
Abstract
Simultaneous mutations in Janus kinase 2 (JAK2), calreticulin, and myeloproliferative leukemia (MPL) genes are generally not considered for characterizing Philadelphia-negative myeloproliferative neoplasms (MPNs), leading to misdiagnosis. Sanger sequencing and quantitative polymerase chain reaction were used to detect gene mutations in patients with MPN. We retrospectively screened the data of patients with double mutations in our center and from the PubMed database. Two patients tested positive for both JAK2V617F and CALR mutations (2/352 0.57%) in our center, while data of 35 patients from the PubMed database, including 26 patients with essential thrombocythemia (ET), 6 with primary myelofibrosis (PMF), 2 with unexplained thrombosis, and 1 with polycythemia vera were screened for double mutations. Among these mutations, co-mutation of JAKV617F-CALR constituted the majority (80.0%), when compared with JAKV617F-MPL (17.1%) and CALR-MPL (2.9%) mutations. Moreover, patients with concurrent mutational myeloproliferative neoplasm (MPN) were relatively older (P = .010) with significantly higher platelet counts than their counterparts with single gene mutations (P < .001). The occurrence of palpable splenomegaly (P < .001) and leukocyte count (P = .041) were also significantly different between patients with single and simultaneous gene mutations. These 4 risk factors also showed significant test effectiveness in the ET and PMF cohorts (P < .05). In terms of clinical characteristics of patients with ET, those with JAK2V617F-CALR mutation had higher but normal hemoglobin levels (P = .0151) than those carrying JAK2V617F-MPL mutation. From a clinical perspective, patients with multiple mutational MPN are different from those with single gene mutations. The poor treatment response by patients in our center and unfavorable indicators for patients with co-mutations in published literature indicate that customized treatment may be the best choice for patients with MPN carrying co-mutations.
Introduction
Myeloproliferative neoplasms (MPNs) are a heterogeneous group of chronic myeloid neoplasms that can potentially progress to acute leukemia. Among its subtypes, except for chronic myeloid leukemia, polycythemia vera (PV), essential thrombocythemia (ET), and primary myelofibrosis (PMF) constitute Philadelphia–negative MPNs and are characterized by mutations in 3 driver genes: Janus kinase 2 (JAK2), calreticulin, and myeloproliferative leukemia (MPL). 1
JAK2, the most common driver gene, is a member of the Janus kinase family and serves as a cognate tyrosine kinase for erythropoietin, thrombopoietin, and granulocyte colony-stimulating factor receptors. The most common mutation of JAK2 in myeloproliferative neoplasm (MPN) is a point mutation in exon 14, named JAK2V617F. This mutation is observed in approximately 90% to 95% of patients with PV and 50% to 60% of those with ET and PMF. 1 Nevertheless, approximately 3% of patients with PV have insertions or deletions in JAK2 exon 12, making the tumor more aggressive than that caused by JAK2V617F mutation. 2 JAK2 mutations are generally associated with older age and characterized by higher hemoglobin level, leukocytosis, lower platelet count, and increased risk of thrombosis; a higher JAK2V617F allele burden is associated with a more aggressive phenotype of pruritus and fibrotic transformation in PV. 3
Mutations in CALR, occupying 50% to 80% of patients with ET and PMF, are the second most common gene alteration that drives myeloproliferation. 4 CALR mutations resulting in ET are associated with younger age and male sex, and are clinically characterized by higher platelet count, lower hemoglobin level, lower leukocyte count, and lower incidence of thrombotic events. PMF arising from CALR mutation is associated with younger age and is characterized clinically by higher platelet count, lower frequencies of anemia, leukocytosis, and spliceosome mutations. 4 To date, deletions in CALR have been designated as type 1 or type 2 mutations, accounting for 85% of the CALR gene mutations. Clinically, type 1 mutations are more common in patients with PMF, whereas both mutations occur at a similar frequency in patients with ET. 5 Patients with ET arising from type 2 CALR mutation were relatively young and had higher platelet counts than their counterparts with type 1 mutations. 6
MPL mutations are the least common drivers of MPN, mostly occurring in PMF and ET. Exon 10 mutations in MPL were found in 3% to 5% of patients with ET and 5% to 8% of those with PMF lacking JAK2 mutation. 7 For patients with ET, MPL mutations are associated with greater myelofibrotic transformation, but there is no difference in the overall or leukemia-free survival between patients with MPL mutations and those with JAK2V617F mutation. Moreover, there appears to be no difference in survival between patients with PMF who have MPL or JAK2V617F mutations. 4
In 2008, the World Health Organization (WHO) approved the use of JAK2 and MPL mutations as biomarkers for MPN diagnosis. Initially, CALR, JAK2, and MPL mutations were thought to be mutually exclusive. 8 However, emerging evidence has shown that mutations in these 3 genes can occur together in some MPN cases. It is estimated that the co-mutation of JAK2, CALR, or MPL is detected in 1% of MPN patients. 9 In 2016, Ahmed et al suggested that JAK2V617F and CALR exon 9 mutations could occur simultaneously. Patients with co-mutations might have a different phenotype and clinical course, distinct from that of patients with a single mutation. 10 Identifying MPN patients with co-mutations and studying the impact of this coexistence on the phenotype and clinical course will be critically important to better understand the diagnosis and prognosis of such patients. 10 However, there is insufficient clinical evidence to support this proposition. In our study, after screening more than 200 patients with MPN, we identified 2 patients with ET with concurrent mutations. We then browsed multiple articles and extracted relevant information, aiming to provide a preliminary analysis of the incidence of simultaneous mutations in patients with MPN and its associated clinical phenotype.
