
Abstract
Review efficacy and safety of minimally-invasive treatments for Low Urinary Tract Symptoms (LUTS) in patients affected by Benign Prostate Hyperplasia (BPH). We performed a systematic review of the literature from 1993 to 2022 leveraging original research articles, reviews, and case-studies published in peer-reviewed journals and stored in public repositories. Prostate artery embolization (PAE), transurethral needle ablation (TUNA), transurethral microwave thermotherapy (TUMT), high intensity focused ultrasound (HIFU), laser treatments and Cryoablation are valid and safe alternatives to the gold standard (surgery) in the treatment of LUTS in patients affected by BPH, with fewer undesired effects being reported.
Keywords
Introduction
Lower urinary tract symptoms (LUTS) represent a highly prevalent condition, affecting approximately 70% of men over the age of 80. 1 The most frequent cause of LUTS is benign prostatic hyperplasia (BPH), caused by an increase in the number of epithelial and stromal cells in the transition zone of the prostate.1,2
Cellular aging, hormonal changes, and genetic background all contribute to prostate hypertrophy, which causes compression of the prostatic tract of the urethra and obstruction to the outflow of urine.3,4 DHT and estrogens play a crucial role in the development of BPH, yet they represent only one of several factors that contribute to this condition. The importance of DHT-mediated signaling is further confirmed by the proven efficacy of 5alpha-reductase inhibitors, which represent the cornerstone for the treatment of BPH. However, it is to be noted that recent studies highlight a potential role for low testosterone levels and hyperestrogenism in chronic inflammation of the prostate and the subsequent development of BPH.5,6
Urinary symptoms associated with BPH are typically voiding symptoms such as urinary urgency (pollakiuria) and increased frequency of daytime and nocturnal urination (nocturia). Other less frequent symptoms are reduced urinary output, urinary pain (stranguria), and feeling of incomplete bladder emptying (tenesmus). 7 The severity of these symptoms is assessed by means of several questionnaires, such as the International Prostate Symptom Score (IPSS) and the quality of life (QoL).8,9 Several studies reported that LUTS have a detrimental effect on QoL with considerable economic repercussions.10,11
The treatment of symptomatic BPH is often multimodal. Lifestyle modifications and pharmacological treatment (alpha-adrenergic antagonists, beta-adrenergic agonists, 5-alpha-reductase inhibitors, anticholinergics, phosphodiesterase-5 inhibitors, and phytotherapeutics) represent standard first-line treatments. 12 In selected cases, or when pharmacological treatments lose efficacy, a surgical approach is needed. Options include transurethral prostatic resection (TURP) or open prostatectomy (OP), the former representing the gold standard for the surgical treatment of LUTS. 13
Monopolar (m-TURP) and bipolar (b-TURP) approaches yield overlapping results in terms of symptoms improvement, yet b-TURP proved to be superior for the treatment of larger prostates (>60 g) and associated with lower incidence of resection syndrome (also known as TUR-syndrome) and postoperative bleeding.14,15 TUR-syndrome arises from the electrolyte imbalance caused by the absorption of electrolyte-free irrigation fluids employed in m-TURP, thus being replaced by isotonic fluids in b-TURP.
Postoperative complications such as erectile dysfunction and retrograde ejaculation, in addition to specific risks posed by general anesthesia, led to the development of less invasive surgical techniques such as prostatic urethral lift (PUL) and minimally-invasive interventional radiology approaches such as prostatic artery embolization (PAE), transurethral needle ablation (TUNA), transurethral microwave thermotherapy (TUMT), high intensity focused ultrasound (HIFU), laser treatments and partial cryoablation. These techniques, while limiting the side effects of surgery, may be less effective in urethral unblocking.13,16
AIM of the Study
The aim of this review is to dissect and compare state-of-the-art interventional approaches to BPH. These minimally invasive techniques represent a valid alternative for patients who can no longer continue medical therapy or are ineligible to surgery.
Materials and Methods
We performed a systematic review of the literature from January 1993 to January 2022 leveraging original research articles, reviews, and case-studies published in peer-reviewed journals and stored in public repositories among which PubMed and the Cochrane Library.
