
Abstract
Purpose
This study aims to investigate the influence of the magnetic field on treatment plan quality using typical phantom test cases, which encompass a circle target test case, AAPM TG119 test cases (prostate, head-and-neck, C-shape, multi-target test cases), and a lung test case.
Materials and Methods
For the typical phantom test cases, two plans were formulated. The first plan underwent optimization in the presence of a 1.5 Tesla magnetic field (1.5 T plan). The second plan was re-optimized without a magnetic field (0 T plan), utilizing the same optimization conditions as the first plan. The two plans were compared based on various parameters, including conformity index (CI), homogeneity index (HI), fit index (FI) and dose coverage of the planning target volume (PTV), dose delivered to organs at risk (OARs) and normal tissue (NT), monitor unit (MU). A plan-quality metric (PQM) scoring procedure was employed. For the 1.5 T plans, dose verifications were performed using an MR-compatible ArcCHECK phantom.
Results
A smaller dose influence of the magnetic field was found for the circle target, prostate, head-and-neck, and C-shape test cases, compared with the multi-target and lung test cases. In the multi-target test case, the significant dose influence was on the inferior PTV, followed by the superior PTV. There was a relatively large dose influence on the PTV and OARs for lung test case. No statistically significant differences in PQM and MUs were observed. For the 1.5 T plans, gamma passing rates were all higher than 95% with criteria of 2 mm/3% and 2 mm/2%.
Conclusion
The presence of a 1.5 T magnetic field had a relatively large impact on dose parameters in the multi-target and lung test cases compared with other test cases. However, there were no significant influences on the plan-quality metric, MU and dose accuracy for all test cases.
Keywords
Introduction
MR-guided radiation therapy (MRgRT) integrates a magnetic resonance (MR) scanner with a linear accelerator radiation therapy system, offering superior soft tissue contrast in MR images.1–4 However, the presence of a magnetic field inevitably affects radiation dose. Monte Carlo calculations on phantoms have shown that the magnetic field can cause asymmetric point spread kernels, leading to shifts and asymmetry in build-up and beam penumbra regions.5,6 This effect is particularly significant at tissue-air/tissue lung interfaces, resulting in dose changes known as the electron return effect due to secondary electrons being forced back into the tissue by Lorentz forces.7–9
Studies with existing MRgRT techniques for different sites have been reported.10–17 The American Association of Physicists in Medicine (AAPM) Task Group (TG) has published a guidance document and guidelines for intensity-modulated radiation therapy (IMRT) commissioning. 18 These guidelines include test cases to benchmark the overall accuracy of IMRT planning and delivery. Specifically, AAPM TG 11919,20 utilized simplified target structures with organs at risk (OARs) and planning goals using various delivery techniques, devices, and planning systems. In this study, in addition to the typical test cases derived from AAPM TG 119, two additional test cases were utilized. One is the circle target test case in the circle phantom to investigate the impact of shifts and asymmetry in build-up regions and beam penumbra regions of MRgRT. Another is the lung test case21,22 to investigate the influence of the electron return effect on dose.
Here, we present the comprehensive investigation into the impact of the magnetic field on treatment planning using typical phantom test cases. These test cases include a circle target test case, AAPM TG119 test cases (prostate, head-and-neck, C-shape, multi-target), and a lung test case. Our approach involved several steps: First, we contoured the planning target volumes (PTVs) and OARs for each test case. Subsequently, we generated two types of IMRT plans for each case: the original plan with the magnetic field (1.5 T plan) and a re-optimized plan without the magnetic field (0 T plan) under the same optimization conditions. To comprehensively evaluate treatment plan, we considered various dose parameters, including conformity index (CI), homogeneity index (HI), fit index (FI) and dose coverage of the PTV, the dose delivered to OARs, normal tissue (NT) defined as the volume inside the body and greater than 2 cm from the PTV, and monitor unit. We employed a plan-quality metric (PQM) scoring procedure. In addition, for the 1.5 T plans, dose verifications were performed using an MR-compatible ArcCHECK phantom.
Materials and Methods
Contouring of Typical Phantom Test Cases
The typical phantom test cases include circle target test case, prostate, head-and-neck, C-shape, multi-target and a lung test case. A detail description of all the structure sets is as follows:
Circle target structure set (Figure 1) consists of circle PTV. The circle PTV is a cylindrical structure of 6 cm radius, placed at the center of circle phantom. The prostate structure set consists of prostate GTV, prostate PTV, rectum and bladder.
