
Abstract
Objectives
The restoration of as much normal function as possible has become an important goal following the endoprosthetic reconstruction. The objective of this study was to assess the functional outcome after endoprosthetic reconstruction for tumors around the knee and to explore prognostic factors of functional outcome.
Methods
We retrospectively collected data on patients who underwent tumor prosthetic replacements consecutively. Musculoskeletal Tumour Society score and Toronto Extremity Salvage Score were used to assess the functional outcome at 1, 3, 6, 12, and 24 months after surgery. The logistic model was used to select factors that had potential predictive value for postoperative function. Potential prognostic factors included age, gender, tumor site, type of tumor, length of bone resection, type of prosthesis, length of prosthetic stem, chemotherapy, pathological fracture, and body mass index.
Results
At the 24 months after surgery, the mean musculoskeletal tumor society (MSTS) score was 81.4% and the mean Toronto extremity salvage score (TESS) was 83.6%. At the last follow-up, 68% of patients and 73% of patients received perfect or good MSTS score and TESS score, respectively. The multivariate analysis according to ordered-logit model showed that age < 35 years, distal femoral prosthesis, and length of bone resection < 14 cm were independent prognostic factors of better functional outcome.
Conclusions
Endoprosthetic reconstruction may provide good functional results for most patients. Younger patients with distal femoral prosthesis and shorter resection of bone (on the premise of complete resection of tumor) are more likely to obtain satisfactory functional results after surgery.
Introduction
The knee joint is a common site of bone tumors.1–3 Over the past few decades, limb salvage surgery has become a standard procedure for malignant bone tumors around the knee, and tumor prostheses are most commonly selected for the reconstructions of mega bone defects. In general, endoprosthetic reconstruction is a good option for the reconstruction of bone defects; however, it also leads to some medium- to longer-term impairment in the physical, psychological and social sphere. With advances in the treatment of cancer patients and increased survival time, restoration of as much normal function as possible is becoming an important goal. To verify possible prognostic factors of functional outcomes after endoprosthetic reconstruction is crucial for achieving favorable postoperative function.
Some studies have assessed functional outcome, prosthetic survival rate and complications after endoprosthetic reconstruction; however, studies on prognostic factors of functional outcomes are rare.4–6 Skaliczki et al. 7 evaluated the functional outcome in 23 patients who received endoprosthetic reconstruction following resection of malignant tumors around the knee. They correlated functional outcomes with the type of resection, length of resection, type of prosthesis, and tumor site, revealing that the only factor with a conspicuous impact on functional outcome was tumor site. However, only univariate analysis was performed in this study, and the sample size was very small. Tunn et al. 4 analyzed the functional outcome of 87 patients who underwent endoprosthetic reconstruction around the knee using musculoskeletal tumor society (MSTS) and Toronto extremity salvage score (TESS) scores. They found that the effect of age on postoperative function was significant and precise, whether it was assessed using TESS or MSTS score.
The purposes of this study were to assess functional outcomes of patients treated with tumor prostheses and to identify possible prognostic factors of functional outcome.
Patients and Methods
The current study was designed as a retrospective cohort study, and reported according to the strengthening the reporting of observational studies in epidemiology guideline. 8
Patients
The clinical data of 235 consecutive patients who underwent endoprosthetic reconstruction for tumors around the knee between May 2000 and December 2016 were retrospectively collected from two clinical centers (Tianjin Hospital & Jinan Military General Hospital). The inclusion criteria were endoprostheses used to reconstruct mega bone defects following tumor resection. The exclusion criteria were patients with incomplete medical records or patients without two years of follow up. This study was performed in accordance with the “Declaration of Helsinki” and was approved by the ethics committees of Tianjin Hospital (Tianjin City, China; approval number: (2021) Medical Ethics Review No. 231; approval date: December 22nd, 2021) and Jinan Military General Hospital (Jinan City, Shandong Province, China; approval number: (2018) Research Ethics Review No. 26; approval date: August eighth, 2018). Informed consent was obtained from the patients verbally, at the time of telephone follow-up on information about postoperative functional assessment. We have de-identified all patient details such that the identity of any person may not be ascertained in any way.
Twenty-four patients were excluded due to incomplete medical records and twenty-eight patients were excluded due to insufficient follow-up duration, leaving 183 patients for evaluation. There were 103 male patients (56.3%) and 80 female patients (43.7%), and the mean age at the time of surgery was 35 years (13–77 years). One hundred fourteen and 69 implants were placed in the distal femur and proximal tibia, respectively. All patients were staged according to Enneking's system. The histological diagnosis was osteosarcoma in 86 patients, giant cell tumor in 62 patients, malignant fibrous histiocytoma in 14 patients, chondrosarcoma in 9 patients, and other sarcoma in 12 patients. Disease-specific systemic chemotherapy and radiation therapy were administered according to the diagnosis. Chemotherapy was administered in 67 patients (36.6%), and radiotherapy was administered in 34 patients (18.6%). Table 1 displays the baseline characteristics of patients.
Baseline Characteristics of the Patients.

