
Abstract
Introduction
Lung cancer is one of the malignant tumors with the highest morbidity and mortality globally, seriously endangering human life and health. 1 Non-small cell lung cancer (NSCLC) is the most common pathological type of lung cancer, with its most common type, being lung adenocarcinoma and lung squamous cell carcinoma (LSCC). 2 Radical resection of lung cancer is the best treatment option for patients with stage I, II, and partially resectable stage III NSCLC. 3 However, despite the continuous improvement of comprehensive treatment based on surgery, perioperative management, and postoperative adjuvant therapy in recent years, the clinical prognosis of NSCLC is still worrying. The recurrence rate of stage I to III NSCLC patients is 17% to 73%.4,5 Therefore, it is imperative to identify influential prognostic factors in postoperative NSCLC patients.
The literature suggests that the inflammatory response and nutritional status are closely related to tumor proliferation, invasion, and metastasis and positively affect cancer progression. 6 At present, a variety of inflammatory and nutritional indicators have been used to predict the prognosis of NSCLC, such as Prognostic Nutritional Index (PNI), neutrophil-to-lymphocyte ratio (NLR), systemic inflammation index (SIS), lymphocyte-to-monocyte ratio (LMR), and controlled nutritional status score (CONUT).3,7–9 In addition, multiple indicators such as gender, smoking status, and age are also associated with the prognosis of NSCLC patients. 10 Due to its advantages of minor trauma, convenience, rapidity, and reproducibility, the biomarkers related to inflammation and nutrition in the blood have gradually become the focus of cancer research. The Naples Prognostic Score (NPS) score is a new inflammation-nutrition scoring system, calculated from the patient's preoperative serum albumin (ALB), total cholesterol (TC), NLR, and LMR. It reflects the patient's systemic inflammatory response and nutritional status. 11
We conducted this study to explore the clinical significance of NPS in the prognosis of NSCLC patients, especially those with stage III NSCLC, through the Kaplan-Meier method and multivariate Cox regression analysis. The NPS was also compared with CONUT and SIS through the area under curve (AUC) to evaluate their accuracy in predicting long-term survival after surgery.
Methods
Patients
This study retrospectively analyzed 319 NSCLC patients who underwent surgery from March 2017 to February 2019. All the participants were followed-up by outpatient visits, and the follow-up ended in February 2021 for this cohort. All the enrolled patients met the following criteria: (1) Receiving surgery and pathologically diagnosed as NSCLC; (2) Not receiving radiotherapy and chemotherapy before surgery; (3) Sufficient follow-up data. Exclusion criteria: (1) History of other malignant diseases in the past; (2) Inflammatory diseases or surgery within one month; (3) Recent use of steroid drugs; (4) Patients with hematological diseases, infectious diseases, or severe immune system diseases. The Medical Ethics Committee of our institute approved this study (No.2022059). Due to the retrospective design of this study, we waived patients’ informed consent. We have de-identified all patient details. We ensure the confidentiality of experimental data and all procedures comply with the Declaration of Helsinki. The reporting of this study conforms to STROBE guidelines. 12
Data Collection
We extracted patient preoperative information from medical record system, who underwent radical resection of lung cancer, including smoking history, gender, body mass index (BMI), histological type, age at diagnosis, clinical stage, blood inflammation-nutrition indicators (TC, neutrophil, lymphocyte, ALB, absolute monocyte count), postoperative adjuvant therapy (including chemotherapy, targeted and immunotherapy). Naples Prognostic Score is calculated from the patient's preoperative ALB, TC, NLR, and LMR levels, according to previously reported methods by Galizia et al 11 . NLR ≤ 2.96, LMR ≥ 4.44, ALB ≥ 40 g/L and TC > 180 mg/dL, score 0; scored 1 for NLR > 2.96, LMR < 4.44, ALB < 40 g/L and TC ≤ 180 mg/dL. Naples Prognostic Score is the combination of each of the above scores. We divided patients into 3 groups according to the NPS score, patients with score 0 were divided into group 0, patients with scores 1 and 2 were divided into group 1, and patients with scores 3 and 4 were divided into group 2. PNI = 10 × albumin (g/dL) + 5 × lymphocyte count (109/L), NLR = neutrophil/lymphocyte, LMR = lymphocyte/monocyte. The endpoints of this study are overall survival (OS) and recurrence-free survival (RFS). Overall survival refers to the time from the day of surgery to death from any cause. Recurrence-free survival is the time from the day of surgery to tumor recurrence.
