
Abstract
Introduction
According to Global Cancer Statistics (GLOBOCAN) 2020, there were approximately 2.2 million new cases of lung cancer globally, accounting for 11.4% of all new cancer patients, and approximately 1.8 million deaths, accounting for 18.0% of all cancer-related mortality. 1 The burden of lung cancer constantly ranks first among all malignant cancers worldwide. 2 Surgical resection is the gold-standard treatment method for patients with early-stage lung cancer.3,4 Readmissions after surgical procedures have become an increasingly important indicator for healthcare utilization and surgical quality. Reducing hospital readmission has been considered an important strategy to improve patient care and reduce healthcare expenditures. 5 At present, risk factors for readmission after pulmonary resection in patients with lung cancer are still not fully elucidated, and related studies have shown inconclusive results.6–8 For instance, unlike previous studies, Uchida et al 8 indicated that air leakage prevention during initial surgery is crucial to reduce the risk of hospital readmission. In contrast to previous studies, Quero-Valenzuela et al 7 showed that no correlation was found between the type of resection and readmission. To date, no systemic review has comprehensively evaluated the risk factors for readmission after pulmonary resection in patients with lung cancer. In this paper we analyze, synthesize the existing literature, clarify the risk factors for readmission and providing evidence for the prevention of readmission after surgical resection in patients with lung cancer.
Methods
This study was performed according to the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines and registered with INPLASY (https://inplasy.com/). The INPLASY registration number is INPLASY2022100049.
Search Strategy
We systematically conducted a search of the following databases: PubMed, Web of Science, the Cochrane library, CNKI, and Wanfang. The databases were searched for articles published in English from the date of establishment of each database up to May 10, 2022. The key words, including “lung cancer or lung carcinoma”, and “thoracic surgery” or “pulmonary resection” or “lung resection”, and “readmission” or “rehospitalization”, and “predictor” or “risk factor” were searched in the above databases. The reference lists of the compiled articles were manually searched for additional potentially relevant studies.
Inclusion and Exclusion Criteria
Included articles needed to meet the following criteria: (I) the full article could be retrieved and had sufficient data for extraction; (II) the study focused on risk factors for readmission after pulmonary resection for lung cancer; and (III) patients were readmitted to the same institution. Studies were excluded if: (I) they were abstracts, letters, reviews, or case reports; (II) patients were readmitted to the emergency department or there was early return to the clinic; and (III) study contained repeated data or did not report the outcomes of interest.
Data Extraction
Two authors independently extracted the details of the included studies, including the name of the first author, publication year, study size, country, surgical approach, and quality score using the Newcastle–Ottawa Quality Assessment Scale (NOS). If there was any disagreement, it was resolved through mutual consultation, discussion, and consensus with a third review author. Since this was a meta-analysis of previous studies, no ethical approval was required. The patients from the selected studies were divided into the readmission group and non-readmission group. The literature screening and data extraction protocol are shown in Figure 1. All analyses were based on the previously published studies, thus no ethical approval and patient consent are required.

Flowchart for identification of studies in the meta-analysis.
Quality Assessment and Risk of Bias
Quality was assessed using the NOS, and involved the selection of the study groups, evaluation of intercomparability between the groups, and measurement of outcomes, with a maximum score of 9 points; studies with ≥6 points were considered to be of relatively higher quality. 9
Statistical Analysis
Statistical analysis was carried out using STATA SE12.0 (Stata Corp.) software. Odds ratio (OR) was adopted as the effect quantity index, and standardized mean difference (SMD) was used as the effect index for continuous variables. Heterogeneity was examined using Cochran's Q (χ2) test and quantified by the I2 statistic. If the I2 > 50%, stratified analysis or random-effect should be used. Otherwise, a fixed-effect model (the Mantel Haenszel method) was adopted. 10 The weight given to each study is chosen to be inverse of the variance of the effect estimate. Due to some studies using the median and interquartile range (IQR) value for reporting the age, operative time and length of day (length of stay [LOS]), we adopted the mathematical method used by Wan et al 11 to estimate the mean value and standard deviation from the sample size, median, range and/or IQR. Every index effect was expressed with a 95% confidence interval (CI). Metaregression was employed to explore the potential source of heterogeneity. Sensitivity analyses were performed to assess the reliability and stability of the results. Subgroup analysis was adopted to explore the sources of heterogeneity. The power of each study included in this meta-analysis was calculated with Gpower software 3.1. 12 A 2-tailed P value of ≤.05 was considered statistically significant.