Materials and Methods
Patients
From May 2017 to April 2021, 352 patients with MPN were simultaneously tested for mutations in JAK2 (V617F), exon 9 of CALR, and exon 10 of MPL. All diseases were diagnosed according to the criteria outlined by the WHO. 11 The retrospective study in our center was approved by the Ethics Committee of the Affiliated Hospital of Guizhou Medical University (Approval number: 2021021-FR-01, 2021022-FR-01, 2022023-FR-01; Approval date: 24/3/2022). Informed verbal consent was obtained from all participants for anonymous case reports. Because the study involved are routine clinical tests, we did not get written consent from patients.
DNA Extraction
Total DNA was extracted from fresh BM specimens, or peripheral blood samples were obtained from patients with suspected MPN. A commercial kit (TianGen Biotech Co., Ltd, Beijing, China) was used for DNA extraction. The concentration of the extracted DNA, measured using EPOCH spectrophotometry, was 100–400 ng/L.
Quantitative Polymerase Chain Reaction for the JAK2V617F Mutation
JAK2V617F wild-type and mutant alleles were amplified using 2 independent antisense (AS)-quantitative polymerase chain reaction (qPCR) multiplex reactions, 1 specific for the wild-type allele and the other specific for the mutant allele. JAK2 V617F wild-type and mutant primers were as follows: forward primer 5ʹ-CTTTCTTTGAAGCAGCAAGTATGA-3ʹ, probe 6-FAM-TGAGCAAGCTTTCTCACAAGCAT TTGGTTT-TAMRA, wild-type specific reverse primer 5ʹ-GTAGTTTTACTTACTCTCGTCTCCA CATAC-3ʹ, JAK2V617F mutation-specific primer 5ʹ-GTAGTTTTACTTACTCTCGTCTCCAC ATAA-3ʹ. All AS-qPCR reactions were performed in a Realplex2 Real-Time PCR System (Eppendorf, Germany) and consisted of 15 µL of Maxima Probe/ROX qPCR Master Mix (2 × ) (Applied Biosystems, USA), 3 µL of 10 × JAK-2 Prime Time Assay and 1.5 µL 10 × RNAse P Prime Time Assay, and 10 µL of DNA normalized to 2.5 ng/µL in the following thermocycling conditions: denaturation for 10 min at 95 °C, followed by 50 cycles of 95 °C for 15 s and 60 °C for 60 s. Nontemplate control, positive, and negative controls were used in all reactions. The threshold was always set to 0.1 DeltaRn in all qPCR experiments.