19
One-third of rectum overlaps with prostate PTV. The head and neck structure set consists of head PTV, LT & RT parotids and spinal cord. There is 1.5 cm gap between spinal cord and PTV.
19
The C-shape structure set consists of C-shape PTV with 1.5 cm inner and 3.7 cm outer radius.
19
The OAR core is a cylindrical structure of 1 cm radius and with a gap of 0.5 cm between the C-shape PTV and the core. Multi-target structure set has three cylindrical structures of 4 cm diameter and 4 cm length stacked along the coronal axis.
19
The lung test case, displayed in Figure 2, references target published in previous literature.21,22 The lung structure set consists of lung PTV, lung L, lung R, Lung All, heart and cord. The lung PTV is a cylindrical structure of 2 cm radius. The cord is a cylindrical structure of a 0.5 cm radius with a 2.0 cm gap between lung PTV and the cord. There is a 1.0 cm gap between the heart and PTV. The density of Lung L/R was set to 0.25 g/cm3.
23

Circle target test structure set. The set comprises a circle PTV with 6 cm radius, centered within a circular phantom.
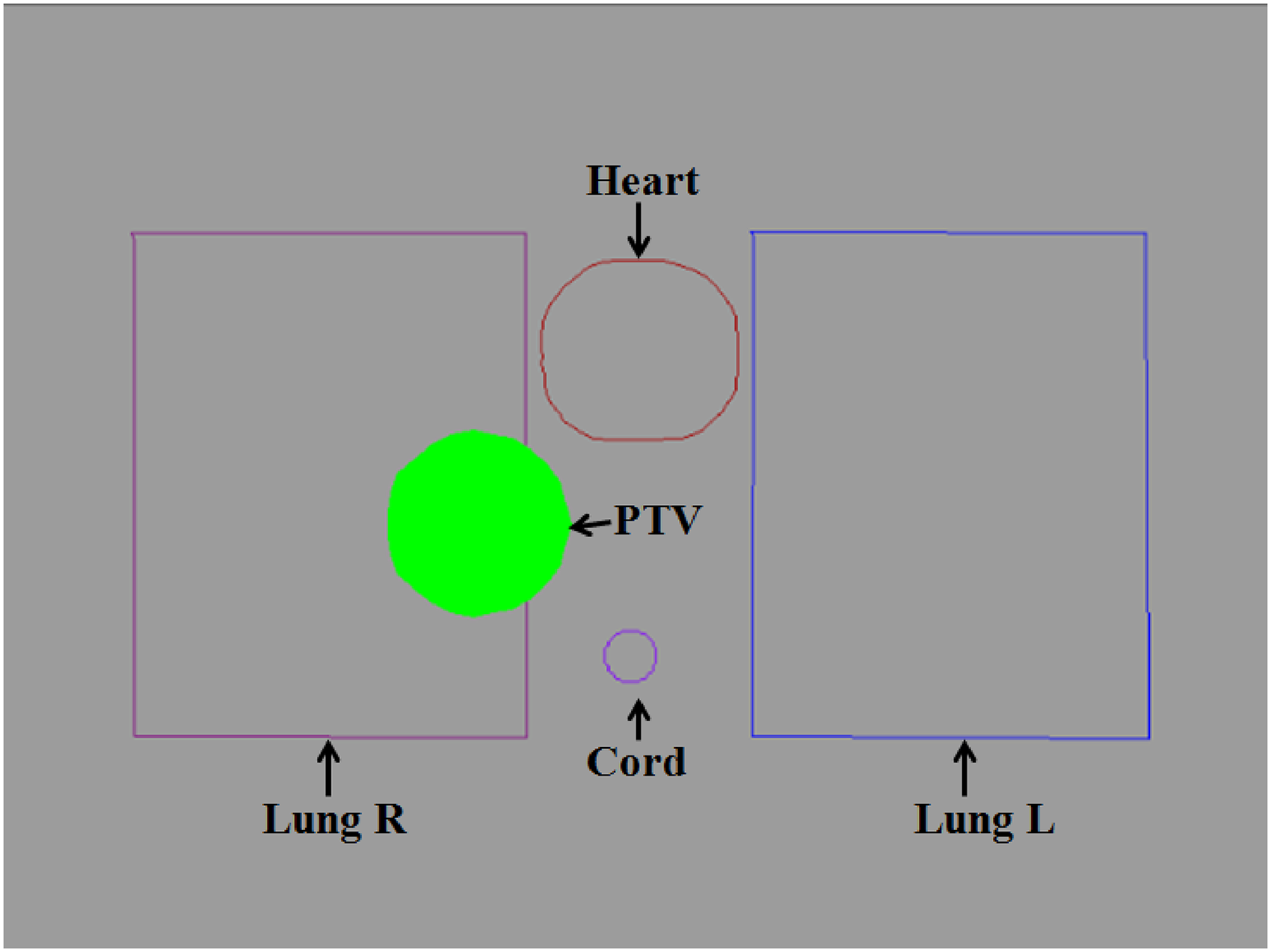
Lung test structure set. The set consists of PTV, lung L, lung R, heart and cord. The density of Lung L/R was set to 0.25 g/cm3.