Results
Literature Search Results
A total of 859 potential articles were initially identified. After eliminating 251 duplicates, the titles and abstracts of the remaining 608 articles were screened, and 458 irrelevant articles were removed. Subsequently, the full text of the remaining articles was read, and studies that did not meet the requirements were excluded according to the inclusion and exclusion criteria. The screening process is shown in Figure 1. Finally, 11 articles were included in our study,4,6–8,13–19 involving a total of 386 012 participants. Of the 386 012 patients, 26 465 underwent readmission, while 359 547 did not undergo readmission. The NOS score of the included articles was ≥6 points, indicating that the quality of these articles met the study requirements. The basic characteristics of the included studies are shown in Table 1. Nine of these articles were retrospective studies, the others were prospective studies. Data source of these articles were National cancer database, Nationwide readmissions database, hospitals, or thoracic surgical centers. No significant publication bias was found by Begg's and Egger's tests (Table 2). The sensitivity analysis was performed and we found the results were relatively stable (Data was not shown).
Characteristics of Published Studies Included in the Meta-analysis.

Abbreviations: VATs, video-assisted thoracoscopic surgery; NOS, Newcastle-Ottawa Scale; NCDB, the National Cancer Database; NA, not available.
Combined Results of Readmission After Pulmonary Resection in Patients With Lung Cancer.
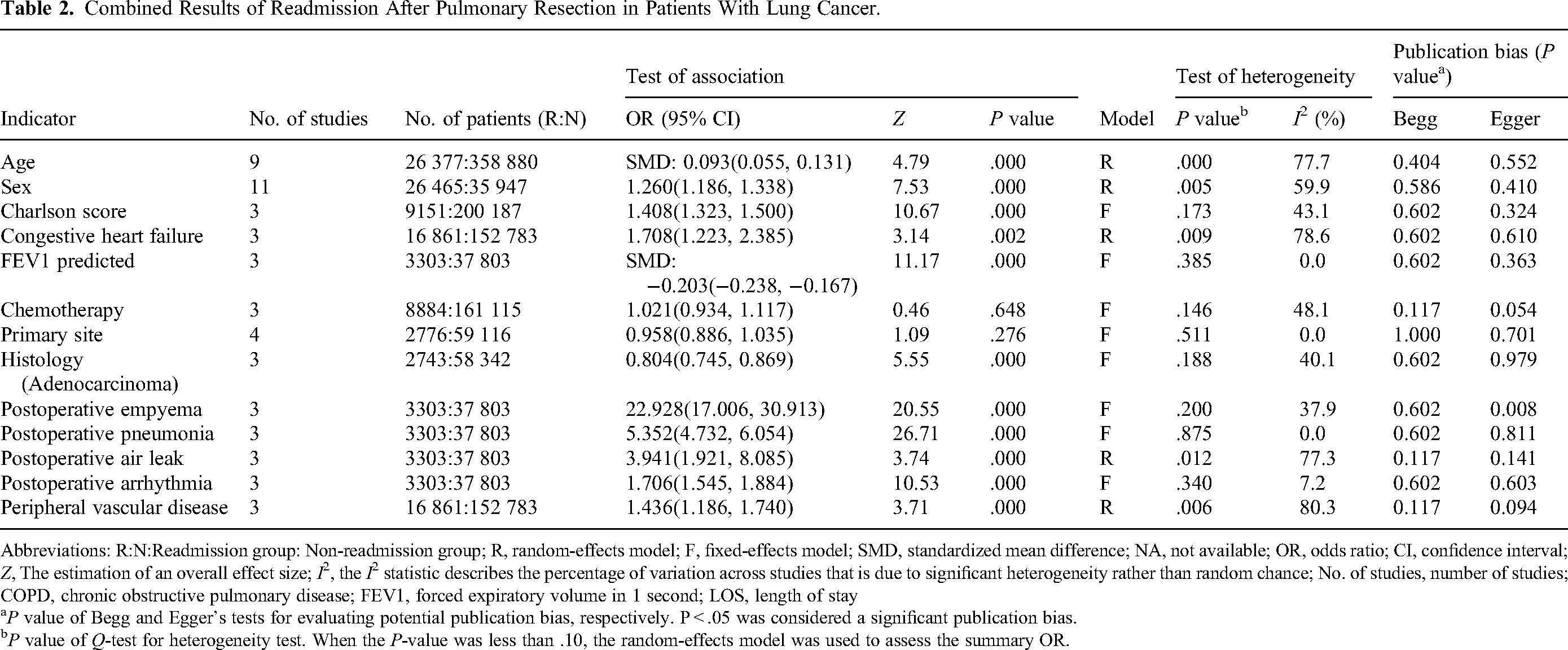
Abbreviations: R:N:Readmission group: Non-readmission group; R, random-effects model; F, fixed-effects model; SMD, standardized mean difference; NA, not available; OR, odds ratio; CI, confidence interval; Z, The estimation of an overall effect size; I2, the I2 statistic describes the percentage of variation across studies that is due to significant heterogeneity rather than random chance; No. of studies, number of studies; COPD, chronic obstructive pulmonary disease; FEV1, forced expiratory volume in 1 second; LOS, length of stay
P value of Begg and Egger’s tests for evaluating potential publication bias, respectively. P < .05 was considered a significant publication bias.
P value of Q-test for heterogeneity test. When the P-value was less than .10, the random-effects model was used to assess the summary OR.