Direct Sequencing for Mutation of Exon 9 in CALR and Exon 10 in MPL
DNA samples from the patients with MPN were assessed for mutations in exon 9 of the CALR gene and exon 10 of the MPL gene using Sanger sequencing, based on a commercial kit (Genome Precision Technology Co., Ltd, Beijing, China), following the manufacturer's instructions. The resultant sequences were compared with GenBank sequences using Sequencher v4.1 software (Gene Codes Corporation, Ann Arbor, Mich, USA). The CALR mutations were classified as previously described. 12
Strategy of Searching Cases in the Literature
Published articles that reported the coexistence of any 2 of the 3 driver gene mutations in Philadelphia-negative MPN were identified in the PubMed database. The relevant genomic and clinical information of the patients was collected. According to guidelines from the international working group, the International Prognostic Score of Thrombosis (IPSET) for ET was calculated using 3 indicators: age, JAK mutation, and history of thrombosis. Similarly, the International Prognostic Scoring System was used for PMF based on age, WBC count, Hb level, number of blasts in peripheral blood, and the presence of systemic symptoms. All indicators were collected before the targeted treatment. Finally, data were integrated into a unified standard.
Statistical Analysis
Statistical data following a normal distribution or that showed similarity to normally distributed data are presented as mean ± SD, and the difference in statistical significance was determined using a t-test. However, the statistical data that did not follow a normal distribution are presented as medians (upper quartile, lower quartile), and nonparametric tests were used for difference analysis. Frequency (%) was used to describe the enumeration data, and chi-square analysis was used to analyze differences. In our study, P < .05 was considered statistically significant.
Results
Incidences of Patients With Philadelphia-Negative MPN Carrying Simultaneous Mutations in the Driver Genes
Numerous studies have demonstrated the presence of concurrent mutations in genes that drive the development of MPN. Therefore, we tested for simultaneous mutations in JAK2 (V617F), CALR exon 9, and MPL exon 10 in 352 patients with MPN enrolled from 2017 to 2021. Accordingly, we found 1 ET and 1 PMF patient with concurrent mutations in JAK2 (V617F) and CALR (2/352, 0.57%).
The patient diagnosed with ET was a 68-year-old woman who had visited a local hospital for routine treatment of a fracture in the right hand that had been sustained a year before. The platelet count was abnormally high (700 × 109/L). In November 2019, she was readmitted to the hospital with nausea and persistent abdominal pain. The platelet count had increased to 900 × 109/L. Surprisingly, the patient showed no significant improvement after completing a dose of Danshen dripping pills (Chinese patented medicine) and clopidogrel bisulfate. The patient was transferred to our hospital in December 2019 for a detailed examination. A full blood examination showed leukocytosis (white blood cell count of 12.04 × 109/L), thrombocytosis (platelets, 947 × 109/L), and normal hemoglobin levels. Blood biochemistry tests from their part revealed slight increases in lactate dehydrogenase (271 U/L) and ferritin (449.40 ng/mL) levels. Sanger sequencing of DNA extracted from bone marrow blood further detected simultaneous mutations in JAK2 (V617F) and CALR (type 1, c.1092_1143del; L367fs*46) genes (Figure 1A-B), and no other variants were detected related to MPN. No specific presence of chromosomal abnormalities, history of thrombosis, or risk of other cardiovascular diseases was noted. The patient was discharged following treatment with aspirin and hydroclopidogrel hydrochloride. One month later, she was readmitted to the hospital for treatment of a new fracture and sustained thrombocytosis. The platelet count had increased to 1198 × 109/L and further increased to 1332 × 109/L after 2 days. After 2 platelet isolation treatments, hydroxyurea and interferon were administered continuously. However, at the time of reporting, the platelet count remained between 600 × 109 and 800 × 109/L. The patient was classified as high-risk based on IPSET for scoring thrombosis. Unfortunately, the patient did not achieve remission after all necessary therapies as stipulated by the National Comprehensive Cancer Network. At the time of this report, ET had not transformed into leukemia.
