
Abstract
Objective
The purpose of this research was to compare two treatment techniques for oropharyngeal cancers: conventional linac-based static intensity-modulated radiotherapy (sIMRT) and helical tomotherapy (HT). The study examined several parameters, including target coverage, organs at risk, integral dose, and beam on time. Additionally, the study evaluated the doses to the parotid, temporomandibular joint, and pharyngeal constrictor muscles, which are important for swallowing.
Method
The present study retrospectively analyzed the data of 13 patients with oropharyngeal cancer who underwent radiotherapy between 2019 and 2021. The treatment plans for each patient were regenerated using both sIMRT and HT treatment planning systems with the sequential boost method. The techniques were evaluated and compared based on dose-volume histogram, homogeneity index, and conformity index parameters. The target coverage and organs at risk were statistically compared for two techniques. Additionally, the doses received by the healthy tissue volume were obtained for integral dose evaluation. The beam on time for each technique was assessed.
Results
When considering planning target volume evaluation, there was no difference in Dmeans between the two techniques and sIMRT demonstrated higher D2% values compared to the HT. The HT technique had better results for all organs at risk, such as the parotid, temporomandibular joint, and pharyngeal constrictor muscle. As for integral dose, it has been shown that the sIMRT technique provides better protection compared to HT. In addition, the beam on time was also longer with the HT technique.
Conclusion
Both techniques may provide optimal target coverage for patients with oropharyngeal cancer. HT conferred notable advantages, especially with regard to critical structures implicated in swallowing, such as the parotid, temporomandibular joint, and pharyngeal constrictor muscle, in comparison to sIMRT.
Keywords
Introduction
The oropharynx anatomically includes the base of the tongue, soft palate, tonsillar region, and posterior pharyngeal wall. It extends from the hard palate to the hyoid bone. 1 Head and neck cancers are widespread worldwide, and oropharyngeal cancer is a significant contributor to this. Recently, there has been an alarming increase in its incidence, especially among young people in many countries. This trend is particularly worrying because of the high prevalence of oropharyngeal cancer linked to Human Papillomavirus (HPV) infection. 2
Radiotherapy is essential in the management of oropharyngeal cancer, offering curative potential, organ preservation, and improved quality of life for patients. 3 Planning radiotherapy for the head and neck region is difficult due to the complex anatomy and numerous organs at risk. However, there have been continuous efforts to address these challenges using advanced radiotherapy applications and planning techniques. 4 Predicting optimal technology and treatment techniques relies heavily on patient characteristics, clinical requirements, available resources, and the expertise of the treatment team.
Static (step-and-shoot) intensity-modulated radiotherapy (sIMRT) and helical tomotherapy (HT) deliver precise radiation doses to tumors and minimize damage to healthy tissues. This fact has been demonstrated in head and neck cancer patients. 5 Previous studies have compared the dosimetry of different IMRT and HT planning techniques for oropharyngeal cancer.6,7 Nonetheless, the studies have not collectively examined essential structures pertinent to the process of swallowing, including the parotid, temporomandibular joint, and the pharyngeal constrictor muscle.
This study aimed to compare the effectiveness of sIMRT and HT techniques in treating oropharyngeal cancers, considering parameters such as target coverage, organs at risk, integral dose, and beam on time. In addition, the study comprehensively assessed the doses to the parotid, temporomandibular joint, and pharyngeal constrictor muscles, which are crucial for swallowing.
Materials and Methods
Thirteen patients with oropharyngeal cancer who received radiotherapy between 2019 and 2021 were included retrospectively. This retrospective study followed the relevant Equator guidelines. 8 All patient data were deidentified. These patients were staged in accordance with the eighth edition of the American Joint Committee on Cancer (AJCC) staging system. 9
Computed tomography (CT) simulations were performed with a slice thickness of 2.5 mm using a thermoplastic mask. The gross tumor volume (GTV) and clinical target volume (CTV) were delineated by using clinical information, magnetic resonance imaging, and positron emission tomography. CTV1 was created by applying a 5-10 mm margin to the primary tumor and 3-5 mm to the lymph nodes. CTV2 included high-risk areas and lymph node levels, and CTV3 included elective lymph nodes. All planning target volumes (PTVs) were created with a 3-mm margin. Organs at risk included the brainstem, spinal cord, mandible, temporomandibular joint, pharyngeal constrictor muscle, parotid, and cochlea.