Systematic Review and Meta-analysis Results
We reviewed the literary works, which included in our study and identified whether patients were readmitted to the same institution after pulmonary resection. Three of them reported that patients were readmitted to the same hospitals.6,7,15 The other 2 articles reported that some patients were readmitted to another institution. For instance, 1 study reported that 13 of 30 patients readmitted to a hospital that had not performed the surgery, the other study reported that 12% of related first readmissions were to a different acute care facility than the index admission.17,18 However, we found that 6 of them did not mention whether patients were readmitted in the same hospital or another institution clearly.4,8,13,14,16,19
A pooled analysis of nine (2 of 11 articles did not report original data of age) available studies showed that age was a risk factor for readmission (SMD = 0.093, P < .001), with a heterogeneity (I2 = 77.7%) between the studies (Figure 2, Table 2). The results of metaregression analysis showed that type of surgery (P = .037) and readmission interval (P = .034) might be the source of heterogeneity between studies, while publication year, sample size, and ethnic group were not (all P > .05) (Table 3). No publication bias was found by Begg's test (P = .404) and Egger's test (P = .552). Results of subgroup analyses revealed that hospital readmission was related to Asian (P < .001) and North Amercia (P < .001) population, but not in Europe population (P = .613) (Table 4).

Forest of association between age and readmission after pulmonary resection in patients with lung cancer.
Metaregression Results for Variables.

Subgroup Analysis of the Association Between Indicators and Hospital Readmission After Pulmonary Resection in Patients With Lung Cancer.

Abbreviations: R, random-effects model; SMD, standardized mean difference; NA, not available; OR, odds ratio; CI, confidence interval; Z, The estimation of an overall effect size; I2, the I2 statistic describes the percentage of variation across studies that is due to significant heterogeneity rather than random chance; No. of studies, number of studies
P Value of Begg and Egger's tests for evaluating potential publication bias, respectively. P < .05 was considered a significant publication bias.