Reconstruction and Rehabilitation
Two chief physicians who are familiar with the related operations of tumor prosthesis replacement surgery completed all the operations. Determination of the osteotomy plane primarily depends on the position where the normal bone marrow signal on T1WI becomes an abnormal signal. Two kinds of tumor prostheses (Lidakang, Beijing, China and Wego, Beijing, China) were used for the reconstructions. One hundred prostheses were custom and 83 prostheses were modular. In all cases, stems were cemented and patellas were not replaced. The affected limb was raised and maintained at blockage negative pressure for 3 days, and intravenous antibiotics were used to prevent infection during this period. A folded towel was placed under the heel to achieve full knee extension after surgery. Standing and walking began within 4 days following surgery using crutches. A continuous passive motion apparatus was used 2 h per day and was continued until discharge. Ninety degrees of flexion was the goal at the time of discharge from hospital, and all patients received rehabilitation for at least one month.
Outcome Measures
Routine checks after surgery were performed at 1, 3, 6, and 12 months, and annually thereafter. For the investigation, patients were interviewed and examined in the outpatient department or were contacted by telephone. Among them, 170 patients underwent outpatient examinations and telephone follow-ups, while the rest only underwent telephone surveys. The prosthetic survival, defined as the time interval between the primary reconstruction operation and prosthesis failure or the final follow-up, was recorded. The MSTS and TESS scores were used to assess the functional outcome after endoprosthetic reconstruction to provide a better measure reflecting the complex situation of each patient. MSTS score 9 was calculated based on a standardized physical examination by the physician, and TESS 10 was completed by the patients to record the patients’ self-assessment. The MSTS scoring system includes six parameters: pain, functional capacity, emotional acceptance, need for walking aids, walking distance, and gait. Each parameter is scored between 0 and 5 according to specific criteria, and the maximum possible points is 30. The TESS questionnaire consists of 30 questions regarding patients’ disability, such as dressing, housework, mobility, and leisure. Each aspect is assigned a score from 1 to 5 with the total score of 150. The results of MSTS and TESS scores were calculated as percentages by dividing by the highest score and were classified as perfect (90%-100%), good (80%-89%), fair (70%–79%), or poor (0%–69%). The 24-month MSTS and TESS scores were regarded as the primary outcomes of this study. Additionally, in order to reflect more details concerning walking, we chose four questions from the MSTS and TESS at 24 months as the secondary outcomes: knee pain (yes vs no), walking distance (≥1 km vs < 1 km), need for walking aids (yes vs no), and walking upstairs (≥20 steps vs < 20 steps).
Data obtained from the medical records and subsequent follow-up included age (<35 years vs ≥ 35 years), gender (male vs female), tumor site (distal femur vs proximal tibia), type of tumor (benign vs malignant), length of bone resection (<14 cm vs ≥ 14 cm), type of prosthesis (custom vs modular), length of prosthetic stem (<14 cm vs ≥ 14 cm), chemotherapy (yes vs no), pathological fracture (yes vs no), and body mass index (<25 kg/m2 vs ≥ 25 kg/m2). These previously described factors were included as potential prognostic factors of functional outcome in this study.
Statistical Analysis
Mann-Whitney test and Kruskal–Wallis test were used to perform analyses on subgroups of MSTS and TESS scores. Logistic regression model was used to assess the predictive value of the recorded factors on functional outcome measured 24 months after surgery. Univariate analysis was carried out, and variables that were significant at the P ≤ .15 level were included in the multivariate analysis. Pearson Chi-square test was used to evaluate the statistical association between walking and three factors (age, tumor site, and length of bone resection). Kaplan-Meier analysis was used to calculate the prosthetic survival rate and prostheses were censored for death and problem-free at the last follow-up. P < .05 was considered statistically significant. Statistical analyses were performed using SPSS 22.0 software (SPSS Inc., Chicago, Illinois, USA) and GraphPad Prism 7 Software (GraphPad Software, Inc., SanDiego, CA).
Results
Baseline Characteristics
The mean duration of follow-up in this study was 93 months (range, 24-213 months). At the last follow up, among the 183 patients with bone tumors around the knee, 127 were continuously disease-free, 22 were disease-free after treatment of local recurrence, 11 were alive with tumor, and 23 had died of disease. The 5-year prosthetic survival rate was 92.2% (Figure 1). Thirty-five patients (19.1%) underwent revision surgery due to various complications, including 20 cases of aseptic loosening, six cases of deep infection, five cases of tumor progression, three cases of periprosthetic fracture, and one case of soft tissue problems. The mean overall time from surgery to complication was 79 months (range, 24–160 months).