Our review is compliant with the relevant equator guidelines, preferred reporting items for systematic reviews and meta-analyses (PRISMA) (Figure 1).

PRISMA flow diagram.
We revised relevant clinical trials on minimally-invasive treatment of BPH published in peer-reviewed journals.
Research and selection of relevant studies were conducted via multiple search systems: PubMed, Google Scholar, MEDLINE, and Scopus.
PubMed was interrogated by the Boolean search string “prostatic artery embolization” AND “benign prostatic hyperplasia OR BPH,” “ablation” AND “benign prostatic hyperplasia OR BPH,” “microwave thermotherapy” AND “benign prostatic hyperplasia OR BPH,” “laser treatment” AND “benign prostatic hyperplasia OR BPH,” “cryoablation” AND “benign prostatic hyperplasia OR BPH.”
Inclusion criteria included original research focusing on mini-invasive treatments for LUTS in the setting of BPH. Of the 53 articles selected, 16 of them were published in the past 5 years.
Our review has been registered with INSPLAY with INPLASY2022120004 as registration number.
Prostate Artery Embolization (PAE)
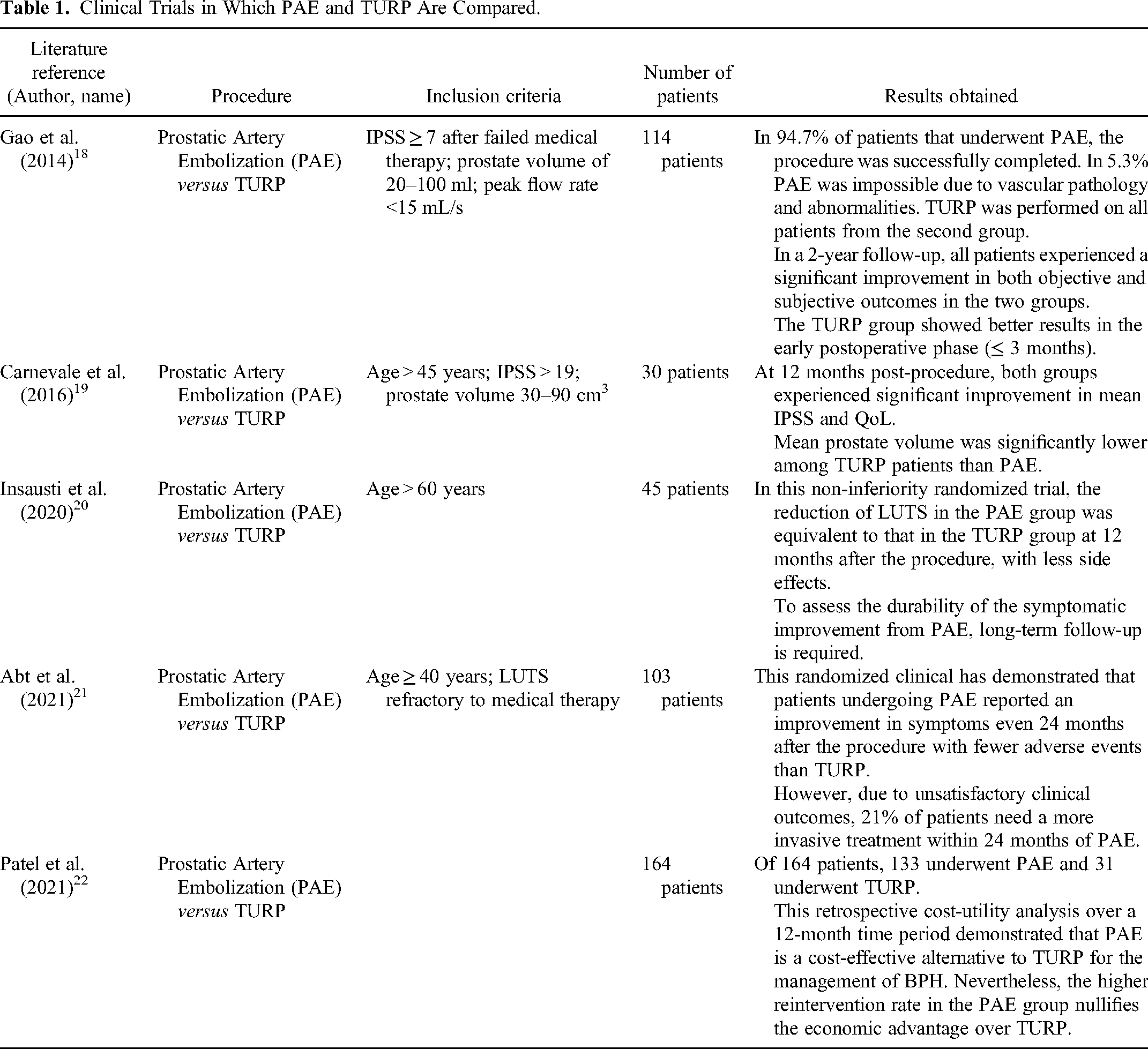
The Society of Interventional Radiology (SIR) has ratified PAE is safe and effective for the treatment of urinary symptoms caused by BPH as outlined in Table 1. 17
Clinical Trials in Which PAE and TURP Are Compared.