For patients receiving definitive radiotherapy, three dose levels were used: 70 Gy/35 fractions to primary and nodal GTVs, 60 Gy/30 fractions to regions at high risk for microscopic disease, and 50-54 Gy/25-27 fractions to elective lymph node regions. For cases involving adjuvant radiotherapy, elective neck radiotherapy of 50-54 Gy/25-27 fractions was delivered, followed by boost doses to the tumor bed and involved lymph node regions up to a total dose of 60-66 Gy/30-33 fractions. A daily prescribed dose of 2 Gy was applied to each PTV.
A healthy tissue volume was created to evaluate the integral dose. To commence this procedure, a volume was generated by augmenting the dimensions of the PTV by 5 cm along all sides in CT axial sections. Subsequently, healthy tissue volume was acquired by subtracting the PTV with a margin of 0.3 cm from the obtained volume. The generation of healthy tissue volume for a representative patient is illustrated in Figure 1. For comparison of integral dose, the healthy tissue volumes that received at least 5 Gy, 10 Gy, 15 Gy, and 20 Gy were assessed.

The generation of healthy tissue volume in coronal (a) and sagittal (b) sections for a representative patient. (The blue color signifies the healthy tissue volume, while the red line represents the PTV.) PTV, planning target volume.
The treatment plans for each patient were regenerated using the sequential boost method using both sIMRT and HT treatment planning systems. sIMRT plans were generated for all patients using 6 MV photon energy beams of Elekta Synergy platform linear accelerator with 1-cm-wide, 80-leaf (Elekta, Stockholm, Sweden). HT plans were created for each patient utilizing 6 MV flattening filter-free photon energy beams delivered by the Tomotherapy HDA (Accuray, Madison, Wisconsin, USA). The goal of the treatment was to ensure that 95% of the radiation dose covered 95% of the PTV, while also ensuring that the maximum dose received by 1 cc volume did not exceed 107%. A summary of the dose limitations for normal tissues in the oropharyngeal cancer treatment plans is given in Table 1.
Dose Constraints for Organs at Risk.
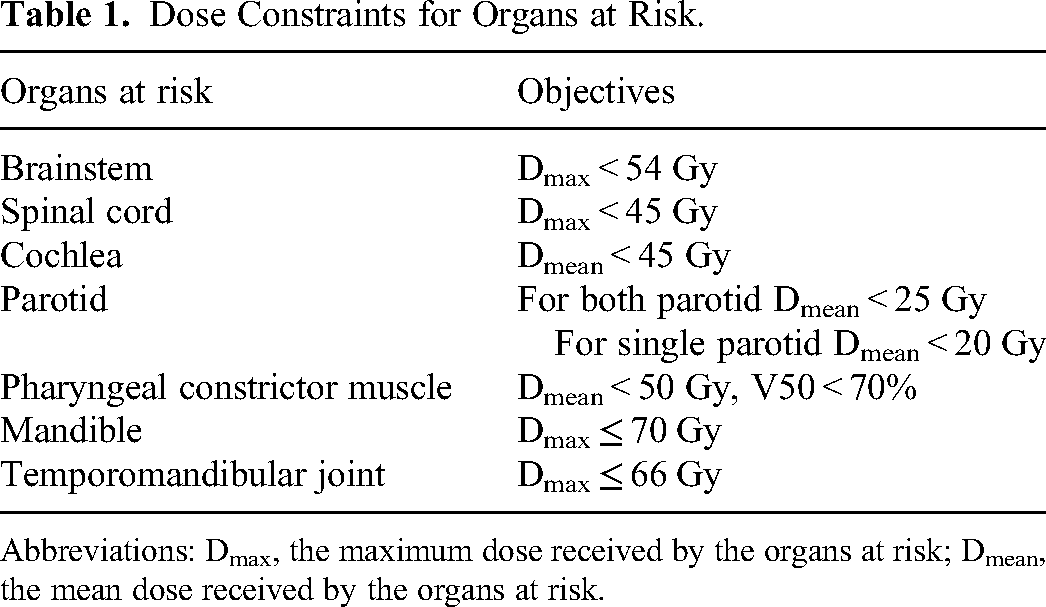
Abbreviations: Dmax, the maximum dose received by the organs at risk; Dmean, the mean dose received by the organs at risk.