Statistics
The descriptive statistical analysis described the association between NPS and clinicopathological features in NSCLC patients. The optimal cutoff value for PNI was calculated using X-tile software version 3.61. We used the “survival” and “survminer” packages of R software to draw survival curves and analyze the difference in survival curves, used the “time ROC” package to draw time-dependent ROC (t-ROC) curves, and calculate the AUC when the follow-up time was 3 years. To examine the predictive ability of NPS score in OS and RFS prognosis in NSCLC patients, we utilized Statistical Product Service Solutions (SPSS) to create univariate and multivariate Cox proportional hazards models. The R software version is 4.1.2, and the SPSS software version is 26.0. A P-value <.05 was considered statistically significant.
Results
Baseline Characteristics
We retrospectively analyzed the patient information of 319 individuals with NSCLC diagnosed by pathology from March 2017 to February 2019. Table 1 shows the clinicopathological characteristics of the clinical research subjects. Female patients account for more than half, 162 patients and 157 male patients. Smoking patients accounted for 29.47% of the total populationand smoking patients in the group 2 accounted for more than 60% of the total population in group 2. There are 92 patients with recurrence and 74 patients with death. The median age to diagnosis for all patients is 61 years (interquartile range, IQR: 13 years), and the median follow-up time is 32 months (IQR: 12 months). Compare to patients in group 0, the median OS of group 2 patients seems to be much reduced (group 2 vs group 0, 28 months vs 35 months).
Association of Naples Prognostic Score and Clinicopathological Characteristics in 319 Patients With Resected NSCLC.

Abbreviations: BMI, body mass index; LAD, lung adenocarcinoma; LSCC, lung squamous cell carcinoma; Tis, tumor in situ; PNI, Prognostic Nutritional Index; ALB, serum albumin; TC, total cholesterol; NLR, neutrophil-to-lymphocyte ratio; LMR, lymphocyte-to-monocyte ratio; NSCLC, non-small cell lung cancer; OS, overall survival.
Survival Analysis
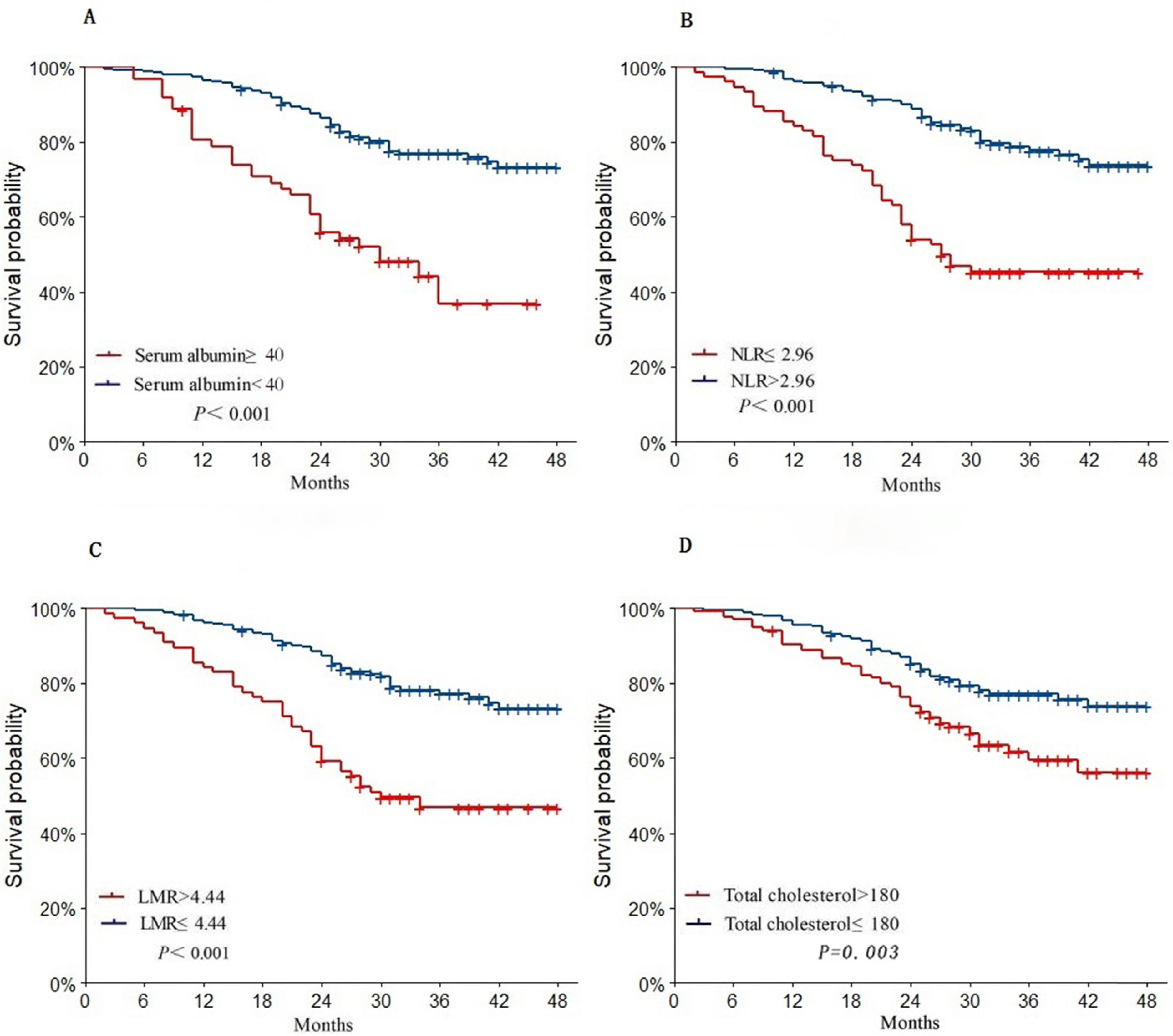