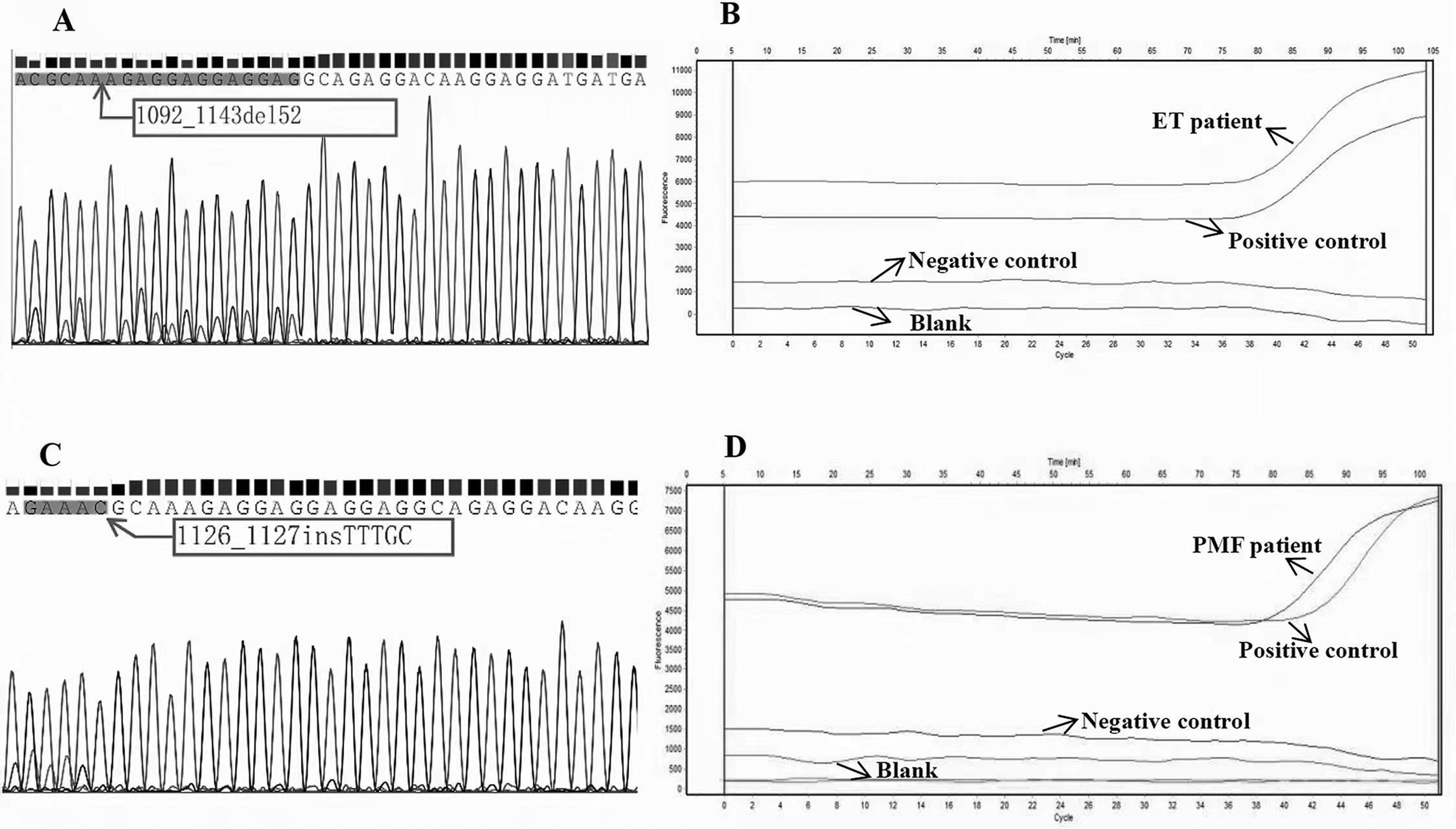
Genetic information of patients treated for MPN carrying double driver gene mutations at our center. A. Mutant location of CALR exon 9 detected by Sanger sequencing in the patient with ET. B. Amplification diagram of JAK2V617F mutation detected by qPCR in the patient with ET. C. Mutant location of CALR exon 9 detected by Sanger sequencing in the patient with PMF. D. Amplification diagram of JAK2V617F mutation detected by qPCR in the patient with PMF.
The patient diagnosed with PMF was an 83-year-old female without any commendable medical history. The patient was admitted to our hospital after experiencing “dizziness for more than 10 days.” Blood tests revealed a high platelet count (1058 × 109/L) and an elevated white blood cell count (11.26 × 109/L). Blood biochemical analysis revealed a significant increase in lactate dehydrogenase (527 U/L) level. Tests for bone marrow morphology suggested decreased bone marrow hyperplasia, including granular, low erythroid, and megakaryocyte hyperplasia. A bone marrow biopsy revealed reticular fibers ( + + + +) (WHO, 2016 13 ), where the main megakaryocytes were naked and monoprokaryotic. Analysis of MPN-related gene mutations revealed alterations in JAK2 (V617F) and CALR genes. Interestingly, the CALR alteration was a new mutant: 1126_1127 in TTTGC; R376Lfs*56 (Figure 1C-D). After platelet removal treatment, the patient was discharged from the hospital but was lost to follow-up.