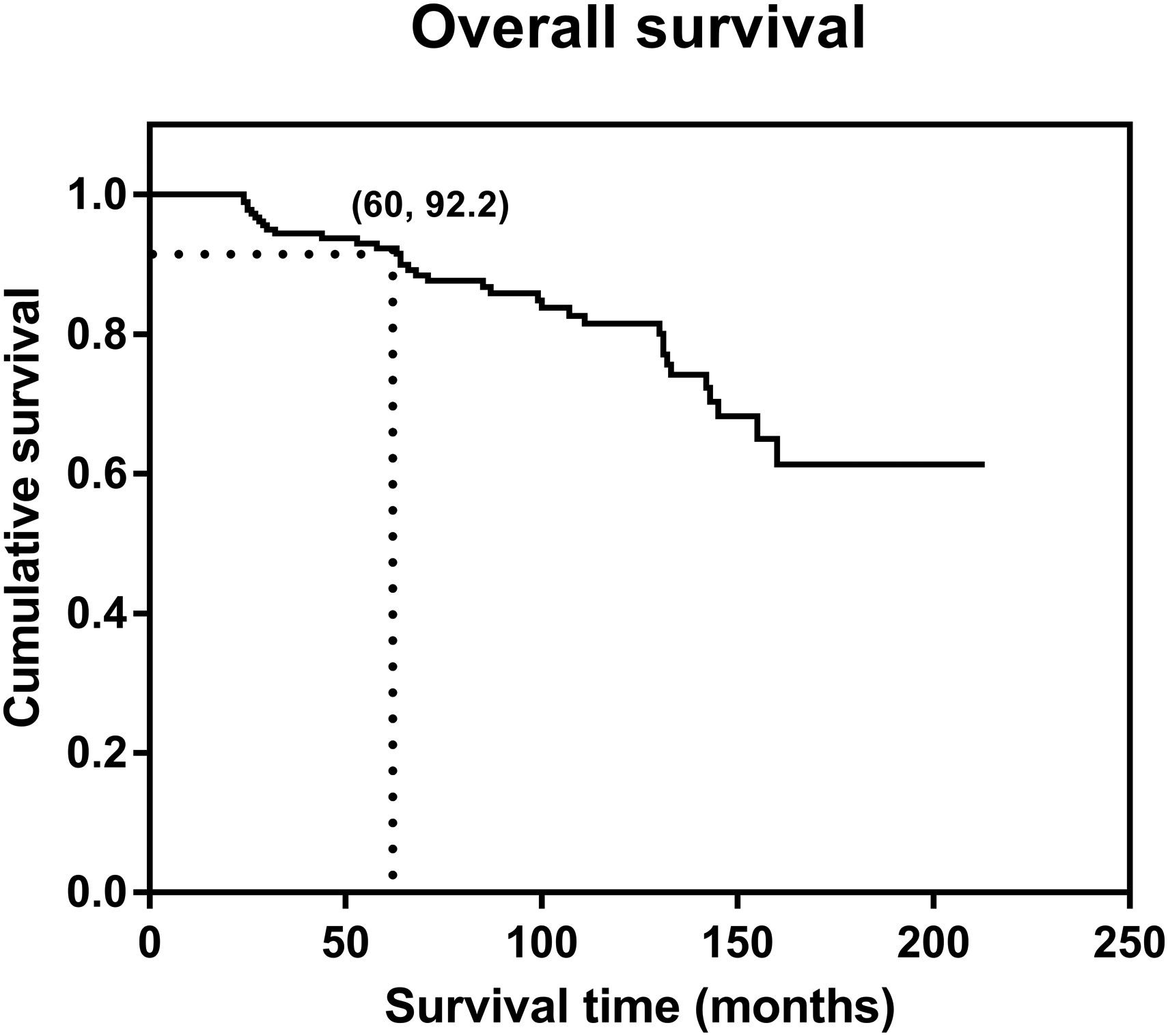
The Kaplan–Meier survival curve for the whole cohort. The 5-year prosthetic survival rate was 92.2%.
Functional Outcomes
At 1, 3, 6, 12 and 24 months after surgery, it was possible to evaluate 144, 141, 134, 132 and 125 patients for MSTS score and 152, 149, 142, 139 and 133 patients for TESS score, respectively (Table 2). Significant differences were observed among the functional results 1, 3, 6 and 12 months after surgery (P < .001 for MSTS and P < .001 for TESS). However, there was no significant difference between the functional results at 12 months and 24 months after surgery with respect to these measures (P = .383 for MSTS score and P = .245 for TESS) (Figure 2). It can be seen from the line chart that the postoperative function in patients with prosthetic replacements was significantly improved during the first year after surgery, but this trend disappeared in the second year, indicating that postoperative function did not be further improve in the second year.

Line chart of MSTS score and TESS related to the time after surgery. The scores of functional result gradually increased after surgery. Significant differences were found among the functional results at 1, 3, 6 and 12 months after surgery (P < .001 for MSTS score and P < .001 for TESS). However, there was no significant difference between the functional results at 12 and 24 months after surgery (P = .383 for MSTS score and P = .245 for TESS).
Mean Functional Score Related to Follow-up Time

Twenty-four months after surgery, the results for MSTS and TESS were 81.4% (60%–100%) and 83.6% (55%–100%), respectively. Results of MSTS score were perfect (90%–100%) in 37.6%, good (80%–89%) in 30.4%, fair (70%–79%) in 18.4% and poor (0%–69%) in 13.6% of patients. Results of TESS were perfect (90%–100%) in 40.6%, good (80%–89%) in 32.4%, fair (70%–79%) in 18.0% and poor (0%–69%) in 9.0% of patients.
