
Abstract
Introduction
The diagnosis of pulmonary nodules is based on imaging findings, and the widespread use of low-dose computed tomography (CT) for lung cancer screening has increased the detection rates of pulmonary nodules. 1 Pulmonary nodules may be precancerous or may signify early lung cancer. Radiological signs suggestive of malignant pulmonary nodules are lobulation, spiculation, and pleural indentation on CT images, and 18F-fluorodeoxyglucose hypermetabolism on positron emission tomography–CT. 2 Some benign nodules also share these features.3,4 Patients have a good prognosis, with a 5-year survival rate of up to 100% following surgical resection.5,6 Premature surgical resection of such lesions leads to the following problems: organ damage, loss of pulmonary function, and postoperative complications. Moreover, early surgery does not significantly improve overall patient survival, compared with follow-up elective surgery. Preoperatively suspected as malignant, the nodule might turn out to be benign postoperatively. The patient thus undergoes an unnecessary surgery which carries a risk of complications. Owing to the aging population, the incidence of early lung cancer has increased in persons above 75 years of age. These patients are often poor surgical candidates because of poor pulmonary function and increased risk of other complications.7,8 The diagnosis of pulmonary nodule creates psychological distress in some patients, which drastically affects their quality of life. 9 To overcome these problems, researchers should develop novel methods for treating pulmonary nodules. Microwave ablation (MWA) has been increasingly applied in the treatment of early lung cancer as a precise and minimally invasive technique.10,11 MWA is less traumatic, highly efficacious, safe, repeatable, and adaptable for a wider population. Factors such as nodular enrichment, adjacent large vessels, or pulmonary hypertension substantially increase the risk of bleeding during a needle biopsy. However, ablation followed by biopsy could be performed with a relatively low risk of hemorrhagic complications even for patients with hypervascular tumors.12–16 This study aimed to compare the clinical data, technical success rates, complications, and efficacy of 2 different CT-guided puncture techniques for simultaneous needle biopsy with MWA for the treatment of suspected malignant pulmonary nodules.
Methods
The inclusion criteria were as follows: (a) patients with a poor cardiopulmonary function who could not tolerate surgery; (b) those who refused to undergo surgical resection; (c) no hilar or lymph-node metastasis; (d) follow-up time ≥6 months; (e) patients with metastatic pulmonary nodules without extrapulmonary metastases who had previously undergone primary tumor resection; and (f) platelet counts >50 000/μL.
The exclusion criteria were as follows: (a) irreversible coagulation disorders; (b) severe chronic obstructive pulmonary disease; (c) severe emphysema and pulmonary fibrosis; (d) cachexia; (e) severe cardiopulmonary insufficiency; (f) severe pulmonary hypertension; and (g) paroxysmal psychosis.
Necessary auxiliary examinations, electrocardiogram, and routine blood tests (including coagulation profile, and function tests for liver and kidney) were performed preoperatively. Patients were also trained to breathe. Preoperatively, an intravenous access was established, and oral antitussives and sedatives were administered. Patients fasted for 4 to 6 h before surgery. An oncologist with >10 years of experience in lung biopsy and thermal ablation treated both patient groups (Figure 1). Intraoperative monitoring of vital signs (respiratory rate, heart rate, blood pressure, temperature, and oxygen saturation) was done. All patients provided written informed consent.

Surgical items: (A) 18 G biopsy needle, (B) 17 G coaxial trocar, (C) microwave ablation antenna, and (D) 15 G coaxial trocar.
