
Abstract
Introduction
Gastric cancer (GC) is one of the most common malignancies in the world and the third leading cause of cancer-related deaths. 1 Currently, radical GC surgery is the only means to cure locally progressive GC; however, lymph node (LN) metastasis in most GC patients greatly affects survival and prognosis.2–4 LN metastasis is an independent risk factor for tumor recurrence after radical GC surgery, and standardized and thorough LN dissection is directly related to the clinical prognosis of GC patients. Therefore, strengthening intraoperative LN tracing and dissection is the key direction of GC treatment.5–8
Carbon nanoparticles (CNPs) are the most widely used and well-studied vehicles for LN visualization and lymphoma-targeting chemotherapy in GC.9,10 The CNPs can follow the flow of lymphatic vessels around the tumor, accumulate in the LNs, and stain black. 11 This improves the intraoperative clearance and postoperative detection of LNs, especially micro LNs. Several studies12–16 have confirmed that nanocarbon helps improve the rate and number of LNs detected during radical surgery for GC. However, as the application of CNP in lymphadenectomy for patients with GC is still in the preliminary stages, its safety and efficacy remain unclear.
We systematically analyzed and evaluated the clinical utility and safety of CNP in patients GC by reviewing relevant domestic and international literature, and by meta-analysis, with the aim of evaluating the value of CNP as a tracer in LN localization.
Materials and Methods
This meta-analysis was performed in accordance with the Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) statement. 17
Study Objective
In this meta-analysis, the primary endpoint was the total number of retrieved LNs, and the secondary endpoints included the number of metastatic LNs, operative time, intraoperative blood loss, and postoperative complications (such as anastomotic leaks, incision infections, pneumonia, and intestinal obstructions). The total number of LNs retrieved and number of metastatic LNs were used to assess the effectiveness of CNP tracer-guided LN dissection, operative time, intraoperative bleeding; postoperative complications and were used to assess its safety.
Search Strategy and Literature Inclusion Criteria
To identify all publications relevant to the safety and efficacy of CNP-labeled LN dissection in the radical resection of GC, we performed a comprehensive literature search using PubMed, EMBASE (Ovid platform), Web of Science, and Cochrane Library, from the inception of the library to October 16, 2022. The search terms were the following: “neoplasm, stomach” or “stomach neoplasm” or “neoplasms, stomach” or “gastric neoplasms” or “gastric neoplasm” or “neoplasm, gastric” or “neoplasms, gastric” or “cancer of stomach” or “stomach cancers” or “gastric cancer” “cancer, gastric” or “cancers, gastric” or “gastric cancers” or “stomach cancer” or “cancer, stomach” or “cancers, stomach” or “cancer of stomach” or “gastric cancer, familial diffuse” and “carbon nanoparticles” or “carbon nanotracers” or “CH-40” or “nano-carbon”. The references of the included studies and related systematic reviews were tracked. Our research was limited to English language articles and not to time periods.
Eligible studies for this meta-analysis met the following criteria: patients were confirmed to have GC by pathological or histological examination; patients with and without CNP tracer-guided radical gastrectomy; articles with the most complete data for studies with duplicated data; retrospective and prospective research, as well as randomized controlled trials (RCTs); the full publication was written in English. The exclusion criteria were review articles, case reports, abstracts, editorials, letters, and meta-analyses. We also excluded articles without direct comparisons, those without sufficient data for analysis (even after contacting the study authors), and duplicate publications.
Data Extraction
Two reviewers (ZCL and WJH) independently extracted relevant data from the eligible studies using a per-design data form. Disagreements were resolved by discussion. Data retrieved from each publication included the basic characteristics of each study, such as the first author, year of publication, country, number of patients in the CNP and non-CNP groups, operative method, number of retrieved LNs, number of metastatic LNs, operative time, intraoperative blood loss, and postoperative complications. Unless the standard deviation (SD) could be obtained from reading the publication, we recalculated the SD from published data using Cochrane's official recommended “data conversion tool”. This tool is an Excel conversion template created by Amy Drahota and Elaine Bellor based on the formulas provided in the Cochrane Handbook. 18
Quality Assessment
Quality assessment of each eligible study was performed by the same reviewers (ZCL and WJH) who extracted the data. They independently read and scored each publication according to the Newcastle–Ottawa Quality Assessment Scale (NOS). 19 This method assesses 3 parameters of quality: selection (0-4 points), comparability (0-2 points), and outcome assessment (0-3 points), with total scores ranging from 0 to 9. A study with a total score greater than 7 was considered high quality in the present meta-analysis.