Genetic Characteristics of Patients With Philadelphia-Negative MPN Carrying Double Mutations in Driver Genes
Due to the small number of Philadelphia-negative MPN patients with double mutations, the clinical characteristics of this disease are poorly understood. In 2016, Ahmed et al reviewed 12 articles with combined data from 34 patients with MPN, reporting concurrent mutations in JAK2 (V617F) and CALR (28 patients with ET, 4 with PMF, 1 with PV, and 1 with unexplained thrombosis (U-MPN)). 10 Although they proposed that the simultaneous mutations in the driver gene may be categorized as a new type of MPN, this hypothesis has not been validated due to limited clinical data. In this study, we searched the PubMed database and screened 23 articles (Supplementary Table).14–36 As a result, 119 patients with MPN were found to display concurrent mutations in MPN driver genes, of which 97 had ET (81.51%, 97/119), 17 had PMF (14.29%, 17/119), 1 had PV (0.84%, 1/119), and 4 had U-MPN (3.36%, 4/119). The mutation combinations included JAK2V617F and CALR (77.31%, 92/119), JAK2V617F and MPL (18.49%, 22/119), and CALR with MPL (4.20%, 5/119). Three mutations in exon 10 of MPL, namely W515L (62.5%, 5/8), W515R (25.00%, 2/8), and W515S (12.5%, 1/8), were observed in patients with JAK2V617F mutation. Among the 3 patients with concurrent mutations in CALR and MPL (W515R) genes, only one had known alterations.
Clinical Characteristics of Patients With MPN Displaying Double-Mutation
To further understand the clinical characteristics of patients with MPN carrying double mutations, we analyzed the pooled clinical data of these patients from the published literature and those from our center (Figure 2). Of the 121 patients (119 from the literature and 2 from our center), 26 with ET (22 from the reported literature and 1 from our center), 6 with PMF (5 from the literature and 1 from our center), 2 with U-MPN (all from the reported literature), and 1 with PV (all from the reported literature) showed complete clinical courses (Table 1). Because of the limited number of patients with PV and U-MPN, we could not perform further analyses.

Flow chart of data extraction and pooling of data used in this study.
Clinical Characteristics of All MPN Patients With Double Driver Gene Mutations.

Abbreviations: MPN, myeloproliferative neoplasm; ET, essential thrombocythemia; PMF, primary myelofibrosis; U-MPN, unexplained thrombosis; PV, polycythemia vera; NA, not available.
We found that 28 (80.0%, 28/35) patients tested positive for JAKV617F-CALR mutation, while concurrent mutations of JAKV617F-MPL (17.1%, 6/35) and CALR-MPL (2.9%, 1/35) occupied a minor proportion. Among the patients with different types of MPN, those with JAKV617F-MPL mutation comprised 73.1% (19/26) of the patients with ET, while all patients with PMF, U-MPN, and PV patients bore the co-mutation for JAKV617F-MPL.
We also detected significant differences in the results of routine blood examinations. The median age of the 26 patients with ET was 66 (23-89) years, with a median platelet count of 1147 (587-2300) × 109/L, far above the normal level of (100-300) × 109/L. Hemoglobin level and WBC count were 133.0 (69.0-156.0) g/L and 10.0(6.0-19.1) × 109/L, respectively.
The median age of the patients with PMF was 75 (49-86) years. The median WBC and platelet counts and hemoglobin levels were 9.8 (5.3-11.7) × 109/L, 451.5(73.0-1170.0) × 109/L, and 119.2 (93.4-149.8) g/L, respectively (Table 1). Three of the Intermediate risk patients displayed enlarged spleens, deep venous thrombosis, or colon bleeding. In terms of prognosis, most patients achieved partial remission after hydroxyurea and interferon therapy.
Comparative Clinical Manifestations of MPN Between Patients With Single-Gene and Simultaneous Gene Mutations
To explore the differences in the clinical characteristics of patients with MPN patients carrying single and concurrent mutations, we pooled our data with information from articles published by the Mayo Clinic, generating a dataset encompassing data from 3023 patients with MPN (Table 2). 37
Comparison of Clinical Courses of MPN Patients With Double Driver Gene Mutations and Single Driver Gene Mutation.