Figure 1 summarizes the Kaplan-Meier survival curves for RFS and OS. Between different groups, there are considerable disparities in OS and RFS (all P < .001), and the median survival time of the higher group and the lower group are significantly prolonged (OS, group 0 vs group 1 vs group 2, 35 months vs 31 months vs 28 months; RFS, group 0 vs group 1 vs group 2, 34 months vs 30 months vs 23.5 months). ALB, TC, NLR, and LMR are analyzed using Kaplan-Meier survival curves, and the results are shown in Figure 2. In terms of OS, patients with LMR ≤ 4.44, ALB < 40 g/L, and NLR > 2.96 have significantly shorter OS (all P < .001), but the survival curves grouped by TC showed no statistical difference(P = .082). In terms of RFS, as shown in Figure 3, patients with TC >180 mg/dL, ALB ≥ 40 g/L, LMR > 4.44, and NLR ≤ 2.96 have significantly prolonged RFS (all P < .05).

(A) Recurrence-free survival (RFS) curves for patients in different groups. (B) Overall survival (OS) curves for patients in different groups.

Overall survival curves for serum albumin (ALB) (A), neutrophil-to-lymphocyte ratio (NLR) (B), lymphocyte-to-monocyte ratio (LMR) (C), and total cholesterol (TC) (D).
Recurrence-free survival curves for serum albumin (ALB) (A), neutrophil-to-lymphocyte ratio (NLR) (B), lymphocyte-to-monocyte ratio (LMR) (C), and total cholesterol (TC) (D).
The use of NPS in patients with resectable stage III NSCLC is still not tested. The data of this study includes a total of 37 patients with stage III, including 6 patients in group 0, 18 patients in group 1, and 13 patients in group 2. Among the total number of the 2 groups, stage III patients accounted for 35.14% of the current group, the highest proportion (Tis vs stage I vs II vs III vs, 1.12% vs 8.86% vs 28.57% vs 35.14%). The Kaplan-Meier curves of OS and RFS are shown in Figure 4. The survival time of the high group was significantly shorter than that of the low group (both P < .05), and the univariate and multivariate Cox analysis shows that stage III and NPS are independent risk factors. Naples Prognostic Score can be utilized as a predictive indicator of stage III patients following surgery.

Kaplan-Meier survival curves of overall survival (A) and recurrence-free survival (B) for the Naples Prognostic Score (NPS) group in stage III non-small cell lung cancer (NSCLC).