Univariable and Multi-Variable Ordered-Logistic Analyses for Knee Functional Outcomes
The univariate analysis according to ordered-logit model showed that age (OR = 0.14, CI 95% 0.06∼0.29, P < .001), tumor site (OR = 0.55, CI 95% 0.28∼1.08, P = .083), length of bone resection (OR = 0.52, CI 95% 0.27∼1.00, P = .049), length of prosthetic stem (OR = 0.47, CI 95% 0.24∼4.24, P = .94), chemotherapy (OR = 3.15, CI 95% 1.55∼6.39, P = .001) and BMI (OR = 0.25, CI 95% 0.13∼0.50, P < .001) were all correlated with MSTS score (Table 3). The factors correlated with TESS were age (OR = 0.19, CI 95% 0.09∼0.39, P < .001), tumor site (OR = 0.52, CI 95% 0.27∼1.00, P = .048), length of bone resection (OR = 0.40, CI 95% 0.20∼0.77, P = .006), chemotherapy (OR = 2.07, CI 95% 1.07∼4.03, P = .031) and BMI (OR = 0.26, CI 95% 0.13∼0.51, P < .001) (Table 3).
Logistic Model Analyses of the Factors on Functional Outcome.

NI: not included; a: univariate analysis; b: multivariate analysis
The multivariate analysis according to ordered-logit model showed that age (OR = 0.12, CI 95% 0.04∼0.34, P < .001), tumor site (OR = 0.40, CI 95% 0.17∼0.96, P = .04) and length of bone resection (OR = 0.31, CI 95% 0.14∼0.70, P = .005) were independent prognostic factors for MSTS score (Table 3). The multivariable model demonstrated that age (OR = 0.15, CI 95% 0.06∼0.40, P < .001), tumor site (OR = 0.33, CI 95% 0.16∼0.67, P = .002) and length of bone resection (OR = 0.26, CI 95% 0.12∼0.56, P = .001) were independent prognostic factors for TESS (Table 3). Age < 35 years, distal femoral prosthesis, and length of bone resection < 14 cm were all significant prognostic factors of better functional outcome.
Effect of Age, Tumor Site and Length of Bone Resection on Walking Situation
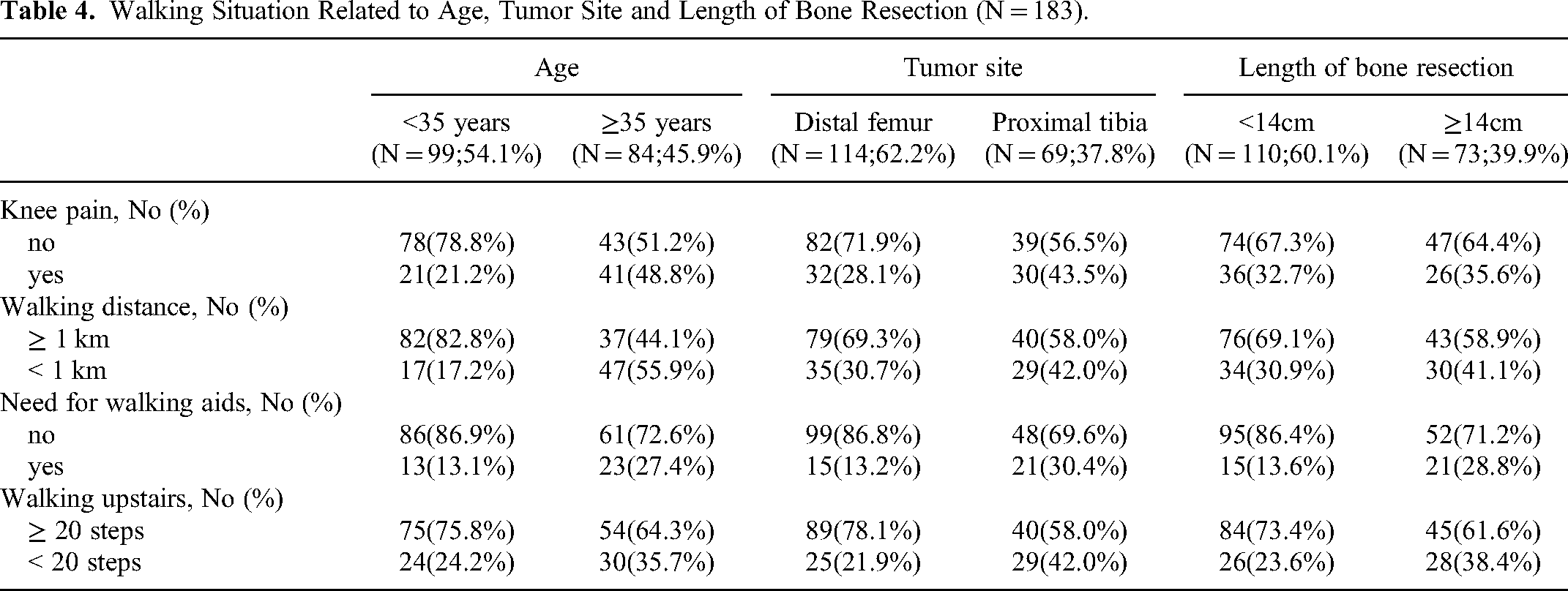
To explore whether these independent prognostic factors directly affect walking function of patients, we conducted an additional analysis. Age-specific differences were identified in three factors: knee pain, walking distance, and need for walking aids (P < .05)(Figure 3). Site-specific differences were found in three factors: knee pain, need for walking aids, and walking upstairs (P < .05). When the length of bone resection was taken into account, significant differences were found in two factors: need for walking aids and walking upstairs (P < .05) (Table 4). The MSTS score and TESS score of patients with complications were lower than those of patients without complications. At 24 months after surgery, the MSTS score and TESS score of patients with complications were 70.1% and 74.3%, respectively; the MSTS score and TESS score of patients without complications were 83.2% and 85.6%, respectively. Figure 4 showed a typical case.