Statistical Analysis
Odds ratios (ORs) and weighted mean differences (WMDs) with their corresponding 95% confidence intervals (CIs) were used to analyze dichotomous and continuous variables. Heterogeneity was tested using the Q statistic and the I2 test. If the P value was more than 0.1 or I2 was less than 50%, then all included studies lacked heterogeneity; thus, the Mantel–Haenszel method (fixed effect model) was used to merge the studies. Otherwise, a random effects model was adopted. For the source of heterogeneity, a sensitivity analysis of each study and subgroup analysis were used for secondary analysis. Egger's or Begg's tests were used to evaluate publication bias. Subgroup analyses were performed for different countries, sample sizes, operation methods, and study designs. Statistical analyses were performed using STATA version 12.0 (StataCorp, College Station). Statistical significance for 2-sided tests was set at P < .05.
Results
Literature Search and Study Baseline Characteristics
A total of 115 abstracts were identified using the search strategy. After screening these abstracts, 7 studies12–16,20,21 involving 1827 patients (551 in the CNP group and 1276 in the non-CNP group) with GC were eligible and included in the present meta-analysis. The process of selecting studies is illustrated in Figure 1. All the research was published between 1998 and 2022 and came from 2 different nations (Italy and China). The sample sizes ranged from 26 to 1199 patients. Patient characteristics and baseline data are presented in Table 1. The mean NOS score of all included studies was 7.6, indicating high methodological quality of the included studies.

Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) flow diagram of the meta-analysis.
Characteristics of Included Studies.

Abbreviations: CNPs, carbon nanoparticles; LTG, laparoscopic total gastrectomy; LSG, laparoscopic subtotal gastrectomy; nCNPs, non-carbon nanoparticles; NR, not reported; NOS, Newcastle–Ottawa Quality Assessment Scale; P, prospective; R, retrospective study.
Characteristics of CNP Injection