Univariate Cox Analysis of OS and RFS
Univariate Cox analysis prompted in Table 2, shows that, stage (Tis vs stage I or stage II or stage III, P = .051, P < .001, P < .001), female(P < .001), age > 61 years (P = .043), smoking (P < .001), LSCC (P < .001), treatment (P < .001), PNI < 49.75 (P < .001), ALB < 40 g/L (P < .001), NLR > 2.96 (P < .001), LMR < 4.44 (P < .001), and NPS (group 0 vs group 1 or group 2, P = .001, P < .001) are intimately correlated with a poor OS rate. Female (P < .001), age > 61years (P = .017), smoking (P < .001), LSCC (P < .001), treatment (P < .001), PNI < 49.75 (P < .001), ALB < 40 g/L (P < .001), TC ≤ 180 (P = .004), NLR > 2.96 (P < .001), LMR < 4.44 (P < .001), stage (Tis vs stage I or stage II or stage III P = .006, P < .001, P < .001), and NPS (group 0 vs group 1 or group 2, P < .001, P < .001) are significantly correlated with RFS (Table 2). Univariate analysis P < .05 for TC and OS, BMI, and RFS. The indicators with P < .10 are added to the multivariate Cox analysis to avoid missing some important covariates.
Univariate Cox Proportional Hazards Model Results of OS and RFS.
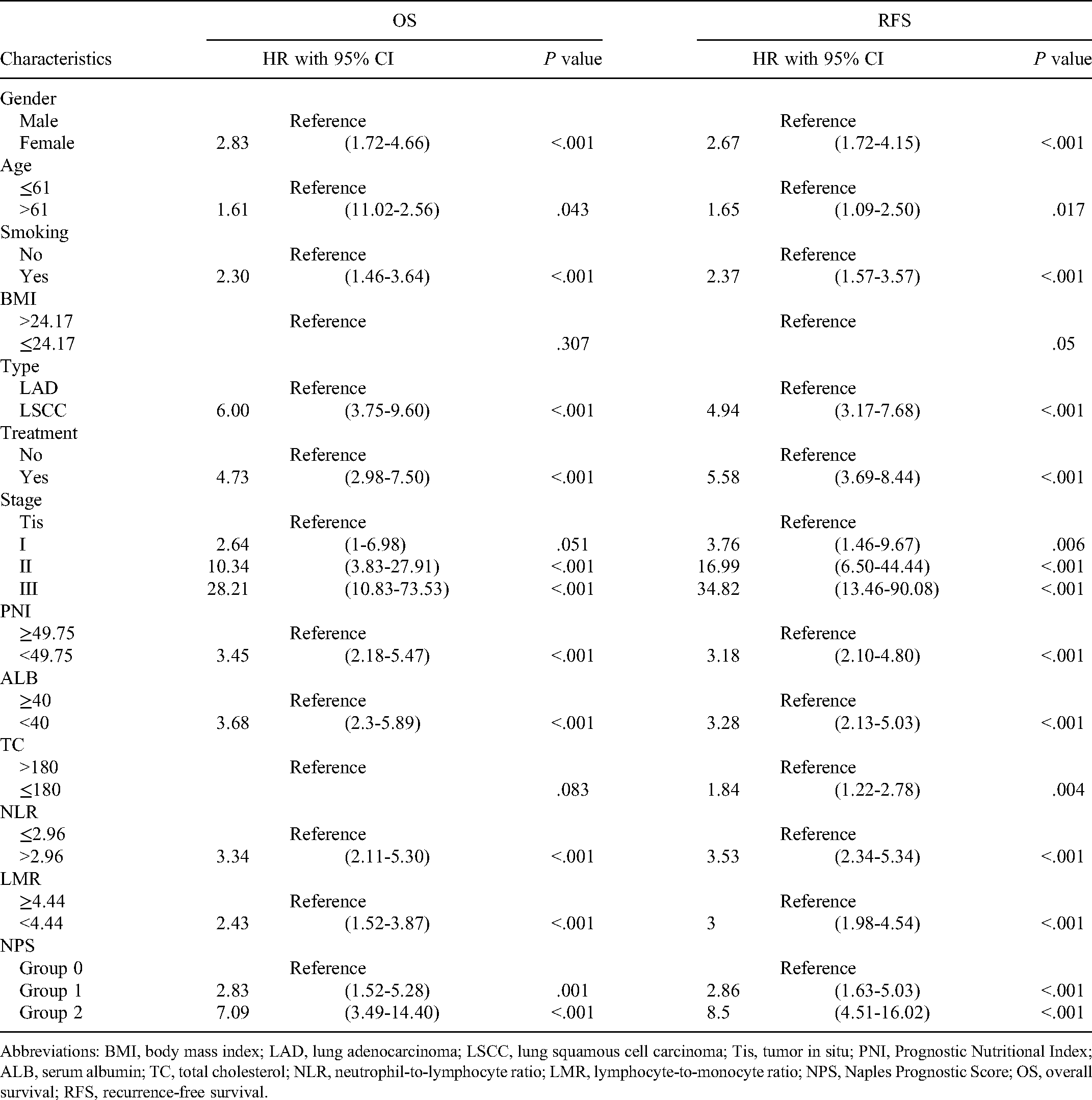
