for irradiation in HIFU treatment. 27 Furthermore, the deposited iodized oil can be used as a target for the focus of HIFU, helping to accurately and quickly localize the target. Therefore, it is more reasonable to perform HIFU after TACE. 28 However, according to Ke S et al. for HCC tumors with diameters larger than 3 cm, ablation is not strongly recommended because of the inability to achieve a sufficiently wide ablative margin. 29 Incomplete ablation increases the chance of tumor recurrence and metastasis, leading to a poor prognosis. 30 However, there was no significant difference in OS between the two groups in this study. The recurrence time of the combined group was significantly shorter than that of the resection group, which greatly affected the quality of life of patients. Compared with the combined therapy, this study shows that surgical resection still has great advantages in delaying postoperative recurrence. However, TACE combined with HIFU is also an effective option for patients with Child-Pugh B cirrhosis who continue to refuse conventional surgical treatment. The survival time after surgery is at least as long as that of conventional surgery.
This study has a few limitations. First, we did not use any tool to estimate the sample size for this study, which was small, as the number of treatments we performed was limited. Second, none of the patients in the combined group received a histological diagnosis. Fortunately, the accuracy of the clinical diagnosis of HCC is high. 31 Finally, this was a single-center study, and the results of the study need to be further confirmed in large-scale, multi-center, randomized clinical trials and through long-term follow-up.
Conclusion
In conclusion, for patients with single or single small HCC, TACE combined with HIFU may not be inferior to surgical resection in terms of the long-term survival rate, while surgical resection still has a definite advantage in terms of delaying recurrence. The increased local recurrence observed with TACE combined with HIFU is associated with the residual tumor following the procedure. In addition, the combination of TACE with HIFU has higher safety than surgical resection.
Footnotes
Acknowledgements
This study was performed by the Department of Hepatobiliary Surgery of the Second Affiliated Hospital of Chongqing Medical University.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Statement
This retrospective study was approved by the Ethics Committee of Second Affiliated Hospital of Chongqing Medical University (2019-281).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China (grant number 81803057).