P value of Q-test for heterogeneity test. When the P value was less than 0.10, the random-effects model was used to assess the summary OR.
A pooled analysis of 11 available studies suggested that men in the readmission group were more likely to be readmitted than those in the nonreadmission group (OR = 1.260, P < .001) (Figure 3, Table 2). Metaregression analysis showed that publication year, type of surgery, sample size, and readmission interval were not the potential sources of heterogeneity (P > .05). However, it was showed that ethnic group might be the source of heterogeneity between studies (P = .020) (Table 3). No publication bias was found by Begg's test (P = .586) and Egger's test (P = .410). Further subgroup analyses also indicated that hospital readmission increased in Asian (P < .001) and North Amercia (P < .001), but not in Europe (P = .831).
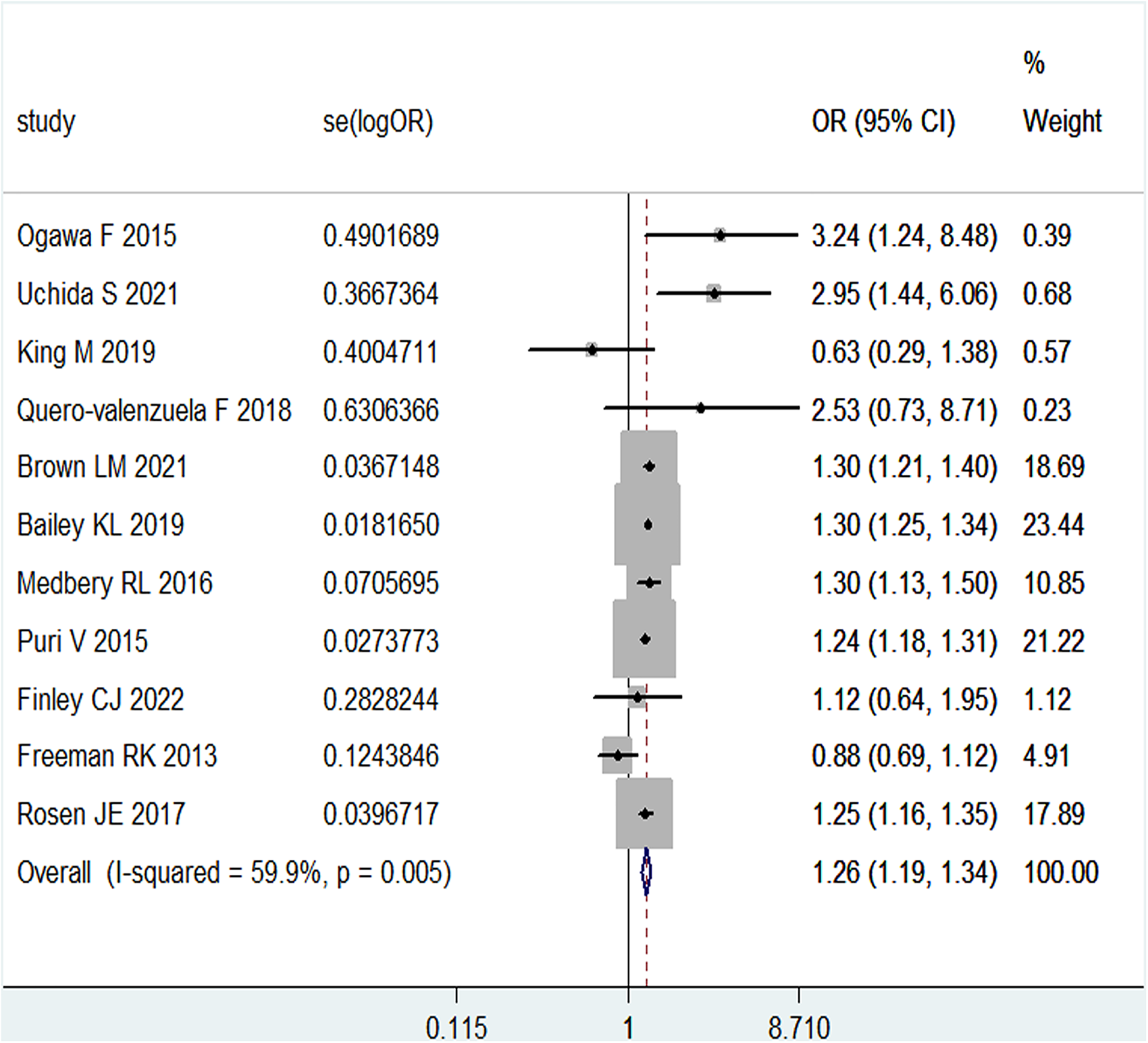
Forest of association between sex and readmission after pulmonary resection in patients with lung cancer.