The patients’ sIMRT inverse plans were created using a seven-field step-and-shoot technique (00, 500, 1000, 1500, 2100, 2600, 3100). The Monte Carlo algorithm of the MONACO TPS (version 5.1, Elekta, Stockholm, Sweden) was used to create the radiotherapy plans. For Tomotherapy plans, a 2.5 cm field width, pitch of 0.28, and nominal modulation factor of 2.5 were used. The Convolution/Superposition algorithm of the Tomotherapy HDA IDMS Precision Planning System (version 2.0.1.1; Accuray, Madison, Wisconsin, USA), which makes inverse planning, was used for dose calculation.
A cumulative dose-volume histogram was used to evaluate plan qualities of each patient. The assessment included doses received by 95% (D95%) and 2% (D2%) of the volume and the minimum, maximum, and mean doses of the PTV. Additionally, evaluations were made for the homogeneity index (HI) and conformity index (CI) for all plans.
ICRU 83 protocol was used for HI calculation.
10
D2, D98, and D50 represent the doses received by 2%, 98%, and 50% volumes of the PTV, respectively.

Statistical Analyses
Statistical analyses were conducted using IBM SPSS Statistics version 24.0 software (Armonk, NY: IBM Corp. 2016), and post hoc power analysis was performed with the G-power tool. 12
Descriptive statistics were performed to present the baseline characteristics. The Kolmogorov-Smirnov and Shapiro-Wilk tests were used to determine if the parameters followed a normal distribution. Non-parametrically distributed data were analyzed by the Wilcoxon matched-pair signed-rank test, whereas parametrically distributed data were assessed by the paired sample t-test. A P-value of less than 0.05 was accepted as statistically significant.
Post hoc power analysis showed that the sample size (N = 13) was adequate to detect the high effects (f = 0.87, P ≤ 0.05, power = 0.80).
Results
The study examined a total of 13 patients with oropharyngeal cancer, consisting of 10 males and 3 females. The median age was 59 years (range 33-80 years). The primary tumor sites were the base of the tongue in nine patients and the tonsil in four patients. Surgical treatment was conducted before radiotherapy in four of the 13 patients. Nine patients underwent definitive radiotherapy, while four received adjuvant radiotherapy. Histopathology of all patients was squamous cell carcinoma and HPV status was negative. Patient characteristics are summarized in Table 2.
Patient Characteristics.

Abbreviations: No, patient number; TNM, tumor-nodes-metastasis.
The comparison of dose, CI, and HI values for PTV1, PTV2, and PTV3 in HT and sIMRT treatment plans is summarized in Table 3. When evaluating PTV1, it was found that sIMRT had a higher D2% value, while HT had a higher D95% value (P = 0.01 for both). For PTV2 and PTV3, sIMRT had higher D2% and Dmax values (P = 0.005 and P = 0.04 for PTV2; P = 0.007 and P = 0.01 for PTV3, respectively). Furthermore, when all PTVs were evaluated regarding Dmean, no statistically significant difference was observed between HT and sIMRT. Although HT had better results in terms of CI for PTV1 (P = 0.005), no significant difference was observed for PTV2 and PTV3. Similarly, no difference was found between the two techniques regarding HI. PTV1% and 95% isodose distribution for sIMRT (a) and HT (b) for one sample patient is presented in Figure 2.