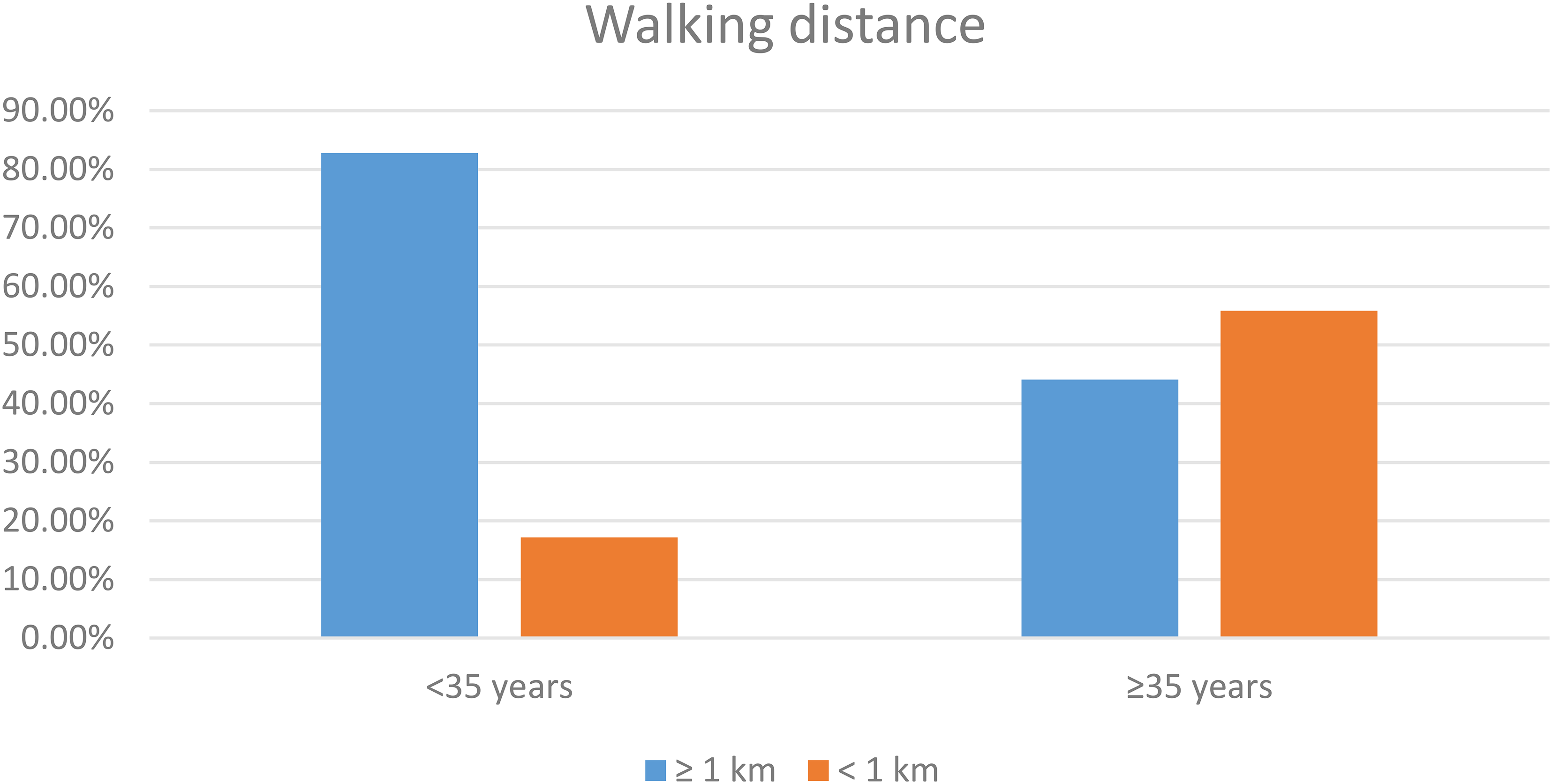
Figure showed the association between changes in age and walking distance, suggesting that younger patients have longer walking distances.