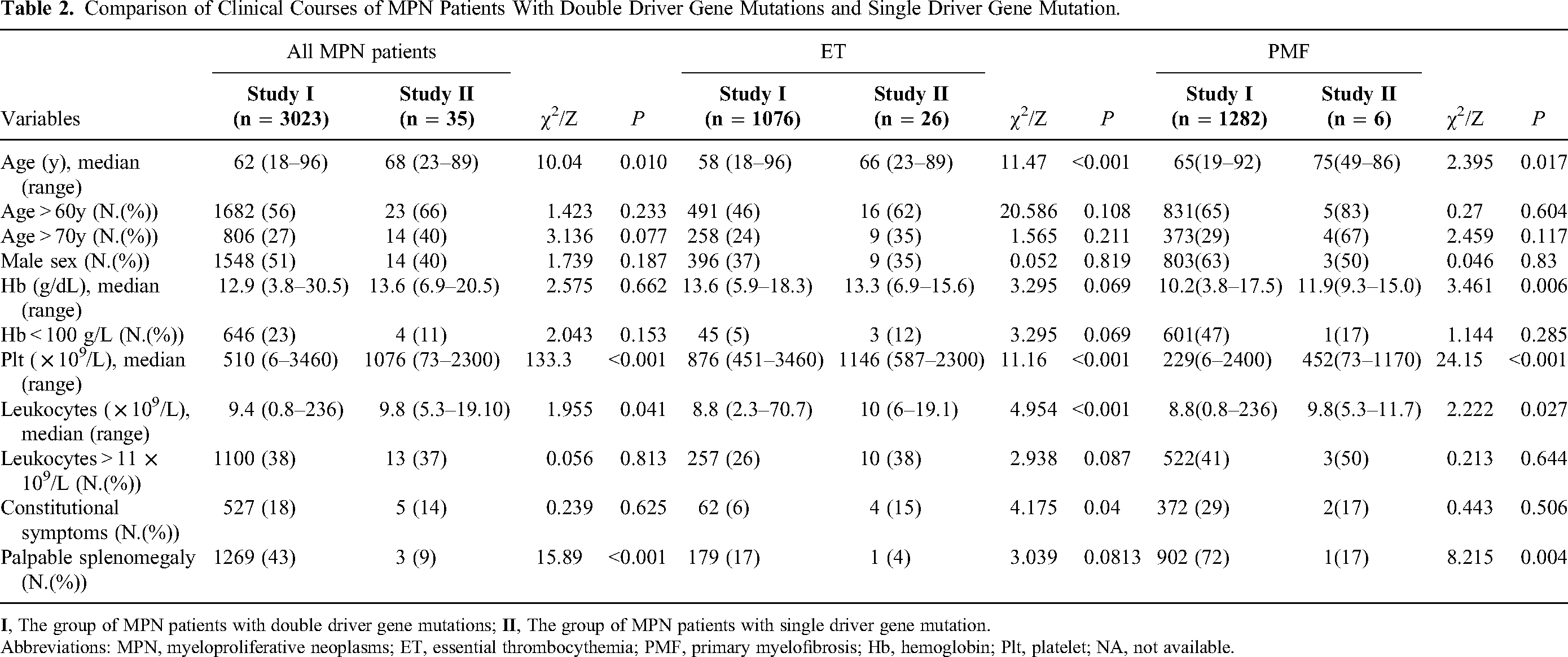
Abbreviations: MPN, myeloproliferative neoplasms; ET, essential thrombocythemia; PMF, primary myelofibrosis; Hb, hemoglobin; Plt, platelet; NA, not available.
The significantly different risk factors between patients with single and simultaneous gene mutations in patients with MPN were platelet count (P < .001), palpable splenomegaly (P < .001), age (P = .010), and leukocyte count (P = .041). The 4 factors also showed significant test effectiveness in the ET and PMF cohorts (P < .05). To illustrate in detail, the median age of patients with simultaneous mutations was 68 (23-89) and 62 (18-96) years for those displaying a single mutation. The platelet count of patients carrying the double mutation was significantly higher than that of patients with co-mutations, which were 1076 (73-2300) × 109/L and 510 (6-3460) × 109/L, respectively. Interestingly, the difference between the clinical characteristics of patients with general MPN and those with ET or PMF carrying co-mutations were similar, with the patients with ET or PMF showing older age (P < .05), higher platelet count (P < .001), and higher level of leukocytes (P < .05). However, we did not find a difference in the incidence of splenomegaly between the cohorts with single-gene and simultaneous gene mutations.