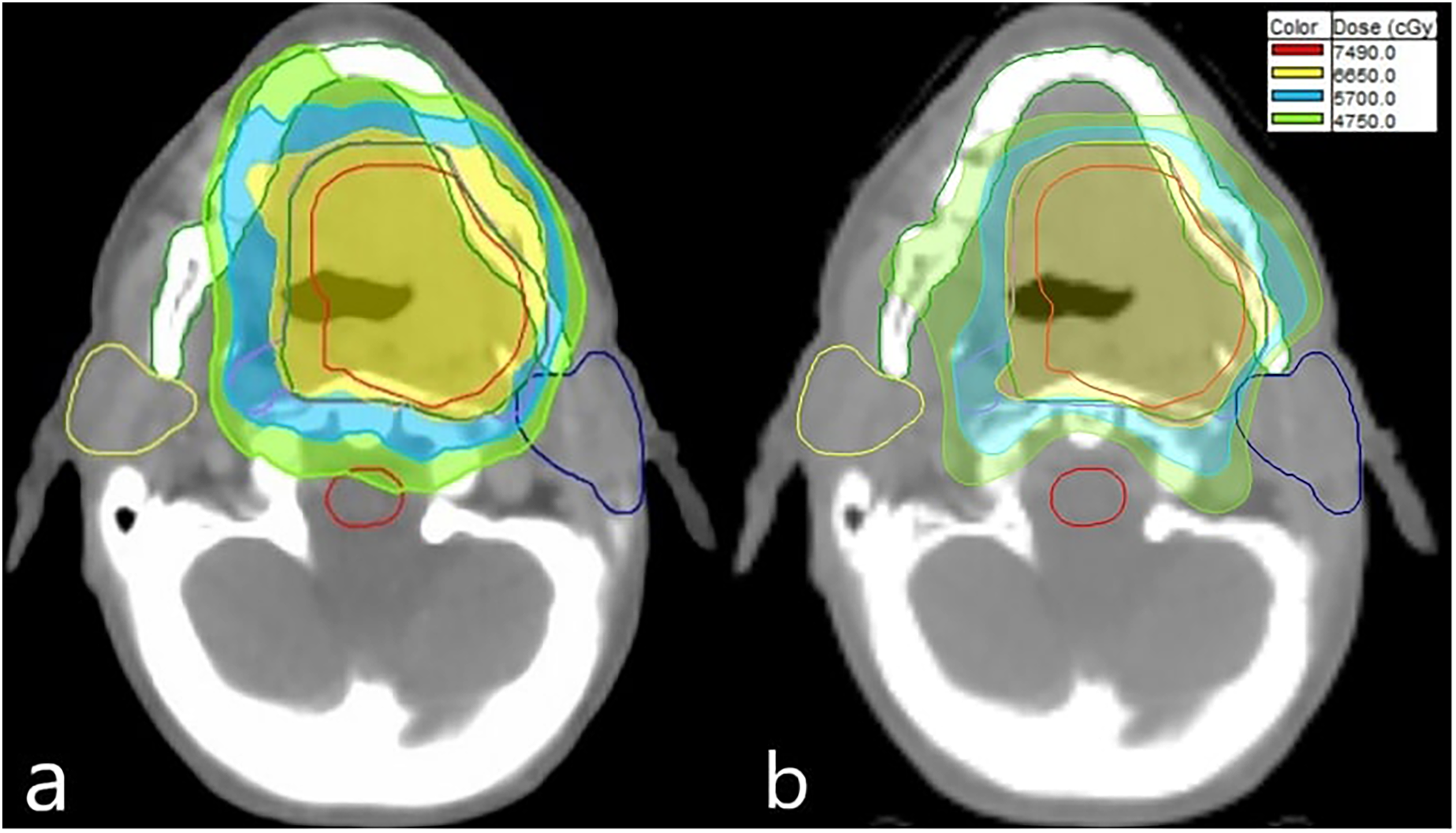
PTV1% and 95% isodose distribution for sIMRT (a) and helical tomotherapy (b) for a sample patient. (Yellow color signifies a dose of 66.5 Gy, light blue color indicates 57 Gy, and green color corresponds to 47.5 Gy.) sIMRT, static intensity-modulated radiotherapy; PTV, planning target volume.
Comparison of Dose, Conformity index (CI), and Homogeneity index (HI) Values of PTV1, PTV2, and PTV3 Obtained from HT and sIMRT Treatment Plans.