Abbreviations: BMI, body mass index; LAD, lung adenocarcinoma; LSCC, lung squamous cell carcinoma; Tis, tumor in situ; PNI, Prognostic Nutritional Index; ALB, serum albumin; TC, total cholesterol; NLR, neutrophil-to-lymphocyte ratio; LMR, lymphocyte-to-monocyte ratio; NPS, Naples Prognostic Score; OS, overall survival; RFS, recurrence-free survival.
Multivariate Cox Analysis of OS and RFS
Through multivariate Cox analysis prompted in Table 3 determines that LSCC (HR = 1.88, 95% CI = 1.07-3.29, P = .028), stage (stage II vs Tis, HR = 7.67, 95% CI = 2.68-21.98, P < .001; Stage III vs Tis, HR = 19.18, 95% CI = 7.03-52.31, P < .001), TC≤180(HR = 0.51, 95% CI = 1.07-3.29, P = .018), NPS (group 1 vs group 0, HR = 3.51, 95% CI = 1.74-7.11, P < .001; group 2 vs group 0, HR = 4.42, 95% CI = 1.77-11.07, P = .002) are found to be a reliable prognostic predictor for OS. NLR > 2.96 (HR = 1.83, 95% CI = 1.08-3.08, P = .024), stage (stage I vs Tis, HR = 3.79, 95% CI = 1.47-9.77, P = .006; stage II vs Tis, HR = 17.48, 95% CI = 6.57-46.52, P < .001; stage III vs Tis, HR = 28.49, 95% CI = 10.80-75.12, P < .001), NPS (group 1 vs group 0, HR = 2.57, 95% CI = 1.42-4.70, P = .002; group 2 vs group 0, HR = 2.51, 95% CI = 1.15-5.50, P = .021) are sharply associated with the prognosis of RFS and can independently predict the prognosis of RFS.
Multivariate Cox Proportional Hazards Model Results of OS and RFS.