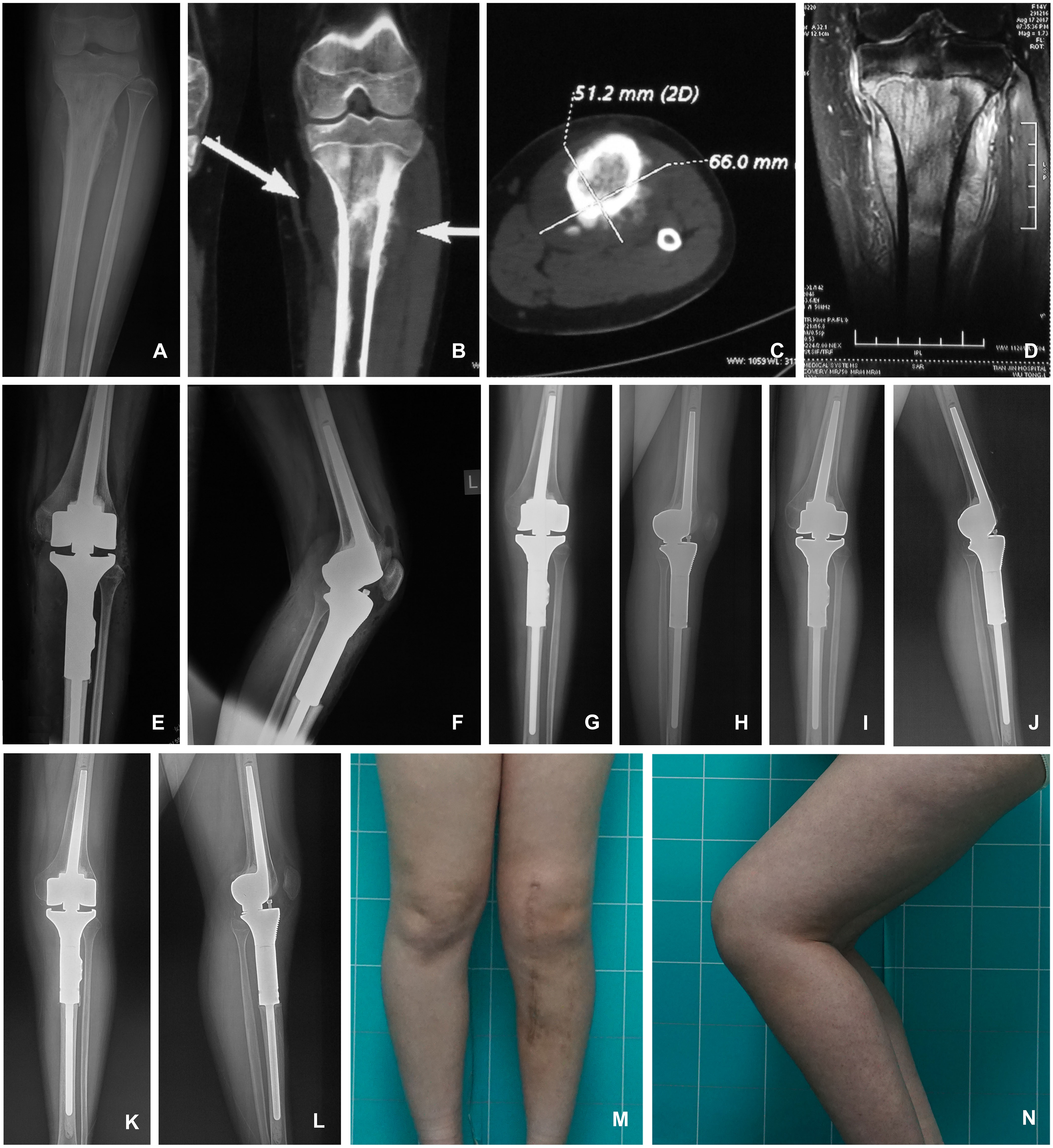
A 14-year-old female patients diagnosed with osteosarcoma at the proximal tibia, who was treated with tumor resection and endoprothesis reconstruction. A. pre-operative AP X ray; B&C. pre-operative CT scanning; D. pre-operative MR scanning; E&F. AP and ML X-rays immediately after operation; G&H. AP and ML X-rays at 3 months after operation; I&J. AP and ML X-rays at 1 year after operation; K&L. AP and ML X-rays at 2 years after operation; M&N. AP and ML photos of the patient's knee. Following operation, the patient retained favourable knee function without local relapse, and the internal fixation is stable without loosening, continuing to the final follow-up (2 years after operation). AP, anteroposterior; ML, mediolateral.
Walking Situation Related to Age, Tumor Site and Length of Bone Resection (N = 183).