Abbreviations: SD, standard deviation; HT, helical tomotherapy; sIMRT, conventional linac-based static intensity-modulated radiotherapy; PTV, planning target volume; D2%, represent the doses received by 2% volumes of the PTV; D95%, represent the doses received by 95% volumes of the PTV; Dmin, represent the minimum dose received by the PTV; Dmax, represent the maximum dose received by the PTV; Dmean, represent the mean dose received by the PTV; PTV, planning target volume; CI, conformity index; HI, homogeneity index.
The doses received by organs at risk and integral dose are compared between HT and sIMRT in Table 4. All plans adhered to limiting the maximum dose to the temporomandibular joint to 66 Gy and the mandible to 70 Gy. However, HT allowed for greater sparing of the temporomandibular joint in terms of Dmax (P = 0.013 for the right and P = 0.009 for the left). It resulted in a reduction of the maximum dose by approximately 5 Gy compared to sIMRT in HT. Moreover, a significant difference was observed in terms of the maximum dose to the mandible between HT and sIMRT techniques (P = 0.007), with a reduction of approximately 3 Gy in HT compared to sIMRT.
Comparison of Organs at Risk and Integral Dose for HT and sIMRT Techniques.

Abbreviations: HT, helical tomotherapy; sIMRT, conventional linac-based static intensity-modulated radiotherapy; Dmax, the maximum dose received by the organs at risk; Dmean, the mean dose received by the organs at risk; TMJ, temporomandibular joint; PCM, pharyngeal constrictor muscle.
All plans adhered to limiting the mean dose to the pharyngeal constrictor muscle to 50 Gy and the parotids to 25 Gy. There was also a significant difference in the pharyngeal constrictor muscle (P = 0.014), with a reduction of approximately 7 Gy in the mean dose in HT compared to sIMRT. Furthermore, HT was superior to sIMRT regarding mean doses for both the right and left parotids (P = 0.001 for both parotids) with a reduction of about 5-7 Gy.
After comparing the HT plan with the sIMRT plan, it was found that the HT plan resulted in a lower Dmax for the brainstem and spinal cord and a lower Dmean for the cochlea. The difference between the techniques was statistically significant for the brainstem, spinal cord, and cochlea (P = 0.001 for the brainstem, P < 0.001 for the spinal cord, P = 0.001 for right the cochlea, and P = 0.02 for the left cochlea). However, the sIMRT plans had lower V5, V10, V15, and V20 values for healthy tissue volume than HT (P < 0.001 for V5, V10, and V15 and P = 0.005 for V20). Moreover, the mean beam on times for HT and sIMRT were 11.02 ± 2.96 min and 5.38 ± 0.94 min, respectively (P < 0.001).
Discussion
While optimal results regarding target coverage were obtained with both techniques, it has been shown that organs at risk can be better protected with the HT technique. In addition, the hot spots in the PTV were observed less in the HT plans. Although many studies have compared HT and sIMRT for head and neck cancer,13,14 the comparison between HT and sIMRT for oropharyngeal cancer is less well documented.6,7 According to Sheng et al, HT is more effective in providing dose homogeneity, with fewer hot spots and lower critical organ doses than sIMRT. Although this study evaluated organs at risk such as the brainstem, larynx, parotid, spinal cord, and oral cavity, the temporomandibular joint and pharyngeal constrictor muscle were not analyzed. 6 In a study by Clemente et al, three techniques were analyzed to treat oropharyngeal cancer: volumetric-modulated arc therapy (VMAT), sIMRT, and HT. The study found that HT plans had superior target coverage, conformity, and homogeneity. All treatment modalities were successful in sparing organs at risk. However, there was no significant difference between the modalities regarding the pharyngeal constrictor muscle, and the temporomandibular joint was not evaluated. 7
The parotid, temporomandibular joint and pharyngeal constrictor muscles are crucial for chewing, swallowing, and speaking. However, exposure to radiation during cancer treatment can cause complications such as muscle dysfunction, pain, osteoradionecrosis, trismus, and dysphagia.15,16 To prevent complications, limiting the dose applied to critical anatomical structures is essential. In our research, we collectively examined the parotid, temporomandibular joint, and pharyngeal constrictor muscle doses, and we observed a statistically significant difference between the two techniques concerning these crucial anatomical structures. We found that the HT plans were more effective, showing a decrease of around 5 Gy in the maximum dose for the temporomandibular joint and approximately 5-7 Gy in the mean dose for the parotid and pharyngeal constrictor muscle, compared to sIMRT. Therefore, HT is recommended as a better treatment option when adhering to the critical organ dose limits for these significant anatomical structures is challenging.