The characteristics of CNP injections are shown in Table 2. Most studies have used endoscopy for submucosal injections, which were performed during or a few days before surgery. No CNP-related complications were reported in any of the studies.
Characteristics of CNP Injection.
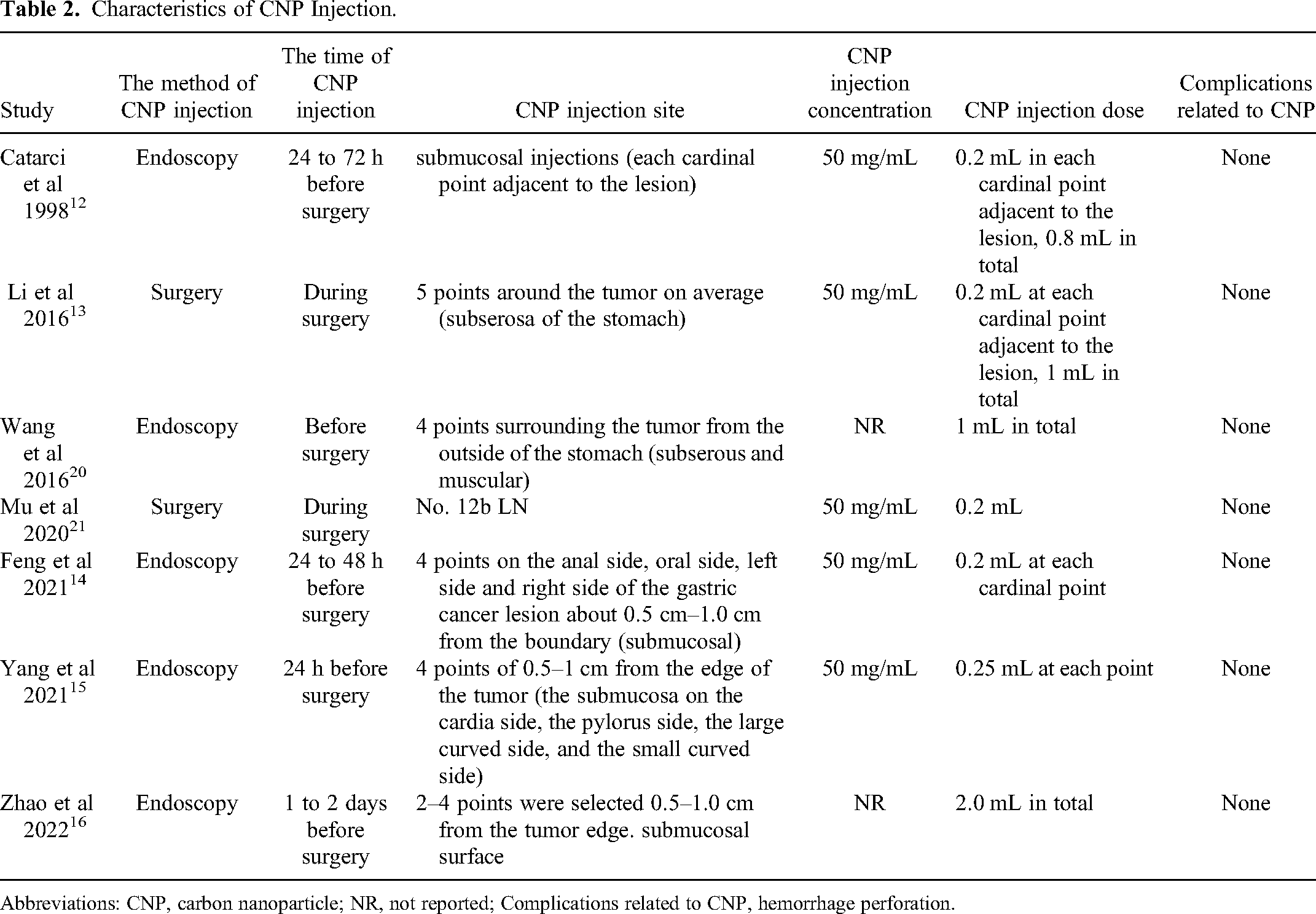
Abbreviations: CNP, carbon nanoparticle; NR, not reported; Complications related to CNP, hemorrhage perforation.
Number of LNs Detected
The primary outcome of this study was the assessment of the CNP tracer-guided number of retrieved LNs after radical gastrectomy. The number of intraoperative LNs detected was addressed in all 7 included studies. The results of the heterogeneity analysis showed that P < .05 and I2 = 96.4%, indicating heterogeneity among studies; therefore, the random effects model was used for analysis. The combined results showed a statistically significant difference in the number of LNs detected in the CNP group compared with the non-CNP group [WMD = 6.67, 95% CI = (3.71-9.62), P < .01], suggesting that CNP tracer-guidance had a positive effect on increasing the number of retrieved LNs. The forest plot is shown in Figure 2.

Forest plot of weighted mean difference (WMD) for the number of intraoperative lymph nodes (LNs) detected.
Number of Metastatic LNs Detected
Three of the included studies reported the number of LN metastases. The results of the heterogeneity analysis showed that P = .65 and I2 = 0.0%, indicating mild heterogeneity among the studies; thus, a fixed effects model was used for the combined analysis. The results showed that the number of detected LN metastases was higher in the CNP group compared with the non-nanocarbon group, and the difference was statistically significant [WMD = 1.60, 95% CI = (0.09-3.12), P = .038] (Figure 3).

Forest plot of weighted mean difference (WMD) for the number of metastatic lymph nodes (LNs).
Operative Time
Three studies reported the operative time. Meta-analysis showed no difference in operative time between the 2 groups (WMD = −11.60, 95% CI: −40.53-17.34, P = .432) with moderate heterogeneity (P < .001, I2 = 89.2%), as shown in Figure 4.

Forest plot of weighted mean difference (WMD) for operative time.