Differences in Clinical Characteristics of Patients With ET Displaying Different Combinations of Concurrent Gene Mutations
Among the 26 patients with ET carrying double gene mutations, 19 displayed JAK2V617F-CALR combination mutations and 6 displayed JAK2V617F-MPL combination mutations. We compared the clinical characteristics of the 2 sets of patients (Table 3). There were no significant differences in age, WBC count, and PLT count (P > .05). However, the level of hemoglobin in a patient with JAK2V617F-CALR mutation was slightly higher than that in patients with JAK2V617F-MPL mutation (P = .015), which were 136.00 ± 15.03 and 110.50 ± 30.64 g/L, respectively. We also compared the data of patients with abnormal hemoglobin levels, WBC count ≥11 × 109/L, and platelet count >1000 × 109/L as well as >1500 × 109/L between the 2 groups of patients and with different sexes. Regrettably, no significant differences were detected between the patients with ET carrying JAK2V617F-MPL and JAK2V617F-CALR mutations (P < .05) (Table 3 and Supplementary Figure).
Comparison of Clinical Characteristics and the Ratio of Abnormal Blood Routine of ET Patients With Different Coexistence of Double Driver Gene Mutations

Abbreviations: Hb, hemoglobin; Plt, platelet; WBC, white blood cell; CALR, calreticulin; MPL, myeloproliferative leukemia; Group A, patients with coexistence of JAK2V617F and CALR; Group B, patients with coexistence of JAK2V617F and MPL.
Discussion
Mutations in JAK2, CALR, and MPL drive MPN development. Separately, they cause different clinical characteristics. However, differences in the clinical characteristics of patients with MPN with concurrent mutations have rarely been reported. Previously, it was thought that JAK2, CALR, and MPL gene mutations were mutually exclusive. This led to a serious underestimation of the proportion of patients with MPN with concurrent mutations in the 3 driver genes. However, the proportion of patients with MPN carrying such newly discovered combination mutations increased significantly with improved detection of driver gene alterations from 2014. 20 Existence of these sub-classifications related to concurrent mutations implies that new subtypes of MPN may be present.
In this study, we tested for simultaneous mutations in the driver gene in patients with MPN at diagnosis. Ultimately, 2 (0.57%) patients (1 with ET and 1 with PMF) with older age and sustained thrombocytosis displayed JAK2V617F-CALR simultaneous gene mutations. However, it is difficult to estimate the long-term prognosis over a short follow-up period. Furthermore, we screened 23 published studies related to simultaneous mutations in the 3 driver genes. Combined with reports published in 2018 by the Mayo Clinic, we collected the data of 35 patients with concurrent mutations, among which ET constituted the major diagnosis, and co-mutation of JAK (V617F) plus CALR accounted for the majority (80%). Moreover, patients with MPN carrying concurrent mutations were relatively older than those with single mutation (P = .010) and were prevalent in patients over the age of 70 (P = .077). 37 This cohort also suffered from thrombocytosis with the median level value of platelet count exceeding 1000 × 109/L (P < .001), palpable splenomegaly (P < .001), and leukocytosis (P = .041). Low hemoglobin levels and conventional risk stratification did not differ between patients with a single mutation.
Additionally, we analyzed the clinical data of patients with ET and PMF separately, which established the same significant risk factors of age and platelet count (P < .05). Patients with PMF carrying simultaneous mutations were more distributed in the INR-2 category. We also analyzed the impact of different combinations of gene mutations on the clinical characteristics of patients with ET. Here, we found that the hemoglobin level in the patients with ET patients carrying a combination of JAK2V617F-CALR mutations was slightly higher than that in patients carrying a mutation in MPL alone (for whom, the corresponding values were within the normal range). However, we found no significant difference between the proportion of patients with abnormal hemoglobin levels and WBC count ≥10 × 109/L (P < .05) in patients with double JAK2V617F-CALR mutations, probably because of the small number of patients with ET carrying only JAK2V617F mutation for MPL. As such, we will continue to collect clinical information from patients with double mutations and provide supplementary information.