PAE had been historically limited to emergency settings, ie massive hematuria, until DeMeritt and colleagues incidentally proved it also led to a reduction in prostate volume and LUTS alleviation. 23
Postprocedural shrinkage and softening of the gland have been evaluated and confirmed by several studies.24,25
PAE leverages local anesthesia and uni- or bi-lateral femoral accesses. Patency and anatomy of iliac vessels is then assessed. Prostatic artery is later identified via superselective catheterization and polyvinyl alcohol microspheres are released, leading to ischaemic necrosis of target volume. 18
The possibility to treat large prostates makes PAE an elective procedure compared to TURP, which is not recommended in prostates >80–100 mL. Studies have shown a prostate volume reduction of more than 44% in prostates of 550 mL.26,27
A further advantage concerns the economic aspect. One study compared the costs of TURP with those of PAE. In PAE there are no costs related to hospitalization and anesthesia, resulting in a third of the costs of TURP. 28
It is to be noted that significant vascular abnormalities and severe atherosclerosis may complicate and even impede the execution of PAE.19,29
Xu et al confirmed the superiority of TURP for both subjective and objective outcomes, but demonstrated that PAE is a safe and valid alternative in the treatment of LUTS due to BPH in patients who refuse or are ineligible for standard surgery. 30
Gao et al compared TURP and PAE at 12 and 24 months post-procedure. 18 In the long term, the results overlapped. A significant difference was appreciated in the group undergoing TURP in the first 3 months post-procedure, explained by the fact that TURP directly removes part of the transition zone. The results of PAE are more evident later because the histopathological changes of the prostate require a longer time following the reduction of blood supply. 18
Carnevale et al further confirmed the comparable efficacy in terms of reduction of IPSS, QoL, and also prostate-specific antigen (PSA) in both groups treated with PAE or TURP. 19
The absence of significant long-term data does not allow for inference regarding long-term efficacy and feasibility of PAE. 30
Transurethral Needle Ablation (TUNA)
Leveraging transurethral access, TUNA delivers energy in forms of radio frequencies to the target prostatic tissue by means of a monopolar 490 kHz electrode, causing intracellular heating (70-110 °C) and eventual necrosis.31,32
Modern devices allow for dynamic power regulation as they perform real-time analysis of tissue impedance and temperature to avoid thermal damage to adjacent non-target tissues. TUNA has several advantages when compared to TURP, such as lower costs and no need for general anesthesia and represents a valid alternative when medical therapy is no longer effective or unfeasible and patients are unfit for surgery.11,32,33
Law et al listed as inclusion criteria for TUNA side effects of medical therapy in 19% of patients, reluctance for chronic medication in 32.2% and persistence of symptoms despite medical therapy in 48.8%. 11 This study demonstrated a significant improvement in urinary symptoms after TUNA by reporting a 65% improvement in IPSS and 75% improvement in QOL. 11
Several controlled studies have compared TURP and TUNA and proved that surgery offers more effective urethral disruption than TUNA as summarized in Table 2.32,34,35
Clinical Trials with TUNA Procedure.