Intraoperative Blood Loss
Three studies reported intraoperative blood loss, all of which showed a statistically significant reduction in the CNP group compared with the non-CNP group. The meta-analysis showed a mean reduction in intraoperative bleeding of 11.33 mL in patients in the CNP group compared with the non-CNP group (WMD = 11.33, 95% CI: 6.30-16.37, P < .01) with low heterogeneity (P = .806, I2 = 0.0%) as shown in Figure 5.
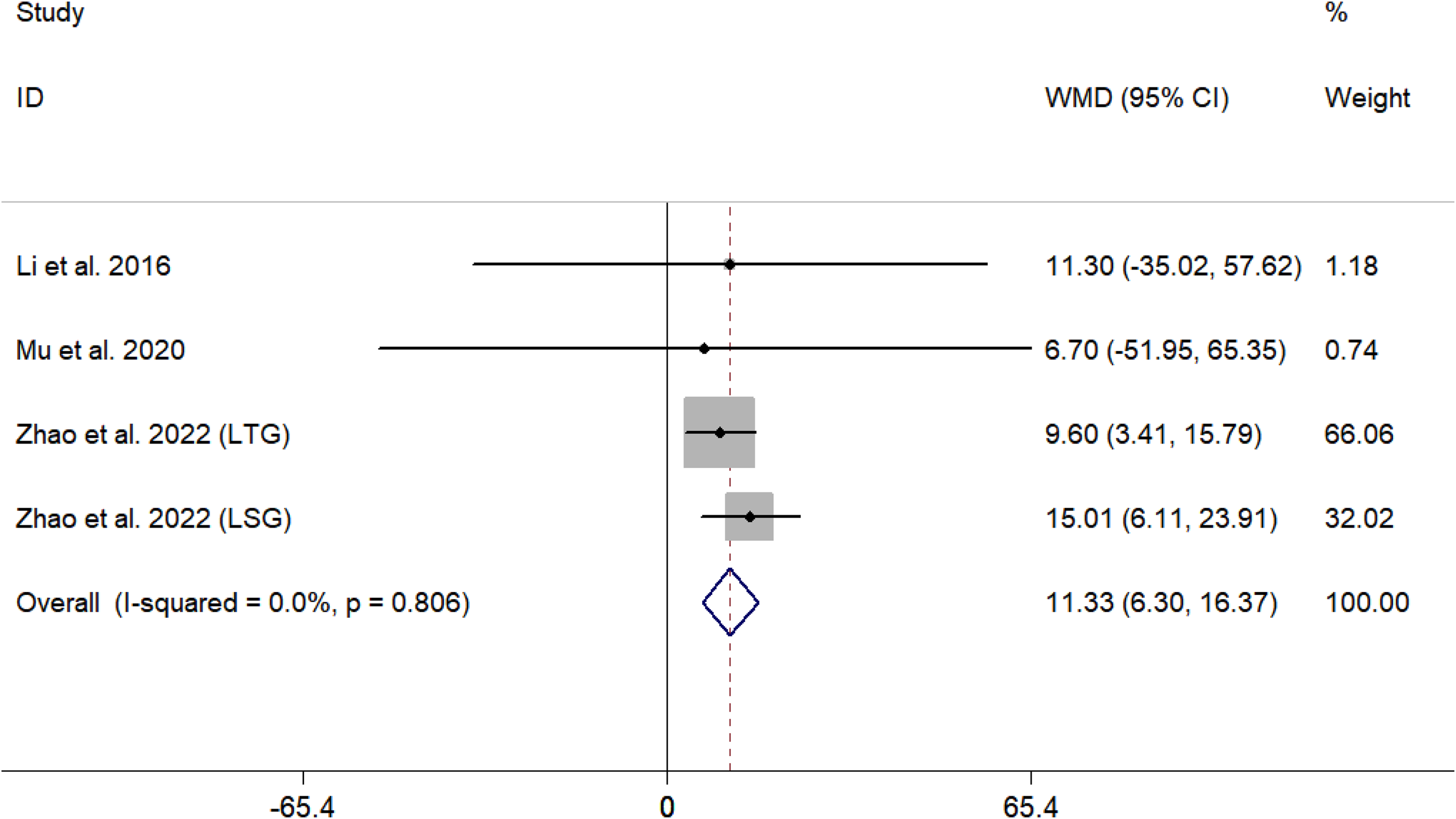
Forest plot of weighted mean difference (WMD) for intraoperative blood loss.