The prescribed dose and dose requirements for the test cases are presented in the Supplemental material file of Table S1. All plans were designed to meet these requirements and adhere to the specified dose volume constraints. Specifically, for the prostate, head-and-neck, C-shape, and multi-target test cases, the prescriptions and dose volume constraints followed the guidelines outlined in AAPM TG119. 19
Design of IMRT Radiotherapy Plan
Treatment planning was performed using the Monaco (v5.40.01, Elekta AB, Stockholm, Sweden) treatment planning system. As described by Hissoiny S et al, 24 the Monaco treatment planning system (TPS) incorporates the GPU Monte Carlo dose algorithm, which can account for the presence of a 1.5 T magnetic field. The algorithm has shown good consistency with GEANT4 calculations at both 0 T and 1.5 T. 25 Due to the absence of the volumetric modulated arc therapy technique; the Unity MR-linac utilizes a step-and-shoot IMRT technique.
Taking into account the location of the PTV and their symmetric distribution, two IMRT plans were generated utilizing 7 to 9 fields while considering the presence of both 0 T and 1.5 T magnetic fields. To prevent high-dose delivery to the cable tube in the low-temperature thermostat, these plans were designed to avoid angles of 13 degrees. The plan parameters were configured as follows: the minimum segment area was set to 4 cm2, the minimum segment width was set to 0.5 cm, low fluence smoothing was applied, a minimum of 4 MU per segment was enforced, the maximum number of segments was set to 120, and the statistical uncertainty per calculation was set at 1%.
The 1.5 T plan was generated at 1.5 T using a set of optimization objectives. For the 0 T plan, we reset the calculation engine, removed fluence, segments, and dose. Additionally, we changed the beam type from “MRL1.5T” to “MRLNoMag” and optimized the plan using the same cost function as the 1.5 T plan. Both plans underwent optimization based on fully optimized fluence maps with a 3-mm grid resolution.
Evaluation of Radiotherapy Plan
To compare the two types of plans, we calculated the dose parameters and plan quality metrics of 1.5 T plan in comparison to 0 T plan.
Evaluation of Dose Parameters
The dose parameters of the targets included the following metrics: (i) D99, D50 and D1, indicating the irradiated dose received by 99%, 50% and 1% of the PTV, respectively. (ii)The homogeneity index (HI),
26
defined as: HI = (D2-D98)/D50

(iii) The conformity index (CI),27,28 defined as:

(iv) The cummulative fit index (cFI),
29
defined as:


Several parameters were compared for the OARs: (i) D30 and D10 of rectum and bladder; (ii) the maximum dose (Dmax) and D1cc to the spinal cord; (iii) D30 and the mean dose (Dmean) to the parotids; (iv) D50, D30, and D20 to lung all; (v) D30 and D40 to heart; (vi) D1 of the core; (vii) the mean dose to normal tissue (NT), defined as the volume inside the body and greater than 1.5 cm from the target volume.
Evaluation of Plan Quality Metrics
Based on the concept of plan-quality metric (PQM) proposed by Benjamin 30 and the plan-quality score (SD) proposed by Bohsung, 31 a PQM scoring procedure was defined for the test case plans. Each metric has a unique quantity and PQM value function used to calculate a point value, with corresponding PQM values ranging uniformly from 0 to 1. A description of each PQM metric is provided in the Supplemental material file of Table S2–7.