Hill et al demonstrated the safety of this technique with fewer side effects than surgical treatment. 37 The improvement in urinary symptoms assessed by IPSS is statistically greater in TURP than in TUNA in the first 4 years after the procedures but at 5 years of follow-up, TUNA proved to be a viable alternative to TURP.
Transurethral Microwave Therapy (TUMT)
Another outpatient mini-invasive technique that has proven effective in improving urinary symptoms from BPH is TUMT.
Under local anesthesia, the treatment catheter is placed through the urethra under transabdominal or transrectal ultrasound guidance. The catheter delivers a higher frequency radiofrequency (RF) than TUNA, typically between 915 and 1296 MHz, that produces electromagnetic radiation with an oscillating magnetic and electric field. 13 Microwaves absorbed by tissue are responsible for the movement of water molecules, which in turn release energy in the form of heat (45-60 °C), which causes coagulative necrosis of prostate tissue. The latest generation catheters optimize the focal intraprostatic concentration of microwaves by reducing their dispersion along the catheter itself, responsible for possible side effects such as urinary retention. 13
Many studies have confirmed the safety and effectiveness of TUMT, with fewer reported side effects than surgical treatment as reassumed in Table 3.13,38–40 However, Hoffman et al proved TUMT inferior to TURP in reducing LUTS with a mean IPSS of 8.2 versus 5 in TURP and a QoL of 58.7% versus 63.4% respectively. 41
Clinical Trials Evaluating the Efficacy of TUMT.

Djavan et al. 39 evaluated the effectiveness and security of TUMT compared to medical therapy for 18 months during which medical therapy had a 7-fold failure rate.
Walmsley et al. 13 compared the different outcomes of patients undergoing TUMT versus TURP and concluded that the margin of improvement in urinary symptoms is greater with TURP than with TUMT, which, however, has a significantly lower adverse event profile.
Wagrel et al. 43 assessed the safety and efficacy of the technique in a relatively short follow-up time. Little data is available on long-term efficacy over >12 months.
High-Intensity Focused Ultrasound (HIFU)
High-Intensity Focused Ultrasound (HIFU) is a non-invasive technique with clinical application for the thermal ablation of benign and malignant tissues. 44
Different studies have been conducted for the application of HIFU in the treatment of uterine fibroids, in the palliative treatment of pain from bone metastases, and in the treatment of prostate cancer and BPH.45–47 In HIFU, frequencies of 0.8–4 MHz with intensities between 400–10 000 W/cm2 are used, unlike conventional diagnostic ultrasound, which works at frequencies between 2–15 MHz and intensities of 0.004–7.5 W/cm2. The mechanical waves of the HIFU are concentrated by special transducers in the area of interest where the temperature reaches 55 °C causing coagulative necrosis of the affected tissue. For real-time treatment evaluation and subsequent monitoring, HIFU can be performed under ultrasound (US-HIFU) or magnetic resonance (MR-HIFU) guidance.
In their in vivo dog experiments, Hynynen et al. 48 were the first to introduce MR-HIFU, allowing the technique's effectiveness and safety to be increased. Compared to US-guidance, magnetic resonance imaging (MRI) provides a better assessment of soft tissue and the possibility to more accurately monitor the temperature reached in the tissue, but they constitute a challenge because of the need for MRI-compatible instruments.
The clinical trials (reported in Table 4) demonstrated the effectiveness of HIFU in the treatment of BPH in the short-term post-procedure.
Clinical Trials with HIFU Procedure in the Treatment BPH.

In a few patients, Bihrle et al. 49 observed a 48.4% reduction in IPSS at 90 days.
Madersbacher et al. 50 reported a persistence of IPSS reduction even at 12 months follow-up. However, the 4-years follow-up it was necessary for 43.8% of patients to perform TURP.