Five literatures were screened for the association of cigret smoking, diabetes mellitus (DM) with readmission after pulmonary resection for lung cancer. Three of them8,14,16 indicated that smoking and DM were related to hospital readmission, while others did not.4,7 Subgroup analyses indicated that hospital readmission increased in North Amercia (P < .05) and Asian (P < .05), but not in Europe (P > .05) (Tables 2 and 4). In addition, 4 articles that reported4,7,14,15 the relationship between chronic obstructive pulmonary disease (COPD) and hospital readmission were also reviewed, and one large study 1 identified COPD as a factor for hospital readmission. Regarding the LOS, 2 articles were reported13,18 to be associated with hospital readmission, while the other 2 did not.7,15
Five articles reported the association between type of resection (pneumonectomy vs lobectomy) and hospital readmission, and found that one large study 14 considered pneumonectomy as an influence factor for hospital readmission. Two articles contained original data of surgical approach (thoracotomy vs minimally invasive) between readmission group and nonreadmission group, and the results showed that thoracotomy was associated with an increased risk of hospital readmission.14,16 Three articles reported the association between surgical approach (thoracotomy vs video-assisted thoracoscopy) and hospital readmission, and Medbery et al 6 reported that the video-assisted thoracoscopic surgery (VATs) was associated with a 40% increased likelihood of readmission; Quero-Valenzuela et al 7 reported that no significant differences were observed in relation to the surgical approach used, while Bailey et al 14 reported that readmission rate was higher in thoracotomy than VATs.
According to the meta-analysis, congestive heart failure (OR = 1.708), forced expiratory volume in 1 second (FEV1) predicted (SMD = −0.203) and Charlson score (SMD = 1.408) were also regarded as influencing factors for readmission. No publication bias was found by Begg's test (P = .602) and Egger's test (P = .303). However, hypertension was not (P > .05) (Table 2).
We also found that histology (OR = 0.804) was an influencing factor for readmission. Squamous cell carcinoma (36.42% vs 32.20%) and large cell carcinoma (4.56% vs 4.00%) accounted for a higher ratio in the readmission group than that of nonreadmission group, whereas the ratio adenocarcinoma was lower in the readmission group (53.48% vs 58.88%).
As shown in Table 2, patients with postoperative empyema (OR = 22.928), postoperative pneumonia (OR = 5.352), postoperative air leak (OR = 3.941), and postoperative arrhythmia (OR = 1.706) had higher odds of hospital readmission (Table 2).