Discussion
The current study found that patients had an overall favourable knee functional outcome (mean MSTS: 81.4%, mean TESS: 83.6%; 68% and 73% of patients received perfect or good MSTS and TESS scores) at the final follow-up. Age <35 years, distal femoral prosthesis, and bone resection length <14 cm were independently associated with better functional outcome.
Limb salvage surgery with endoprostheses has steadily increased in patients with primary bone tumors and metastatic lesions over the last decades.2,6,11,12 Although failures and complications of tumor prosthesis remain very common compared to total knee arthroplasty, the functional outcomes are satisfactory in most cases.3,6,12–14 The MSTS and TESS scores are two commonly used tools to evaluate functional outcome after surgery. In the literature, the mean MSTS score after endoprosthetic reconstruction was 58%-88% and the mean TESS was 82%–94%.4,5,15–17 The variability in these scores may be due to differences in implant design, implant type, population ethnicity, and follow-up time, etc. This corresponds to our results in MSTS and TESS scores. In our series, mean MSTS score was 81.4% (60%–100%) and the mean TESS was 83.6% (55%–100%) 24 months after surgery.
Tunn et al. 4 analyzed the functional outcome of 87 patients after endoprosthetic limb-salvage therapy of bone tumors, combining TESS and MSTS scores. They found that TESS (77%) was significantly higher than MSTS (82%), mainly due to the different perceptions between patients and doctors. Therefore, parallel recording of MSTS and TESS for functional assessment may provide an improved understanding of the patient's condition. Similar trends were shown in our study (Figure 2). In addition, we observed significant differences among the functional results at 1, 3, 6 and 12 months after surgery (P < .001 for MSTS and P < .001 for TESS), but no significant differences were observed between functional results 12 or 24 months after surgery (P = .383 for MSTS and P = .245 for TESS). This finding indicates that the majority of recovery occurred during the first year after surgery.
Age
It is generally accepted that the functional outcome after endoprosthetic reconstruction is related to patient age.4,16,18 Tunn et al. 4 found significant differences in both of MSTS score (P = .006) and TESS (P = .001) when the youngest (12–25 years) group and the oldest (41–73 years) group were compared after endoprosthetic limb-salvage therapy. The patients in the >40 years group required analgesia and walking aids more often and reported more rapid tiredness. Toepfer et al. 18 found that the functional outcome was strongly correlated with the patient age: the higher the age, the worse the functional outcome was. Our study supports these conclusions. In the current study, the age was a significant prognostic factor of the functional outcome (P < .001). This result may be due to some physical and psychological factors. Younger patients exhibit better adaptation to a changed physical situation and are more likely to learn to live with their disabilities. We found that more than three quarters of the young patients exhibited a pain-free walking distance of more than 1 km, and most of them did not need walking aids. As for the older patients, the proportion with pain-free walking distance of more than 1 km was only two fifths.
Tumor Site
Several studies have attempted to assess the predictive value of tumor site on functional outcome after endoprosthetic reconstruction, with conflicting results.4,7,13,19 Skaliczki et al. 7 studied the functional outcome of 23 patients who underwent endoprosthetic reconstruction around the knee with a median follow-up of 30 months. They observed that the patients with tumors in the distal femur had significantly better functional outcome and quality of life than those with proximal tibial tumors.
In our study, the multivariate analysis showed that tumor site was an independent prognostic factor of functional outcome after endoprosthetic reconstruction (P < .05). The main reason for this result may be the differences in anatomical structure between distal femur and proximal tibia. In most cases of proximal tibial replacements, difficulties with anchoring the patellar tendon and poor soft tissue coverage make the surgery more complicated. 20 Apart from the increased surgical complexity, the braking time of the limb is prolonged. Patients with a proximal tibia replacement experienced a greater extension lag and felt tired more often in daily activities. This result was confirmed in our study when the walking ability was considered. Site-specific differences were found in three factors: knee pain, need for walking aids, and walking upstairs (P < .05).
Length of Bone Resection
The length of bone resection exerted a significant impact on postoperative function of patients undergoing tumor prosthetic replacement and prosthetic survival rate. 21 Kawai et al. 21 noted that the mean net energy cost during walking was correlated with the percentage of the femur that had been resected (r = 0.504, P = .004). Patients who underwent an extra-articular resection had lower mean flexor torque (P = .006) and extensor torque (P = .03) at the knee compared to those who had an intra-articular resection. In our study, multivariate analysis showed that length of bone resection was an independent prognostic factor of functional outcome after endoprosthetic reconstruction (P < .01). The difference caused by different length of bone resection could be due to the different injuries. The more bone that is removed, the less muscle attachment points remain, leaving a larger soft tissue defect. The loss of muscle mass can worsen the ambulation capacity and increase the need for assistance. Trouble-free walking upstairs without assistance was observed more often in patients with short resection of bone, reinforcing our results. This suggests that surgeons should try to avoid removing too much bone and choose a suitable prosthesis under the premise of ensuring the safety of the surgery.