Phantom Measurements
Six 1.5 T plans were recalculated using the CT image of an MR-compatible ArcCHECK phantom (Sun Nuclear Corporation, Melbourne, USA) with Monte Carlo algorithm (GPUMCD). The ArcCHECK phantom was then mounted on the treatment couch using a holder to immobilize it. The data was collected and analyzed using SNC patient software (version 8.2, Sun Nuclear Corporation, Melbourne, USA).The gamma passing rate (ArcCHECK vsTPS) was used to identify discrepancies between TPS calculations and phantom measurements. As recommended by AAPM report TG218, 32 the criteria of 2 mm/3% and 2 mm/2% with global normalization and a threshold of 10% were implemented.
Statistical Analysis
Statistical significance of differences in the monitor units and plan quality metric was tested using the Wilcoxon signed rank test in SPSS v17 (IBM Corp.). Results with p < 0.05 were considered statistically significant.
Results
Dose Distribution and DVHs of 1.5 T and 0 T Plans
The dose distributions for six typical phantom test cases are shown in Figure 3. The axial plane dose distributions of 1.5 T and 0 T plans of circle target test case, prostate, head-and-neck, C-shape and a lung test case are displayed in Figure 3(a-h), and Figure 3(k-l). The coronal plane dose distributions of multi-target case are displayed in Figure 3(i) and Figure 3(j).

The dose distribution of the 1.5 T and 0 T IMRT plans for (a) and (b) circle target, (c) and (d) prostate, (e) and (f) head and neck, (g) and (h) C-shape, (i) and (j) multi-target, (k) and (l) lung test case.