Discussion
Data regarding the risk factors for readmissions following surgical resection of lung cancer were inconclusive. To our knowledge, this systematic review is the first attempt to explore and synthesize the available literature on risk factors for readmission after pulmonary resection in patients with lung cancer. Our study aimed to identify preoperative, perioperative, and postoperative risk factors for readmission in lung cancer patients. Postoperative readmissions are considered both an indicator of healthcare quality as well as a financial factor impacting hospital reimbursement. 6
This study showed that advancing age and male sex were associated with increased postoperative readmission in lung cancer patients who had undergone pulmonary surgery. With an increase in age, a parallel increase in comorbidities was observed, with nearly 70% of the elderly population having 2 or more comorbidities, while 14% of them were likely to have 6 or more chronic conditions. 20 In terms of the impact of sex on readmission after pulmonary resection, the results were mixed, with some studies showing no relationship with sex,21,22 while other studies reported an increased risk among men of unplanned readmission among men.13,23 Potential explanations for these differences might be related to tumor biology, including diverse genetic pathways and response rates to systemic therapy, different levels of social support, residual confounding, or possibly even a combination of multiple factors. 24
Among preoperative comorbidities, congestive heart failure and FEV1 predicted were associated with readmission in our study. There is evidence showing that preoperative comorbidities were associated not only with the development of postoperative complications but also with the risk of readmission.22,25 Medbery et al 6 reported that readmitted patients had more underlying medical comorbidities, combined with a higher proportion of the Charlson/Deyo score and had a longer median hospital LOS. In addition, a low FEV1 preoperatively was also reportedly associated with a higher risk of unplanned readmission. This is to be expected because it reflects the postoperative pulmonary status of the patients. 21
According to a recent study by Bailey et al 14 included in this review, COPD and history of smoking were factors influencing hospital readmission after pulmonary resection. COPD was regarded as a heterogeneous disease, COPD and smoking were previously reported as independent risk factors for developing postoperative pulmonary complications (PPCs) 26 ; patients diagnosed with COPD have an increased risk of developing both pneumonia after surgery. It has also been demonstrated that PPCs were up to 5 times more prevalent in current smokers when compared to never smokers. The key underlying mechanisms are likely to be related to the impairing effect of smoking on the mucociliary escalator and on the antimicrobial and proinflammatory functions of the alveolar macrophages, which further decrease further during anesthesia and surgery.26,27
Recently, increasing attention was being focused on readmission of patients with DM, and readmission was reported 17% more likely among patients with DM compared to those without DM. 28 This was similar to the result included in our study.8,16 Hospital readmission among patients with DM posed a large burden on healthcare systems and personal expenditure. A better understanding of these comorbidities might lead to lowering the risk of hospital readmission.
Furthermore, our meta-analysis revealed that histology was associated with postoperative readmission. It was shown that adenocarcinoma of the lung accounted for the high ratio of identified tumor tissue in the non-readmission group, whereas the ratio of high-grade malignancy that was not adenocarcinoma was higher in the readmission group of lung patients.15,19
A large study conducted by the Washington University School of Medicine 13 revealed that readmitted patients were more likely to have a longer LOS, and LOS was independently associated with readmission. This finding was in line with those of previously published studies.18,29 The readmission group might require procedures that are more extensive because of the more advanced clinical stage of the disease; moreover, readmitted patients may experience greater comorbidity, thus lead to a significantly higher preoperative mean Zubrod score than the other patients.15,18
Pneumonectomy was a high-risk procedure, combined with more common postoperative complications and related to unanticipated readmissions. 13 Puri et al 13 reported that the type of resection (pneumonectomy) was associated with hospital readmission after pulmonary resection, which was consistent with previous report. 30 However, this result was not confirmed by other smaller studies included in our study. Larger sample studies still need further establish a correlation between type of resection and hospital readmission.
Moreover, when compared with minimally invasive surgery, thoracotomy was considered to be a relatively large operation, which may lead to bleeding, pneumothorax and other complications, and the risk of it might be higher than minimally invasive surgery. Bailey et al 14 reported that VATs remained a significant variable predicting higher readmission rates (vs thoracotomy), they postulated that patients undergoing VATs are likely to be older and sicker than those undergoing thoracotomy. It was likely that individuals who underwent VATs may be adapted to enhanced recovery protocol, thus go through speed-up recovery and discharge from hospital. It might be speculated that patients were discharged too early after VATs, thus leading to an increased risk of hospital readmission. However, Quero-Valenznela et al 7 did not verify this result. Due to the limited number of studies available, further additional studies are warranted to verify the association.