The following procedures were carried out in the coaxial diagnosis and treatment group. Based on the location of the nodule on preoperative contrast-enhanced chest CT, patients were positioned to obtain the optimal puncture approach. CT was performed with a 3 mm slice thickness with a 1.0 mm thin section reconstruction of the region of interest. The puncture needle insertion point and path were set and marked. Disinfection and draping of the body surface were done. Local anesthesia was achieved using 6-10 mL of 1% lidocaine solution. Before puncture, a 1.6 mm MWA needle was placed into a 15 G coaxial introducer needle (Argon Medical Devices, USA) to confirm the matching and the rubber ring position was adjusted to reserve 3 to 4 cm in front of the ablation needle. The parietal pleura was punctured after inserting the 15 G coaxial introducer needle in a stepwise manner along the predetermined path. The needle tip location at the lesion was confirmed with CT. After removing the stylet, an MWA antenna (MTC-3C MWA instrument SFDA 20163251059; Nanjing VISON Medical Equipment Co. Ltd, Jiangsu, China) with a diameter of 1.6 mm was inserted into the distal end of the nodule. The ablation antenna was removed and replaced with a disposable 18 G semiautomatic biopsy gun (Argon Medical Devices, USA), and 2 to 3 pathological tissue samples were obtained. The disposable MWA antenna (water-cooled) was reintroduced through the coaxial cannula into the distal end of the nodule and its position in the lesion was confirmed using CT. After estimating the ablation range required to cover the lesion, the ablation device was activated. Ablation power in the range of 40 to 60 W was delivered over a period of 5 to 10 min. The maximum ablation range was approximately 3.5 cm × 4.0 cm. Chest CT was performed immediately after ablation to confirm the ablation range and to observe any complications. When necessary, the directions of the cannula and microwave antenna were adjusted to reach different parts of the lesion for complete ablation. Postoperatively, patients were observed for 24 to 48 h to detect and manage complications promptly (Figure 2).

A 67-year-old woman presenting with pure ground-glass node (pGGN). (A) A 1.3 × 1.2 cm ground-glass node in the upper right lobe of a 67-year-old woman. (B) The ablation antenna has been inserted through the coaxial trocar during operation, followed by ablation at 30 W for 1 min. (C) Biopsy has been performed by ablation, the nodule is completely replaced by ground-glass opacities. Histopathological examination revealed an invasive adenocarcinoma. (D) One month after microwave ablation, the nodule has been completely covered by ground-glass opacities.
In the noncoaxial diagnosis and treatment group, a 17 G introducer needle, 18 G biopsy gun, and MWA needle were used for the noncoaxial diagnosis and treatment group. The MWA antenna was first passed to the center of the nodule 0.5 cm past the distal end, and ablation at 30 to 40 W was performed for 1 min. An additional puncture path to reach the nodule was created using a 17 G trocar. The 18 G biopsy gun was used to obtain 2 to 3 pathological tissue samples. Following the biopsy, the trocar was inserted on the posterior side of the nodule, followed by MWA. The ablation power was similar to that described above (Figure 3).

A 65-year-old woman presenting with a ground-glass node (GGN). (A) A 1.0 × 0.9 cm GGN in the right middle lobe of a 65-year-old woman. (B) The microwave ablation antenna has been inserted into the nodule center. (C) The trocar and biopsy needle has been inserted along an alternate puncture path to complete the biopsy sectioning. (D) One month after microwave ablation, the nodule has been completely covered by ground-glass opacities. Histopathological examination revealed adenocarcinoma in situ.
The data of 81 patients, each with a suspected malignant pulmonary nodule who underwent CT-guided needle biopsy with simultaneous MWA between September 2016 and September 2021 at the Department of Oncology, were retrospectively analyzed. The associated complications and treatment efficacy were observed and recorded. The following parameters were defined: operative success was defined as the simultaneous completion of biopsy and MWA; efficacy was defined as no tumor progression. Safety was assessed based on complications associated with needle biopsy and MWA. Complete tumor ablation (assessed on immediate postablation CT) was suggested by the presence of ground-glass opacities around the nodule, ranging from 0.5 to 1.0 cm. Patients underwent enhanced chest CT at 1, 3, and 6 months following MWA. To determine efficacy, we used the disease characteristics at postoperative 1 month as the baseline. The response was assessed based on the sum of the diameters of the enhanced areas in the arterial phase of the lesion as follows: complete response (CR), no tumor enhancement; partial response (PR), 30% decrease; stable disease (SD), without PR or progressive disease (PD); and PD, 20% increase or appearance of new lesions.
Statistical Analysis
SPSS 22.0 software package (RRID: SCR_002865) was used for data processing. Continuous parameters were tested for normality, and parameters were expressed as means ± standard deviations, whereas categorical variables were expressed as numbers and percentages. The independent t test was used for the comparison of continuous variables between 2 groups while the chi-square test was used to compare categorical variables. P < .05 was considered statistically significant.