Postoperative Complications
Postoperative complication rates were reported in 5 studies. The results of the heterogeneity analysis showed that P > .05 and I2 = 0.0%, indicating that the heterogeneity between studies was not statistically significant; therefore, the fixed effects model was used for the combined analysis. The results of the combined analysis showed that the incidence of postoperative complications in the CNP and non-CNP groups was not statistically significant [OR = 0.88, 95% CI: (0.52-1.48), P = .623; P > .05]. (Figure 6)
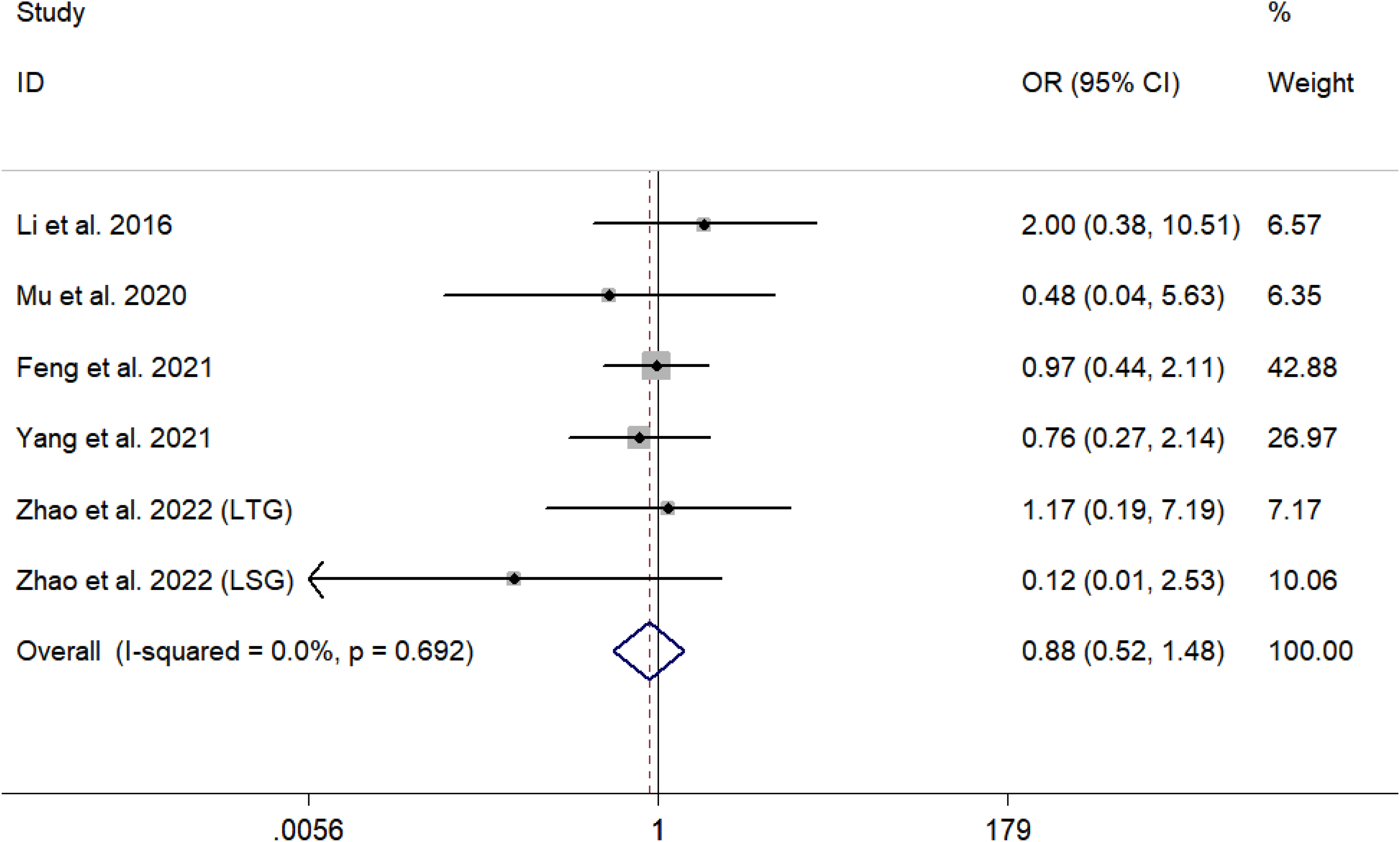
Forest plot of odds ratio (OR) for postoperative complications.