The main limitation of HIFU remains related to the difficulty of temperature control due to heat loss, which prevents proper concentration of the waves and can ultimately lead to incomplete ablation. 44
Laser Treatments
The side effects of TURP have promoted the development of new alternative techniques such as laser resection, as reported in Table 5. Different types of lasers have been introduced that allow transurethral resection of the hypertrophic portion of the peri-urethral prostate such as Holmium Laser (Holmium Laser Enucleation Prostate
Clinical Trials Evaluating the Efficacy of Various Laser Treatments.

The Nd:YAG laser (neodymium-doped yttrium aluminium garnet) and the Holmium laser were the first techniques developed around the 1960s and are still used today. 52
The laser beam source is placed at the end of an endoscope inserted transurethrally similar to the resectoscope used in TURP. Lasers use different wavelengths and frequencies to induce coagulative necrosis in the target area. The rate of tissue penetration and the thermal effect is related to waves absorption by the tissue. Waves that are not absorbed, on the other hand, are reflected and are responsible for side effects in adjacent tissues. 52
Laser techniques, particularly HoLEP and ThuLEP, show overlapping results when compared to open prostatectomy in terms of decompression and removal of obstruction and at the same time allow for optimal control of haemostasis. 59 The difference lies in the type of wavelength that is pulsed for the holmium laser and continuous for the thulium laser.
In the randomized clinical trial, Ahyai et al. 54 compared HoLEP with TURP. Although TURP is still considered the gold standard for the treatment of LUTS, laser resections have shown excellent results in reducing urinary symptoms with fewer side effects than surgery.
In a prospective randomized trial, Bozzini et al. 57 compared ThuLEP and transurethral resection of the prostate in saline solution (TURis). TURis is a variant of b-TURP that, unlike classic monopolar TURP, employs saline solution as irrigation fluid, therefore lowering the incidence of fluid reabsorption syndrome. ThuLEP and TURis showed overlapping results both in terms of IPSS and QoL at 3-month follow-up. ThuLEP proved to be superior in terms of blood loss, catheterization time, irrigation volume, and hospitalization. 57
Cryoablation
MRI-guided partial cryoablation has already been approved for the treatment of intermediate-risk prostate cancer.60–62
Selected cases of BPH may also benefit from the employment of this technique, endowed with fewer risks than generalized cryoablation, such as erectile dysfunction, incontinence, and recto-urethral fistulas by targeting only the part of the gland that causes urinary symptoms.
At the time of writing, published data in peer-reviewed journals regarding focal cryoablation in BPH is still limited, hence cryoablation remains a second/third-line therapy when medical or surgical therapy fails. Two pilot studies focused on the topic as shown in Table 6.63,64
Articles with Partial Cryoablation in BPH.

The first study was conducted on 21 patients who did not benefit from medical therapy and was unfit for surgery, leveraging on US guidance. 64
Focal cryoablation resulted in a significant reduction in PSA at 4 weeks and a clear improvement in urinary flow rate (UFR). 64
A case report focused on cryoablation under MRI-guidance in patients unresponsive to multiple lines of treatments. 63 Percutaneous accesses on both sides of the urethra were positioned within the hyperplastic transition zone of the prostate. Correct positioning of needles was then checked via MRI. Once benignity was confirmed with biopsies, simultaneous cryoablation was then conducted on the two hyperplastic zones of the prostate responsible for compression of the urethra.
MRI guidance proved to be superior when compared to US guidance because it is not susceptible to imaging artifacts due to the ice ball formation.
Despite modest statistical power due to the small cohorts of patients, both studies yielded promising results. 63,64 Positive urinary flow responses with no complications such as recto-urethral fistulas and decreased daytime and nocturnal urinary frequency were reported.
Discussion
At the time of writing, TURP still represents the gold standard for the treatment of symptomatic BPH in patients with inadequate responses to medical treatment.
However, TURP is endowed with significant adverse effects, namely bleeding, retrograde ejaculation, and transurethral resection (TUR) syndrome due to excessive reabsorption of electrolyte-free irrigation fluids. 59 The incidence of TUR-syndrome has been reduced with the use of TUR is technique, which combines bipolar energy with isotonic solutions as irrigation fluid instead of the electrolyte-free solution of classic TURP. 14 Large prostates (>80 mL) are a further limitation for TURP. 16
The aforementioned possible complications and contraindications to TURP have promoted the development of alternative, minimally-invasive approaches for the treatment of moderate-to-severe LUTS secondary to BPH.