Results
Clinical Data
A total of 81 pulmonary nodules in 81 patients aged 30 to 86 years (59.6 ± 11.4), including 42 men and 39 women, met the inclusion criteria. The nodule size ranged from 0.5 to 2.5 cm (1.29 ± 0.43). The coaxial diagnosis and treatment group (group A) included 41 patients with 41 suspicious malignant pulmonary nodules, whereas the noncoaxial group (group B) included 40 patients with 40 pulmonary nodules. Chronic obstructive pulmonary disease was present in 10 patients in group A and 11 patients in group B. Smoking history was present in 10 patients in group A and 9 patients in group B. The average size of the pulmonary nodules was 1.25 ± 0.44 and 1.32 ± 0.42 cm in groups A and B, respectively. There was no statistical difference in the baseline characteristics between the 2 groups (Table 1).
Baseline Patient Data in the 2 Groups.

Abbreviations: pGGO, pure ground-glass opacities; mGGO, mixed ground-glass opacities; SN, solid nodule.
Histopathological Results
Following biopsy, pathological results were obtained from 78 suspected malignant pulmonary nodules. Group A had atypical adenomatous hyperplasia (9), adenocarcinoma in situ (adenocarcinoma in situ [AIS]; 2), minimally invasive adenocarcinoma (MIA; 2), adenocarcinoma (12), inflammatory nodules (8), lung tissue by puncture (2), and 4 nodules had other findings (2 cases of squamous cell carcinoma, 1 case of small-cell lung cancer, and 1 case of endometrial cancer lung metastases). Group B included atypical adenomatous hyperplasia (6), AIS (7), MIA (4), adenocarcinoma (12), inflammatory nodules (5), lung tissue by puncture (1), and 5 other findings (2 cases of squamous cell carcinoma, 1 case of lung metastasis of breast cancer, and 1 case of carcinosarcoma) (Table 2).
Pathological Results of Puncture Biopsy in the 2 Groups.

Abbreviations: AAH, atypical adenomatous hyperplasia; AIS, adenocarcinoma in situ; MIA, minimally invasive adenocarcinoma; IA, invasive adenocarcinoma.
Technical Success Rate and Complications
Following MWA, all patients underwent contrast-enhanced chest CT at 1, 3, and 6 months, with a follow-up time of >6 months. Complete ablation was achieved in all 47 malignant nodules (AIS/MIA/invasive adenocarcinoma [IA]), with a CR rate of 100% (47 out of 47). Lesions without a response were assessed as SD or PD. No patient died during the follow-up.
Development of severe intraoperative pneumothorax (lung compression >50%) in 3 out of 81 patients led to discontinuation and failure of MWA-synchronous biopsy; the technical success rate of the procedure was 96.3%. The major complications were pneumothorax, hemoptysis, and chest pain. The incidence of pneumothorax was 56.1% (23 out of 41) and 30.0% (12 out of 40) in groups A and B, respectively, the difference being statistically nonsignificant (P = .084). Moderate (lung compression >20%) and severe (lung compression >50%) pneumothorax developed in 5 cases from group A and in 3 cases from group B. Of these, 3 patients in group A and 2 patients in group B underwent drainage. Patients with mild pneumothorax were treated conservatively. The incidence of hemoptysis was 39.0% (16 out of 41) and 17.5% (7 out of 40) in groups A and B, respectively, the difference being statistically significant (P = .015). Of the 16 group A patients who had hemoptysis, 6 had minimal (≤10 mL), 10 had moderate (>10 mL, ≤100 mL), and none had severe (>100 mL) hemoptysis. Of the 7 group B patients who developed hemoptysis, 6 had minimal and 1 had moderate hemoptysis. The incidence of chest pain was 34% (14 out of 41) and 40% (16 out of 40) in groups A and B, respectively, the difference being statistically nonsignificant (P = .759). Air embolism, bronchopleural fistula, or needle implantation metastasis was not observed in either group (Table 3).
Incidence of Complications Following Treatment Using the 2 Techniques.