Sensitivity Analysis and Publication Bias
Sensitivity analysis were performed by sequentially omitting individual cohort analyses to assess the reliability and stability of our results. When we excluded any studies, the pooled WMDs and their corresponding 95% CIs were similar. Hence, our findings are relatively consistent and reliable (Figure 7). Egger's and Begg's tests were used to analyze the publication bias in our meta-analysis. There was no evidence of publication bias in the number of retrieved LNs (Egger test, P = 0.721; Begg test, P = 0.902) (Figure 8).

Sensitivity analysis of the intraoperative use of carbon nanoparticles (CNPs) and the number of lymph nodes (LNs) dissected.

Funnel plots evaluating the relationship between the intraoperative use of carbon nanoparticles (CNPs) and the number of lymph nodes (LNs) dissected.
Subgroup Analysis
The results of subgroup analysis (based on sample size, country, operation method, and study design) are presented in Table 3. Subgroup analysis based on “country” suggested that CNP tracer-guided lymphadenectomy was significantly associated with an increasing number of retrieved LNs in China (WMD = 5.73, 95% CI: 3.39-8.07, P < .01), with significant heterogeneity (I2 = 88.5%, P < .01), and Italy (WMD = 9.80, 95% CI: 9.13-10.47, P < .01). In terms of “operation method,” CNP tracer-guided had a positive effect on increasing the number of retrieved LNs in all kinds of operations (open gastrectomy: WMD = 9.80, 95% CI: 9.13-10.47, P < .01; laparoscopic surgery: WMD = 3.92, 95% CI: 3.29-4.54, P < .01; open or robot laparoscopic: WMD = 7.90, 95% CI: 4.42-11.39, P<.05). Regardless of whether the sample size was >60 (WMD = 4.31, 95% CI: 1.95-6.66, P<.01) or ≤60 (WMD = 9.84, 95% CI: 9.18-10.50, P < .01), CNP tracer-guidance showed a positive effect on increasing the number of LNs compared to non-CNP. We found that CNP tracer guidance could increase the number of LN harvested in the retrospective study (WMD = 5.71, 95% CI: 4.80-6.61, P < .01) with no significant heterogeneity (I2 = 0.0%, P = .881) and the prospective study (WMD = 7.11, 95% CI: 6.59-7.63, P < .01) with significant heterogeneity (I2= 97.4%, P < .01).
Subgroup Analysis of WMD for the Number of Lymph Nodes (LNs) Dissected.

Abbreviations: No., number; WMD, weighted mean difference; 95% CI, 95% confidence interval.
Discussion and Conclusions
Recently, with the development of nanotechnology in medicine, nanocarbons have been used in clinical practice. It is not only convenient to stain but also has high lymphatic tropism. Thus, it has become an ideal lymphatic tracer in current clinical practice.22–24 CNP injection is critical for effective LN imaging in radical GC surgery. 9 Most studies12,14–16,20 used endoscopy for submucosal injections, which were performed around the primary tumor within 3 days before the procedure. This definitely increases patient discomfort, medical costs, and physician workload compared to intraoperative CNP injection studies.13,21 However, for early stage tumors, it is difficult to identify the tumor location intraoperatively and subsequently perform CNP injection because the tumor does not break through the plasma layer. Therefore, endoscopic injection is undoubtedly a better choice. Regardless of the method of injection, the vast majority of studies have confirmed that CNP is a significant tracer for the LNs of GC and increases the number of LNs harvested while reducing intraoperative blood loss, without increasing the operative time or postoperative complications. CNP tracer-guided lymphadenectomy is considered safe and effective for gastrectomy. The above findings are consistent with the results of our meta-analysis. Additionally, the subgroup analyses based on country, sample source, operation method, and study design were consistent with the above results.