Custom-Made Versus Modular Prosthesis
The discussing on the prosthetic survival and functional outcome of custom-made and modular prostheses has been widely reported. Overall prosthetic survivorship has been frequently regarded as the primary outcome in these studies. Bickels et al. 22 reviewed 110 consecutive patients treated with endoprosthetic reconstruction (73 modular prostheses, 27 custom-made prostheses, and 10 expandable prostheses) after distal femur tumor resection, demonstrating favourable function outcome (85.4% good or excellent functional outcome at 2 years) and high limb salvage rate (96%). The overall prosthetic survivorship was 93% at 5 years and 88% at 10 years, and there was no significant difference in prosthetic survival among custom, modular and expandable groups. In the study of Zhang et al., 23 they selected aseptic loosening as their outcome, showing that there is no significant difference on the aseptic loosening rate between custom and modular groups after tumor prosthetic replacement around the knee. Similarly, Houdek et al 24 also found that there was no difference in implant survival comparing modular and custom endoprostheses for periarticular tumors of the distal femur. Sacchetti et al. 25 showed that type of prosthesis (modular vs custom) is not related with the prosthetic survival in endoprosthetic replacement of the proximal tibia for oncological conditions. However, some other studies reported significantly higher prosthetic survival for modular endoprostheses compared to custom-designed implants.26–29 Schwartz et al. 26 retrospectively compared the outcome of patients treated with cemented distal femoral endoprostheses (101 with custom implants and 85 with modular implants) for musculoskeletal tumors, showing that modular components had a significantly higher overall prosthetic survival (15-year survival: 93.7% vs 51.7%). At the final follow-up, 31/101 (30.69%) custom-casted stems were revised, while only 4/85 (4.71%) forged modular components were revised. Wu et al 27 showed that custom design prosthesis is associated with a higher risk of prosthetic failure (hazard ratio = 8.747 and P = .044) for patients who underwent cemented proximal tibial replacement.
Few studies have compared the functional outcomes of modular and custom implants for reconstruction of the tumor around knee. Malo et al. 30 reported that modular implants were associated with an improved MSTS functional score in patients reconstructed for distal femoral sarcoma resection. However, in the current study, we found that type of prostheses (custom vs modular prostheses) is not related with the MSTS and TESS score. Even so, there are scarce evidence to precisely conclude the effect of the type of prostheses on the knee functional evaluations.
The original prosthesis was customized prosthesis, which required clinicians to predict the extent of osteotomy based on preoperative imaging data, and then with the cooperation of engineers, a prosthesis matching the size of the patient's bone defect and medullary cavity could be manufactured. This is undoubtedly time-consuming and expensive. The most frightening thing is that the patient with bone tumors may miss the best treatment opportunity. With the increase in the amount of tumor prosthesis replacement surgery, custom-made prostheses that take several weeks to produce gradually cannot meet clinical needs, and modular prostheses appear. From the perspective of medical cost and efficiency, modular prosthesis is undoubtedly a better choice. Thus, some more further well-designed researches are required with a larger sample size.
Limitation
The current study has limitations. First, the limitation of our study was related to its retrospective nature. It was impossible to contact all patients and complete the functional score assessments. Some patients could not be included because of incomplete data. Therefore, selection bias cannot be excluded. In addition, different primary tumors have distinct biological behaviors and prognosis. In order to ensure a relatively sufficient sample size and statistical efficiency, we included all pathologic types in the statistical analysis. Then, as the complications such as tumor recurrence, prosthesis loosening, and tumor spread may cause negative influence on the knee functional score, and the complications predominately arose at a relatively long follow-up time (mean time: 79 months), the results from this study only could be used for guiding the short-term (2 years) knee function predicting. Finally, the calculation of the sample size was not conducted in this study, as we have involved a relatively large cohort (n = 183) compared to most of the previous studies on the topic of endoprosthetic reconstruction for patients with tumors around the knee. We have try our best to enroll patients as many as possible in two clinical centers, during a long period between May 2000 and December 2016. Despite this, we recommend that some more prospective studies with larger sample size are required to verify the findings of this study.
Conclusion
In conclusion, our findings suggest that endoprosthetic reconstruction for tumors around the knee may provide good functional results for most patients, at 2 years after surgery. The major recovery occurs in the first year after surgery. The younger patients with distal femoral endoprosthetic reconstruction and short resection of bone are more likely to obtain satisfactory functional results after surgery. Surgeons should try to avoid removing too much bone on the premise of complete resection of tumor and choose a suitable prosthesis under the premise of ensuring the safety of the surgery. Patients and physiotherapists should also have an advance estimate of rehabilitation plan and limb function.
Footnotes
Abbreviations:
Acknowledgments
We thank all the participants in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Review Statement
This study received institutional review board approval by the ethics committees of Tianjin Hospital (Tianjin City, China; approval number: (2021) Medical Ethics Review No. 231; approval date: December 22nd, 2021) and Jinan Military General Hospital (Jinan City, Shandong Province, China; approval number: (2018) Research Ethics Review No. 26; approval date: August eighth, 2018). Informed consent was obtained from the patients verbally, at the time of telephone follow-up on information about postoperative functional assessment.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article