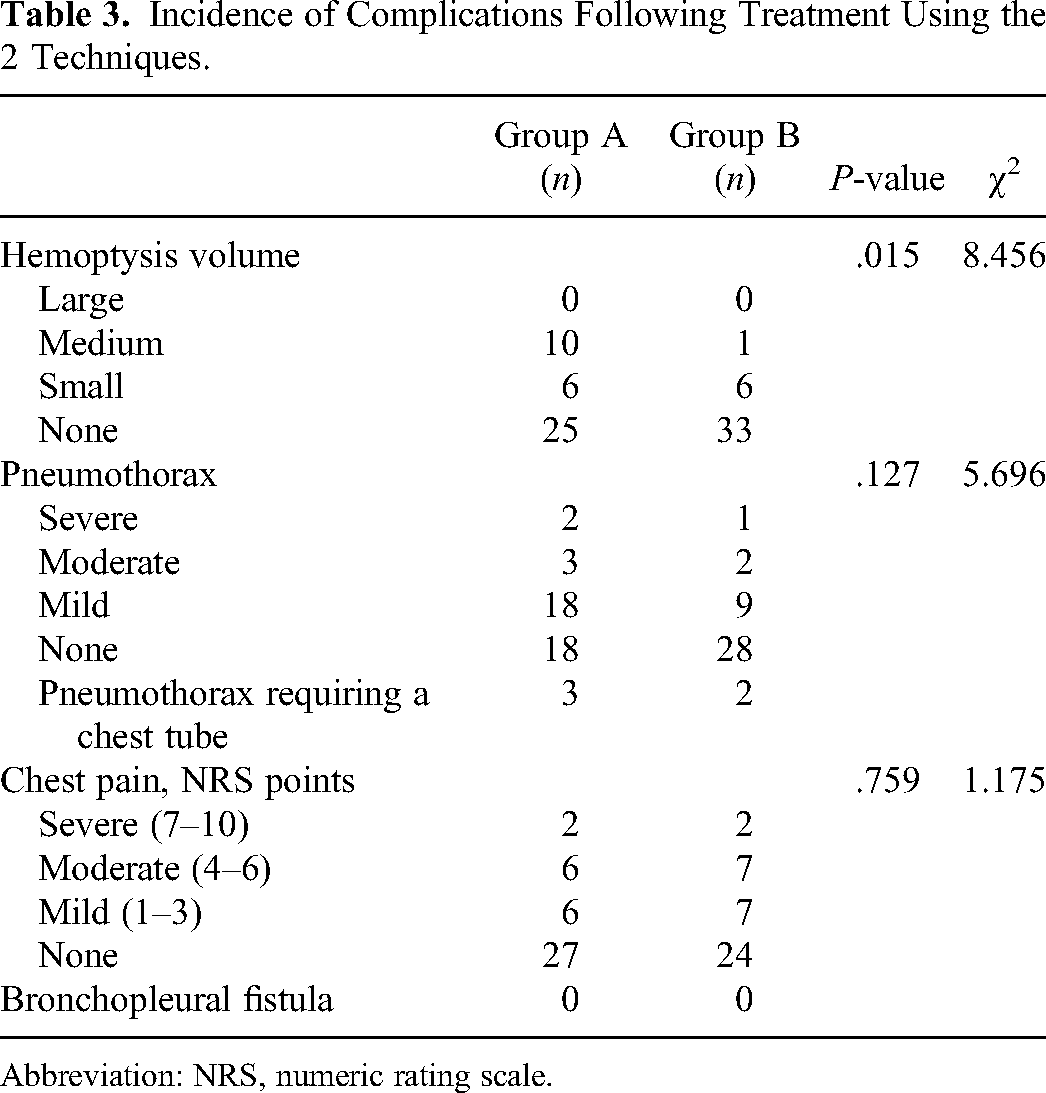
Abbreviation: NRS, numeric rating scale.