Figure 4 shows the DVHs of PTV and OARs for the plans designed for the 1.5 T and 0 T magnetic fields for the circle target, prostate, head and neck, C-shape, multi-target, and lung test cases. In addition, NT is also displayed in the DVHs.
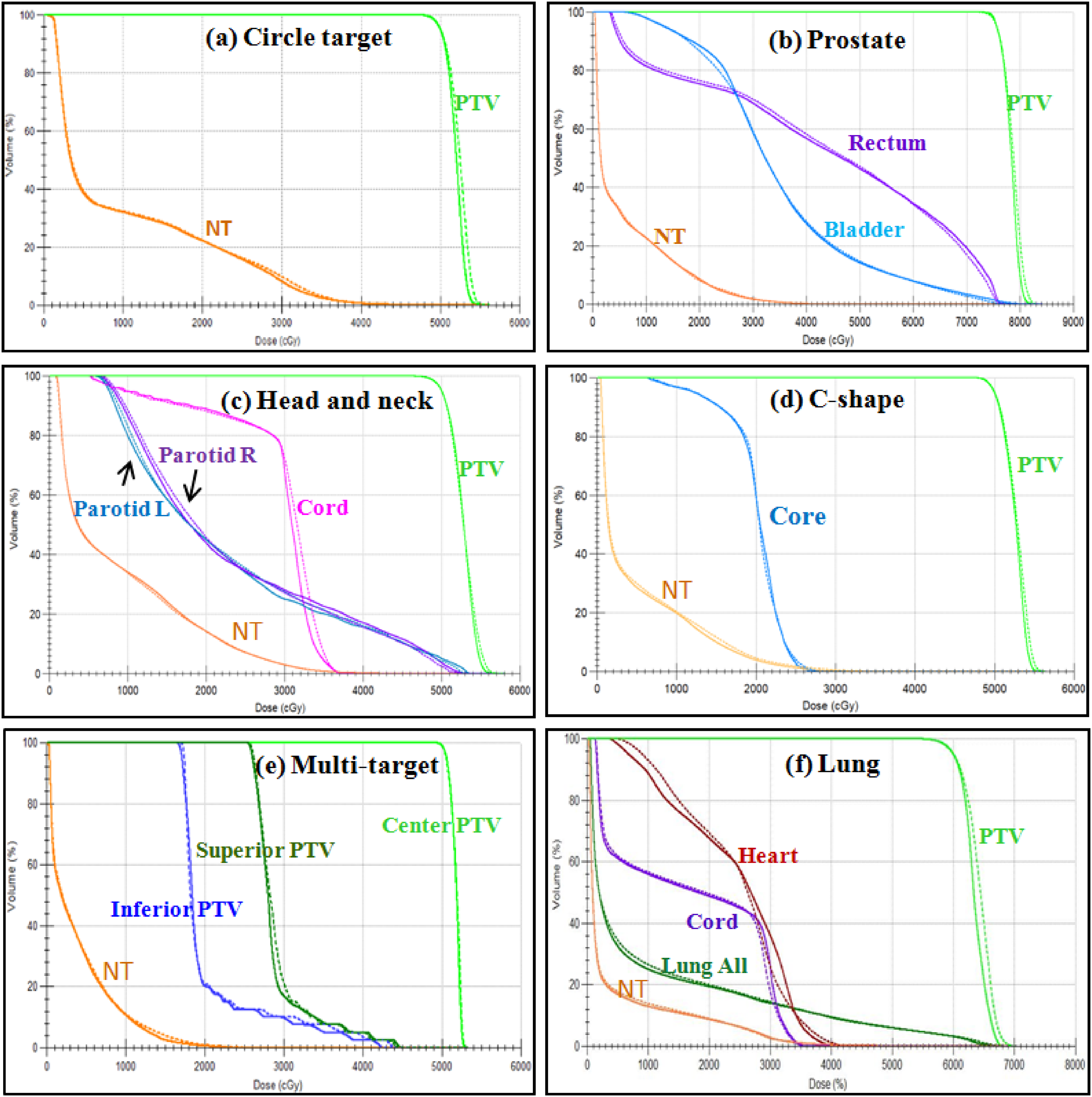
DVHs of PTV and OARs for the plans designed for the 1.5 T and the 0 T magnetic fields. (a) circle target, (b) prostate, (c) head and neck, (d) C-shape, (e) multi-target, and (f) lung test case. The dashed line represents the 1.5 T plan, and the solid line represents the 0 T plan.
Effect of 1.5 T Magnetic Field on Dose Parameters of PTV and OARs
The dose and dose differences in dose–volume metrics between the plans designed for 1.5 T and 0 T magnetic fields are presented in Tables 1–6.
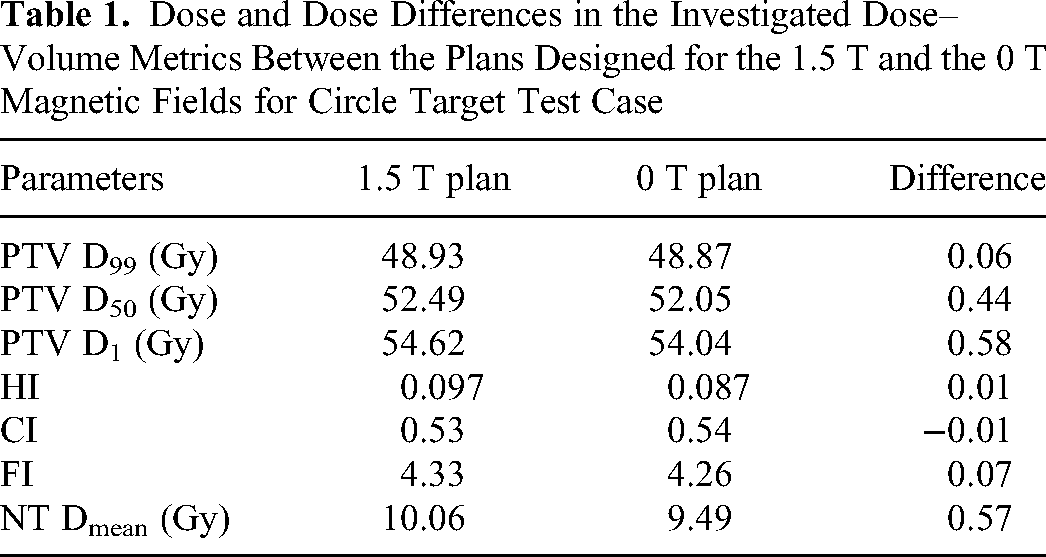
Dose and Dose Differences in the Investigated Dose–Volume Metrics Between the Plans Designed for the 1.5 T and the 0 T Magnetic Fields for Circle Target Test Case
Circle Target Test Case
Dose and dose differences in the investigated dose–volume metrics between the plans designed for the 1.5 T and the 0 T magnetic fields for circle target test case were displayed in Tabel 1. In the circle target test case, the dose differences of D99, D50, and D1 for the PTV between the two plans are smaller than 0.60 Gy. The most significant difference is observed in the D1 value of the PTV among D99, D50, and D1. The difference values of HI and CI are smaller than 0.1. The mean dose difference in NT between the two plans was less than 0.6 Gy, influenced by the magnetic field.