As a large proportion of patients, particularly in large cities where there were multiple hospitals within an urban area, were readmitted to other hospitals. We reviewed the studies included in our study, and found that 3 of them were readmitted to the same hospitals, 2 of them were readmitted to other hospitals, while 6 of them did not mention it clearly, thus the impact of readmission occurring at another institution could not be adequately assessed.4,6–8,13–19
The prevention of postoperative complications was crucial for reducing the risk of readmission in patients undergoing pulmonary resection. Our results showed that postoperative outcomes, such as empyema, atelectasis, pneumonia, air leak, and arrhythmia were associated with hospital readmission. Prolonged air leakage can cause intrathoracic infection, which can rapidly lead to empyema that necessitates readmission even if the air leakage has stopped and the patient is discharged. Empyema was also reportedly the leading cause of unexpected readmission after pulmonary resection. 8 The identification of these risk factors can help in preventing readmissions that are caused by reversible factors such as postoperative air leaks and atelectasis. 7 For instance, improve preoperative patient healthy lifestyle education, adopt a more proactive smoking-cessation program before pulmonary resection; preoperative assessment of pulmonary function, and treatment for pneumonia with intravenous antibiotics. Take more careful postoperative discharge planning, and visit an outpatient clinic earlier after discharge for follow-up examinations, especially for high-risk patients with many baseline risk factors, and thus to decrease unexpected readmission.
Strengths and Limitations
The main strength of this study is that it is the first and largest sample size of systematic review and meta-analysis evaluating the risk factors for readmission after pulmonary resection in patients with lung cancer. The study was conducted in accordance with the PRISMA guideline and data on several outcomes were reviewed. The present study might be the best available evidence to identify preoperative, perioperative, and postoperative predictors of hospital readmission after pulmonary resection in lung cancer patients.
However, some limitations of this study should be noted. First, observational studies might be prone to publication bias, even though no obvious evidence of such bias was found by Egger's and Begg's tests. Second, most of the literatures included did not mention whether patients were readmitted in the same hospital or another institution, and the impact of readmission occurring at different institutions could not be adequately assessed. Third, due to a paucity of data in the literature available, multivariable analysis was not able to further affirm that comorbidities have an effect that is not just due to their correlation with age. Furthermore, although our large sample size allows us to identify subtle differences, this study might be dominated by a single large sample of study, which did not control for the important potential confounders, and the conclusions of this study were for the majority based on single studies. Thus, the result might be subject to bias as a result of the inaccurate magnitude of association reported in the original studies. Finally, the number of studies included in this meta-analysis was limited. The power of each study ranged from 0.68 to 1, except for 1 literature work with a low power of 0.44. Thus, the results of individual studies on the effects of predictors analyzed in our study should be interpreted with caution.
Conclusions
In conclusion, this study identified preoperative comorbidities, perioperative characteristics, and postoperative outcomes as the potential risk factors for readmission after pulmonary resection in patients with lung cancer. An improved understanding of the risk factors for readmission after pulmonary resection may be beneficial for implementing relevant preventative interventions and alleviating the burden of readmissions. In the future, more well-designed studies are warranted to verify these results.
Footnotes
Abbreviations
Authors’ Note
The systematic review was not subject to ethical review. Systematic review registration: INPLASY registration number: INPLASY2022100049.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Jiangxi Provincial Science and Technology Department Key Research and Development Project (No. 20203BBGL73160), Natural Science Foundation of China (No. 81960620), Chinese Foundation for Hepatitis Prevention and Control (LZGC2022-06), Jiangxi Provincial Natural Science Foundation Project (No. 20171BAB215052), Health Commission of Jiangxi Province (No. 20172004 and No. 202130976).
Correction (January 2023):
Article updated online to correct Xuli Yang and Yan Xu's affiliations.