In radiotherapy, the integral dose is a crucial measure of the energy absorbed by the patient's body during treatment. Diallo et al found that 12% of secondary malignancies detected after radiotherapy were within the treatment field, while 66% were within a 5 cm radius around the field edge. Furthermore, 22% of the secondary malignancies occurred in regions beyond 5 cm from the irradiated volume. 17 It is important to reduce the integral doses to prevent harm to healthy tissues and the risk of secondary malignancies. Shi et al compared sIMRT and HT plans, focusing on the homogeneity of the PTV and the doses to healthy tissue volumes. According to the study, the HT plans for craniospinal radiotherapy and sIMRT plans for head and neck cancer showed better results. It was also reported that the sIMRT plan provided better protection for healthy tissue volumes. 18 Similarly, doses to organs at risk were found to be lower in HT, while integral dose was demonstrated to be lower in sIMRT, in our study.
When choosing a radiotherapy technique for patients with oropharyngeal cancer, it is crucial to consider the length of treatment. Shorter treatment times can improve patient comfort, reduce the chance of movements during treatment, and may provide biological benefits. 19 Studies have shown that the duration of treatment affects the efficiency of killing tumor cells.20–22 Longer beam on times for fractions in nasopharyngeal carcinoma cell culture result in reduced cell kill. 22 Although the exact processes behind this occurrence are not yet completely comprehended, scientists have suggested that repairing sublethal damage while irradiating may reduce cell kill. In a study conducted by Clemente et al, it was found that sIMRT had longer delivery times when compared to VMAT and HT in cases of oropharyngeal cancer. 7 However, the investigation did not identify any statistically significant difference in beam on times between VMAT and HT. In contrast, our study found that HT presents longer beam on times compared to sIMRT. The use of sIMRT shortened the beam on time compared with HT by an average of 51%. HT's longer treatment delivery time can be attributed to its helical delivery technique and multiple beam deliveries. In addition, HT requires extensive optimization to achieve adequate tumor coverage while sparing organs at risk effectively. This complexity in treatment planning contributes to the prolonged delivery times. As treatment delivery times increase in HT, workload increases and the number of patients receiving daily treatment decreases. It should be noted that this may lead to a possible increase in healthcare expenditures.
Our study has several limitations. First, the small sample size limits statistical power and larger prospective studies are needed to validate these findings. Clinical outcomes such as therapeutic response, toxicity, and survival should also be evaluated in these prospective studies. Another limitation of this study is that the MLC width in sIMRT treatment with Electa Synergy was selected as 1 cm. Better results in terms of organs at risk may be achieved with sIMRT treatments with smaller MLC widths. Therefore, MLC widths should also be considered in these dosimetric studies.
Conclusion
The treatment plans utilizing HT and sIMRT have demonstrated favorable results concerning target coverage in patients with oropharyngeal cancer. Compared to sIMRT plans, HT plans offered notable advantages in sparing organs at risk, including the parotid, temporomandibular joint, and pharyngeal constrictor muscle. Reducing the dose of organs at risk with HT may provide a crucial additional benefit in terms of mitigating possible side effects like dysphagia and improving quality of life. Further prospective studies with larger sample sizes are required to confirm these findings.
Footnotes
Abbreviations
Data Availability Statement for this Work
Research data are stored in an institutional repository and will be shared upon request to the corresponding author.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This study received approval from the Akdeniz University Faculty of Medicine Clinical Research Ethics Committee (Approval No: 59, Date: 27.01.2021). Ethics approval was obtained, but patient consent was not required. The necessity for obtaining informed consent from individual patients was waived by the ethics committee. This waiver was granted because it is an ethics committee-approved retrospective study, all patient information was deidentified, and patient consent was not required.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.