Prostate Test Case
Dose and dose differences in the investigated dose–volume metrics between the plans designed for the 1.5 T and the 0 T magnetic fields for prostate test case were displayed in Table 2. In the prostate test case, the dose differences of D99, D50 and D1 of PTV between two plans were smaller than 1 Gy. Small differences in metrics were found for the HI and CI. The influence of FI was relatively larger than that of HI and CI. The mean dose of rectum increases by 0.34 Gy, while the mean dose of bladder decrease by 0.18 Gy due to the magnetic field. The most significant relative influence was 0.96 Gy on the D10 of the rectum.
Dose and Dose Differences in the Investigated Dose–Volume Metrics Between the Plans Designed for the 1.5 T and the 0 T Magnetic Fields for Prostate Test Case

Head and Neck Test Case
Dose and dose differences in the investigated dose–volume metrics between the plans designed for the 1.5 T and the 0 T magnetic fields for head and neck test case were displayed in Table 3. In the head and neck test case, the most significant influence was on the D1 of the PTV compared to D99 and D50 of the PTV. The changes affected by the 1.5 T magnetic field in Dmax and D1cc for the cord in head and neck test case are less than 0.7 Gy. However, the dose change for parotid L and Parotid R is different. The mean dose of parotid L increases by 0.37 Gy, while the value for parotid R increases by 0.03 Gy. Small differences in metrics were found for the mean dose of NT.
Dose and Dose Differences in the Investigated Dose–Volume Metrics Between the Plans Designed for the 1.5 T and the 0 T Magnetic Fields for Head and Neck Test Case

C-Shape Test Case
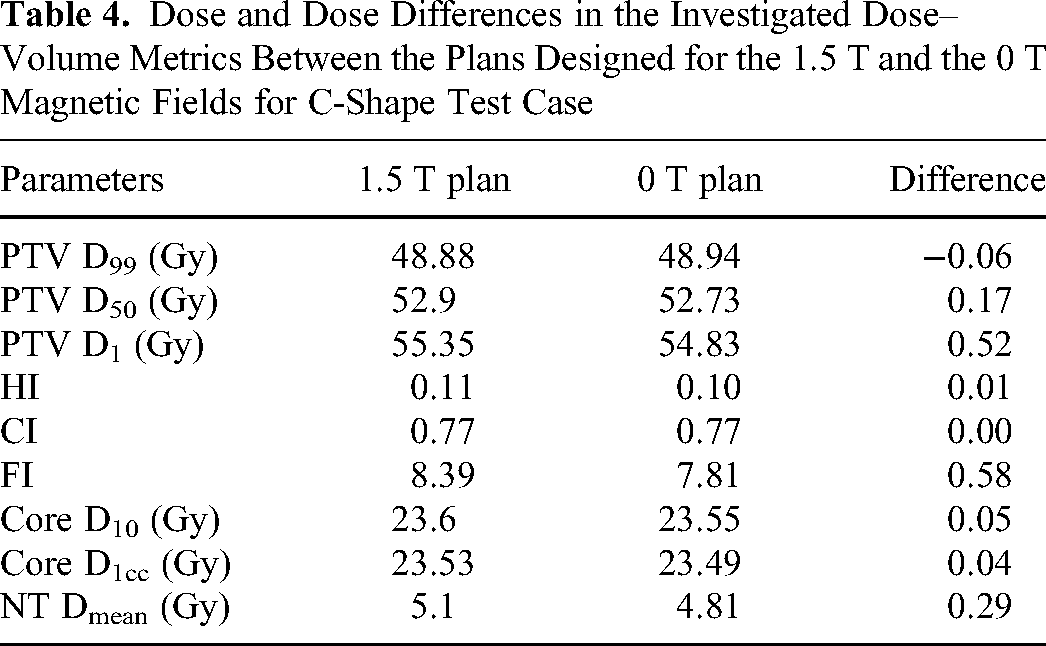
Dose and dose differences in the investigated dose–volume metrics between the plans designed for the 1.5 T and the 0 T magnetic fields for C-shape test case were displayed in Table. 4. In the C-shape test case, the most significant influence was also on the D1 of the PTV compared to D99 and D50 of the PTV. The influence of FI was relatively larger than that of HI and CI. Small differences in metrics were found for the D10 and D1cc of core. The mean dose difference in NT between the two plans was 0.29 Gy.