Most minimally invasive alternatives provided overlapping results when compared to TURP in terms of symptom improvement assessed by scores such as IPSS and QoL. The main advantages are represented by the avoidance of general anesthesia and the lower occurrence of side effects. Furthermore, being outpatients’ options, they are less invasive and less expensive than TURP.
PAE proved to be inferior to TURP in the short term because shrinkage of the gland and reduction in obstructive symptoms can only be observed approximately 3 months after the ischemic damage. In the 12-month follow-up, however, the effects obtained with PAE are comparable to those obtained with TURP. 18
At the time of writing a limited number of studies focusing on long-term results of PAE have been published in peer-reviewed journals. Bilhim et al. 65 demonstrated PAE represent a safe and effective strategy to treat LUTS due to BPH, with a 20% re-intervention rate at 5 years and 30%–60% after 5 years post-procedure.
Furthermore, PAE is feasible for large prostates for which TURP is not recommended. 26
The disadvantage concerns the limitation related to the tortuosity of the vascular anatomy that may impair the success of the procedure, which may still be overcome with the transradial approach. 29
Radiofrequency techniques such as TUNA and TUMT provide more rapid results than PAE, comparable to TURP because they leverage wave-induced coagulative necrosis. However, they are able to remove a smaller portion of prostate than TURP, thus with lesser results in terms of unblocking, but with a lower complication rate.13,32 Despite the lack of long-term data, both techniques were found to be effective and safe.40,66
HIFU, which uses radiofrequency waves to induce thermal ablation of the treated tissue, needs further investigation. Under ultrasound (US-HIFU) or magnetic resonance imaging (MR-HIFU) guidance, the correct insertion of the treatment needle into the tissue can be monitored. 48
However, the difficulty of focusing the waves in the target area to reach temperatures suitable for inducing coagulative necrosis renders this technique still inefficient. Further studies will be needed to limit wave dispersion and control heat concentration. 44
The application of lasers in the treatment of LUTS due to BPH has sparked growing interest since the introduction of the Nd:YAG laser and the holmium laser (HoLEP). 52
Lasers with different wavelengths and frequencies make it possible to induce coagulative necrosis of the hypertrophic zone of the prostate responsible for urinary symptoms and simultaneously control hemostasis, therefore, reducing the risk of bleeding. 52
Some lasers, ie HoLEP, are feasible in patients who are receiving anticoagulant therapy. 57
Another recent alternative for the treatment of BPH is partial cryoablation, endowed with less adverse events such as erectile dysfunction or recto-urethral fistulas and collateral damage to healthy surrounding tissues than total cryoablation. Technical difficulties regarding the thermal beam explain the limited popularity of this technique to date. 63
To conclude, we believe each one of the approaches described in this review possesses unique features, strengths, and drawbacks. One may object such a wide range of possibilities might translate into an undesirable degree of variability in terms of clinical decisions and outcomes, with individual centers making arbitrary decisions based on their specific expertise, availability of qualified personnel, and presence of dedicated facilities. It is tempting to speculate that a jack-of-all-trades, gold-standard approach should be identified once and for all. However, we believe the existence of several treatment options will and should be a fundamental asset in the era of so-called “precision medicine,” in which each patient is treated as a unique individual with peculiar features and needs, worthy of receiving a bespoke customized treatment.
Key patients’ features to help clinicians identify the most appropriate treatment strategy for their patients are summarized in Table 7.

Conclusion
Although minimally invasive treatments have proven to be effective, TURP remains the gold standard in the treatment of LUTS due to BPH.
Among mini-invasive procedure, no technique proved to be indisputably superior in every context and for every patient, especially because subjective patients’ preferences need to be taken into account.
While one patient may express stronger interest in preserving antegrade ejaculation, another might opt for the least invasive procedure or the one that is endowed with the lowest risk of re-intervention.14,51
Additional investigation is thus needed to evaluate the efficacy and feasibility of individual treatment options in the long-term.
Footnotes
Acknowledgements
We have nothing to declare.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.