In a similar study, it was suggested that patients with double mutations are not only older, and have a higher incidence of arterial thrombotic events after diagnosis, but also belong to the high-risk group with thrombohemorrhagic complications. 20 Moreover, the presence of co-mutation significantly reduced overall survival and increased the risk of conversion to acute myeloid leukemia. Some patients had a poor tolerance or suboptimal response to hydroxyurea or imatinib than expected. 38 Based on this, some researchers suggested that the treatment of these patients should be focused on controlling platelet increase and splenomegaly symptoms instead of using tyrosine kinase inhibitors. 10
Taken together, although some patients with co-mutations reported in the published literature achieved partial remission after standard treatment, we still found a disappointing response in some special cases with poor characteristics. It is possible that traditional treatments cannot meet clinical needs under such conditions. The evidence above underlines the need for customized treatment for patients with MPN with concurrent mutations. 7
However, the patients with ET did not achieve remission, and the patient with PMF was lost to follow-up in our center. The treatment outcome differs from our conclusion, the reasons for which require further exploration. Moreover, the use of different methods for detecting gene mutations in the literature, including next-generation sequencing with high sensitivity and Sanger sequencing with high specificity, has led to inconsistent gene testing sensitivity. Combined with the low-load of gene mutations in patients with MPN, the false-negative rate of laboratory tests was high. Fortunately, the proportion of patients with double mutations is expected to increase significantly with advances in detection methods. Additionally, the co-mutation cases raised the question of whether they were acquired by one malignant clone or within a separate clone. Some researchers have suggested that the special mutations likely originate from 2 independent clones for genomic instability, 27 but more targeted research is still needed to obtain an accurate mechanism, which will help in the clinical treatment of MPN.
Conclusion
The number of patients with MPN with double mutations was highly underestimated. The current study provides insights into the coexistence of double mutations in driver genes and the potential molecular complexity of MPN. Based on the integration of mutational characteristics with the clinical disease course, customized therapies should be formulated to provide accurate predictions for individual patients during the follow-up period. This study outlines the clinical manifestations of MPN in patients with simultaneous mutations in the key genes that drive MPN. This study also provides preliminary evidence to further classify this category of patients into a new subtype.
Supplemental Material
sj-tif-1-tct-10.1177_15330338231154092 - Supplemental material for Genetic and Clinical Characteristics of Patients with Philadelphia-Negative Myeloproliferative Neoplasm Carrying Concurrent Mutations in JAK2V617F, CALR, and MPL
Supplemental material, sj-tif-1-tct-10.1177_15330338231154092 for Genetic and Clinical Characteristics of Patients with Philadelphia-Negative Myeloproliferative Neoplasm Carrying Concurrent Mutations in JAK2V617F, CALR, and MPL by Yan Wang, Fei Ran, Jin Lin, Jing Zhang and Dan Ma in Technology in Cancer Research & Treatment
Supplemental Material
sj-docx-2-tct-10.1177_15330338231154092 - Supplemental material for Genetic and Clinical Characteristics of Patients with Philadelphia-Negative Myeloproliferative Neoplasm Carrying Concurrent Mutations in JAK2V617F, CALR, and MPL
Supplemental material, sj-docx-2-tct-10.1177_15330338231154092 for Genetic and Clinical Characteristics of Patients with Philadelphia-Negative Myeloproliferative Neoplasm Carrying Concurrent Mutations in JAK2V617F, CALR, and MPL by Yan Wang, Fei Ran, Jin Lin, Jing Zhang and Dan Ma in Technology in Cancer Research & Treatment
Footnotes
Abbreviations
Authors’ Contributions
YW drafted the manuscript and DM designed the study. YW, FR, and JZ collected and analyzed the data. YW and FR revised the manuscript and all authors approved the final version.
Acknowledgments
The authors acknowledge the support of Jishi Wang in obtaining the ethics approval.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Statement
The retrospective study in our center was approved by the Ethics Committee of the Affiliated Hospital of Guizhou Medical University (approval number: 2021021-FR-01, 2021022-FR-01, 2022023-FR-01; Approval date: 24/3/2022) and informed verbal consent was obtained from all participants for anonymous case report.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article. This work was supported in part, by the National Natural Science Foundation of China (Nos. 82003835, 82160704 and 81760670), Basic Research Program of Guizhou Province Technology Bureau (No. ZK [2021] General-399, No. ZK [2022] General-451), Science and Technology Program of Guizhou Province Health Committee (Nos. gzwkj2021-466), Guizhou Provincial Natural Science Foundation (No. [2022]4017 and [2021]4029), Project of scientific and technological innovation talent team in Guizhou Province (NO: CXTD[2021]002).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.