Dose and Dose Differences in the Investigated Dose–Volume Metrics Between the Plans Designed for the 1.5 T and the 0 T Magnetic Fields for C-Shape Test Case
Multi-Target Test Case
Dose and dose differences in the investigated dose–volume metrics between the plans designed for the 1.5 T and the 0 T magnetic fields for multi-target test case were displayed in Table 5. In the multi-target test case, there were three target volumes: center PTV, superior PTV and inferior PTV. It is evident from Table 5 that for the inferior PTV, superior PTV and center PTV, the dose differences in D1 of PTV were 1.45 Gy, −0.36 Gy and 0.03 Gy, respectively; the dose differences in D99 of PTV were 0.4 Gy, 0.16 Gy and 0 Gy, respectively; and the dose differences in D50 of PTV were −0.26 Gy, 0.25 Gy, and 0.06 Gy, respectively. Thus, the most significant dose influence was on the inferior PTV, followed by the superior PTV. For the superior PTV, the FI difference was 0.8. A small dose difference of 0.16 Gy in NT between the two plans was found.
Dose and Dose Differences in the Investigated Dose–Volume Metrics Between the Plans Designed for the 1.5 T and the 0 T Magnetic Fields for Multi-Target Test Case

Lung Test Case
Dose and dose differences in the investigated dose–volume metrics between the plans designed for the 1.5 T and the 0 T magnetic fields for lung test case were displayed in Table 6. There was a relatively large dose influence on the lung test case compared with other test cases. In the lung test case, the dose differences in D50 and D1 for PTV are 1.11 Gy and 1.20 Gy. The effect of the magnetic field on the doses of lung and heart is more significant than the core. The D30 and D20 of the lung increased by 1.03 Gy and 1.29 Gy, and the D30 and D40 of the heart decreased by 1.81 Gy and 1.1 Gy due to the magnetic field. However, a small influence was observed on the FI, HI, CI, and the mean dose of NT.
Dose and Dose Differences in the Investigated Dose–Volume Metrics Between the Plans Designed for the 1.5 T and the 0 T Magnetic Fields for Lung Test Case

Effect of 1.5 T Magnetic Field on Delivery Efficiency
To evaluate the efficiency of delivering radiation therapy in the presence of the magnetic field, the MUs for the two types of plans are statistics and shown in Table 7. No statistically significant difference was observed between the MUs for the 1.5 T plans and the 0 T plans.
The Comparison of MU Values Between 1.5 T and 0 T Plan

Effect of 1.5 T Magnetic Field on Plan Quality
Table 8 presents the plan quality metric of the two types of plans. The plan quality score reflects the overall quality of the treatment plans. With the exception of the multiple-target test case, the quality of the 1.5 T plan for various test cases showed a slight decrease in the presence of a 1.5 T magnetic field compared to the 0 T plan. However, no statistically significant difference in plan quality was observed between 1.5 T plan and 0 T plan.
The Comparison of Quality Metric Between 1.5 T and 0 T Plan

Dose Verification Results for the 1.5 T Plan
Figure 5 and Figure 6 display the results of dose verification for the dose distribution of the 1.5 T plan. With the 2 mm/3% criterion, the percentage of passing points ranged from 98.50% to 99.70% (Figure 5). With the 2 mm/2% criterion, the percentage of passing points ranged from 97.2% to 98.8% (Figure 6). For all the plans, gamma passing rates were higher than 95%. 32 These high passing rates indicate that the dose distribution is very consistent with the planned dose distribution within tighter tolerances.

Gamma passing rate of the 1.5 T plan with 2 mm/3% criteria measured using the ArcCHECK phantom.

Gamma passing rate of the 1.5 T plan with 2 mm/2% criteria measured using the ArcCHECK phantom.
Discussion
This study provides an investigation into the effect of 1.5 T magnetic fields on IMRT plans for six typical test cases. Study primarily encompasses two aspects: the influence of the 1.5 T magnetic fields on planning quality and delivery efficient. Two types of plans were formulated: an original plan designed for a 1.5 T magnetic field and a re-optimized plan without magnetic field.