Discussion
The application of low-dose CT for lung cancer screening has increased the annual detection rates of pulmonary nodules. Surgical resection is the primary mode of diagnosis and treatment of pulmonary nodules with malignant features, but cannot be performed in patients who refuse surgery, have precluding comorbidities, or are of older age. Currently, such patients with lung tumors are often treated with the effective, safe, and reliable method of percutaneous ablation therapy, that is, MWA. MWA generally uses 2 frequencies—915 MHz or 2450 MHz. Under a microwave electromagnetic field, polar molecules in tumor tissues, such as water and protein, vibrate at extremely high speeds. The resulting collisions and friction between them rapidly generate temperatures as high as 60 °C to 150 °C; coagulative necrosis of the cells ensues. The radiator effectively concentrates the microwave energy within a certain range to effectively radiate the target area. Microwave thermal radiation causes higher convection and lower heat deposition in the lung.10,17
MWA is widely used because of the advantages of fewer injuries, fewer complications, multiple indications, rapid recovery, repeatability, and short treatment duration, being equieffective to surgical resections.18,19 MWA or radiofrequency ablation can coagulate small vessels of approximately 2 mm in the lungs; hence, biopsy following ablation can reduce pulmonary parenchymal hemorrhage and improve positive biopsy rates.14–16,20 In this study, all patients underwent 30 to 40 W ablation for 1 to 2 min, followed by needle biopsy. This study compared the advantages and disadvantages of performing MWA and simultaneous needle biopsy with both coaxial and noncoaxial techniques. There are several studies on the coaxial technique, reporting technical success rates of >98%.15,21 These rates are consistent with the overall technical success rate achieved in the present study (96.3% in both groups). Complete ablation of all lesions was achieved in all technically successful procedures in this study. This 100% ablation rate achieved is consistent with previously reported rates.
Common complications of lung puncture and percutaneous ablation include pneumothorax, bleeding, and chest pain, whereas infection, pleural effusion, hemothorax, and bronchopleural fistulas are uncommon complications. Rare complications include air embolism, cold shock, and rib fractures. Chi et al 21 reported that the incidence of pneumothorax was 25% in coaxial biopsy combined with MWA for ground-glass nodes. In this study, the incidence of pneumothorax was 56.1% and 30% in the coaxial and noncoaxial groups, respectively, with drainage required in 3 cases of the coaxial group and in 2 cases of the noncoaxial group. All cases recovered after drainage, without significant difference between the 2 groups. Wang et al 15 reported that the incidence of hemoptysis following pulmonary-nodule ablation was 22%. In this study, the incidence of hemoptysis was 39.0% and 17.5% in the coaxial and noncoaxial groups, respectively, and this difference was statistically significant. Since the coaxial trocar was thicker, it was repeatedly adjusted to prevent stab injuries to the pulmonary vasculature. In a previous study, the concurrent use of the fixed-needle technique in needle biopsy could reduce the incidence rate of complications. 22 The technique used in this study was similar to that of the noncoaxial technique used in the present study. An MWA antenna was inserted into the center of the nodule, followed by a needle biopsy. The antenna could act as a fixed needle, helping the needle biopsy trocar accurately hitting the lesions and avoiding increased intrapulmonary bleeding due to repeated trocar adjustments.
The preliminary findings in this study indicate that concurrent MWA and needle biopsy for the treatment of suspected malignant pulmonary nodules are feasible. Both coaxial and noncoaxial techniques can be used with equal efficacy, but the incidence of hemoptysis was lower with the noncoaxial technique than was with the coaxial technique. However, this study included a few cases, had a short follow-up duration, and was a retrospective study based on data from a single center, which may have introduced some limitations and data deviations. Further studies are required to identify the optimal technique for simultaneous needle biopsy and MWA.
Conclusions
In conclusion, CT-guided needle biopsy combined with MWA is safe and effective for the treatment of suspected malignant pulmonary nodules. Although clinicians can use both techniques, based on the findings in this study, the noncoaxial technique is recommended.
Footnotes
Abbreviations
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Statement
The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. The study was conducted in accordance with the Declaration of Helsinki (as revised in 2013). The study was approved by the local Institutional Review Board (No. 2018-Ethics Review-08) and individual consent for this retrospective analysis was waived.
Funding
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: This work was supported by the Medical and Health Science and Technology Development Program of Shandong Province, China (No. 2017WS591).