The main component of CNP is small molecular-weight CNPs with a diameter of 150 nm. 25 Since the basement membrane of capillary lymphatic vessels is incompletely developed, the gap between endothelial cells is 100 to 150 nm, while the gap between capillary endothelial cells is approximately 30 to 50 nm, and the particle size of nanocarbon is in the middle of both of them. Therefore, the nanocarbon particles injected into the sub-plasma membrane of gastric tumors quickly drain into the surrounding lymphatic vessels and LNs and are phagocytosed by macrophages, resulting in a large number of charcoal particles remaining in the LNs and black staining of the LNs, which are easy to intraoperatively identify. 26 Thus, the CNP group was able to obtain higher numbers of LNs, which is consistent with the results [WMD = 6.67, 95% CI: (3.71-9.62), P < .01] in our meta-analysis. Previous studies27,28,29 showed that a larger number of LN dissections was associated with better long-term survival of patients with GC. Therefore, CNP-trace-guided radical gastrectomy may have a better prognosis. Certainly, this needs to be further confirmed by high-quality evidence of long-term survival.
In this meta-analysis, we showed that the number of harvested LN metastases was higher in the CNP group than that in the non-CNP group [WMD = 1.60, 95% CI: (0.09-3.12), P = .038]. The reasons for this may be attributed to the following 2 points: (1) since the LN count is used as a quality measure for GC surgery, 30 the surgeon should obtain as many LNs as possible during the operation, and an increased total number of harvested LNs means a greater possibility of obtaining a higher number of metastatic LNs and (2) the metastatic LNs may change their original morphology, 31 making it easier for the CNPs to remain in the LNs, causing them to stain black. However, this needs to be confirmed through more rigorous experiments in the future.
In terms of intraoperative blood loss, our analysis showed a significant reduction in blood loss in the CNP group compared with that in the non-CNP group. This is most likely due to the fact that black staining of the LNs makes it easier for the surgeon to identify the vascular planes and to distinguish the vascular vessels from the surrounding lymphatic structures, thus reducing the risk of vascular injury. 16 Intraoperative blood loss, operative time, and postoperative complications are important factors in assessing the safety of surgery. The results of our meta-analysis did not show any difference between the 2 groups in terms of operative time and postoperative complications, probably because this is closely related to individual surgical proficiency and experience. This also indirectly proves the safety of nanocarbon.
Based on the available evidence, our study showed that the use of CNP during radical gastrectomy can extract more LNs, minimize intraoperative blood loss, and have short-term effectiveness similar to that of traditional radical gastrectomy. Through a comprehensive review of previous studies, we also found that in addition to being a tracer, nanocarbon may also be a mediator of targeted therapy for GC, which can be used to target residual and micro-metastases for targeted chemotherapy. 32 In summary, CNP-labeled may serve as a safe and effective method for LN tracing. It should be vigorously promoted in clinical practice, and different injection timings should be chosen according to different tumor stages. Larger prospective and standardized investigations should be conducted in the future to confirm our results.
This meta-analysis has some limitations. First, owing to the inherent weaknesses of retrospective studies, the homogeneity test for continuous variables revealed moderate heterogeneity. Second, because most of the included studies were conducted in Asia, the data from this meta-analysis are not applicable worldwide. Third, owing to the relatively small number of included studies and sample size, we were unable to pool the results based on tumor classification. Therefore, larger, multicenter, high-quality studies are urgently needed to confirm our findings. These limitations must be considered when evaluating the findings of our study.
Footnotes
Abbreviations
Acknowledgments
The authors would like to thank Dr Edward C. Mignot, Shandong University, for linguistic advice.
Author’s Contribution
ZCL and DMX made substantial contributions to the conception and design for this work. ZCL and WJH collected all the data. ZCL and WJH were the major contributors in writing the manuscript. DMX and WQ performed the critical revision for this manuscript. All authors contributed to the article and approved the submitted version.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China and the Natural Science Foundation of Gansu Province (grant numbers 82160588, 22JR11RA252).
Ethical Approval
This article did not require an ethical board approval because the study data were downloaded from the open database.
Data Availability
Some or all data, models, or code generated or used during the study are available from the corresponding author upon reasonable request.