Firstly, the study evaluates the disparities in dose parameters of PTV between the 1.5 T and the 0 T plans. The differences in D99 and D50 imply that the impact of the magnetic field on the PTV coverage is relatively modest. This is in line with the findings of Raaijmakers et al 10 and Christiansen RL et al. 11 The maximum observed variation in D1 within the multi-target radiotherapy plan across all test cases signifies that the proximity of multi-target volumes is notably affected by the presence of the magnetic field. Regarding the HI of the PTV, it was noted that, except for the superior PTV in the multi-target case, the HI values for the PTV in the 1.5 T plan were generally greater than those in the 0 T plan across all test cases. The differences indicate that the dose homogeneity in the 1.5 T plan was suboptimal compared to that in the 0 T plan.
Concerning the OARs, the dose differences for the rectum, bladder, parotids, and core in the 1.5 T plan closely resembled those in the 0 T plans, as illustrated in Tables 1–5. These findings align with recent studies,10,13 indicating clinical equivalence between MR-linac plans and plans from conventional linac systems. Notably, there were relatively large increases in D20 and D30 for the lung, suggesting a more pronounced influence of the magnetic field on these parameters. This agrees with previous research by Finazzi et al.15,16 Theoretically, changes induced by the magnetic field result from variations in dose deposition in tissues.6,12,33 In all test cases, there were no significant differences in the mean dose of NT between the 1.5 T and 0 T plans. This suggests that, compared to the 0 T plan, while doses increased in some beam directions in the 1.5 T plan, they decreased in others, and the magnetic field's influence on the mean dose of NT could be compensated by using multiple IMRT beams.
Table 7 displays a comparison of MU values between the 1.5 T plan and the 0 T plan. There were no significant differences between the two plans. The result indicates that the magnetic field does not impact the radiation therapy delivery. However, it's worth noting that the dose rate for the Unity MR-Linac is 425 MU/min, which is lower than that of a conventional linac, typically ranging from 600 to 1400 MU/min. As a result, the delivery time for MR-Linac is longer compared to conventional linacs. 34
The study assesses treatment plan quality under the influence of a 1.5-Tesla magnetic field using a quantitative scoring procedure that considers all metrics for targets and OARs. In most test cases, except for the multi-target scenario, the 1.5 T plan's quality slightly decreased compared to the 0 T plan. This provides the quantitative impacts on plan quality and the robustness of conventional IMRT plans in a magnetic field. It's worth noting that the subjective nature of defining scale and weights in the PQM components is a limitation, but PQM remains a crucial index for quantitatively evaluating treatment plan quality.30,31
The dose verification results for the 1.5 T plans, as displayed in Figures 5 and 6, highlight the high accuracy of dose distribution achieved in MR-guided radiotherapy. Although the presence of a 1.5 T magnetic field, dose verification results demonstrate that despite potential alterations, the treatment plans maintain a high degree of accuracy, dose distribution very consistent with the planned dose distribution within tighter tolerances.
Conclusions
In summary, the presence of a 1.5 T magnetic field had a relatively large impact on dose parameters in the lung and multiple test cases compared with other test cases. In the multi-target test case, the most significant influence was on the inferior PTV, followed by the superior PTV. In addition, study indicates that dose homogeneity in the 1.5 T plan was suboptimal compared to that in the 0 T plan. However, there were no significant influences on the PQM and MUs for all test cases. Although the presences of a 1.5 T magnetic field, dose verification results demonstrate that the treatment plans maintain high dose accuracy.
Supplemental Material
sj-doc-1-tct-10.1177_15330338241272038 - Supplemental material for Impact of 1.5 T Magnetic Field on Treatment Plan Quality in MR-Guided Radiotherapy: Typical Phantom Test Cases
Supplemental material, sj-doc-1-tct-10.1177_15330338241272038 for Impact of 1.5 T Magnetic Field on Treatment Plan Quality in MR-Guided Radiotherapy: Typical Phantom Test Cases by Lingling Yan, Yingjie Xu and Jianrong Dai in Technology in Cancer Research & Treatment
Footnotes
Abbreviations
Acknowledgments
This work was supported by the Guangzhou Shared Future Charitable Foundation “Dengfeng” research project of precision radiotherapy on cancer (2021-DF-002), and the National High Level Hospital Clinical Research Funding (2022-CICAMS-80102022203).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Statement
All procedures performed in this study only involved the phantom data, and there were no animal and human participants involved.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Guangzhou Shared Future Charitable Foundation "Dengfeng" research project of precision radiotherapy on cancer, National High Level Hospital Clinical Research Funding, (grant number 2021-DF-002, 2022-CICAMS-80102022203).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.