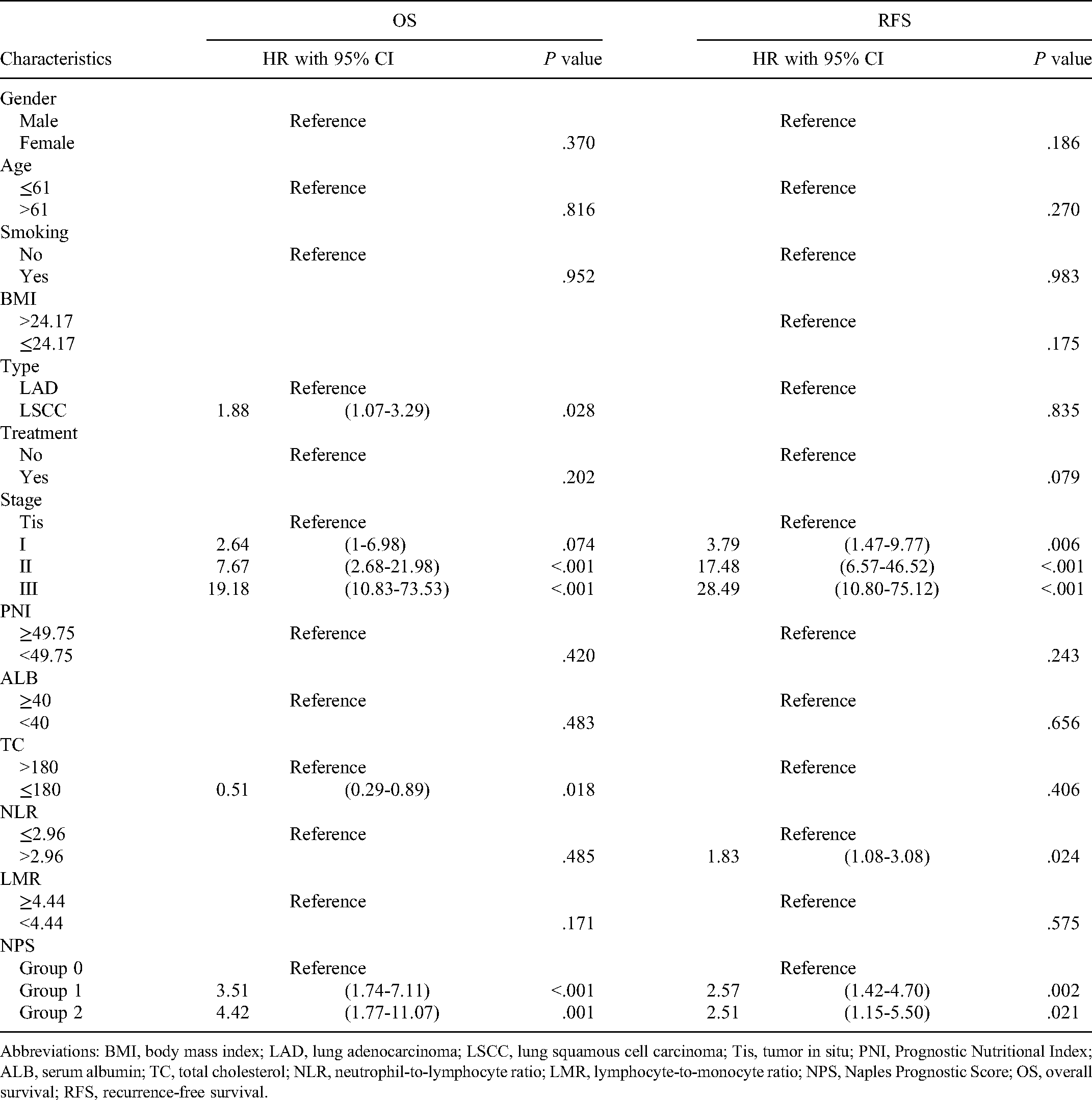
Abbreviations: BMI, body mass index; LAD, lung adenocarcinoma; LSCC, lung squamous cell carcinoma; Tis, tumor in situ; PNI, Prognostic Nutritional Index; ALB, serum albumin; TC, total cholesterol; NLR, neutrophil-to-lymphocyte ratio; LMR, lymphocyte-to-monocyte ratio; NPS, Naples Prognostic Score; OS, overall survival; RFS, recurrence-free survival.
Prognostic Value of NPS
In this study, we compared the predictive ability of NPS with CONUT and SIS by t-ROC. Compared with CONUT and SIS, NPS has a higher AUC numerical value, Figure 5. When the follow-up time was 3 years, the AUC values of NPS, CONUT, and SIS of OS are 0.70, 0.58, and 0.68, respectively. The AUC values of NPS, CONUT, and SIS of RFS are 0.73, 0.60, and 0.69. According to the result, NPS has higher accuracy than CONUT and SIS in predicting the prognosis of NSCLC patients.

The time-dependent area under curve (AUC) analyses of prediction models. (A) Overall survival, (B) recurrence-free survival.
Discussion
This study confirmed that the preoperative NPS of NSCLC patients was related to gender, age, smoking, postoperative treatment, and histological type. In NSCLC, NPS can be utilized as an individual variable to predict postoperative OS and RFS, and it has higher accuracy than other scoring systems (CONUT and SIS).
Inflammatory cells are an integral component of the tumor microenvironment (TME) and play a vital role in tumor appreciation, progression, and drug resistance. 13 Naples Prognostic Score includes NLR, LMR, ALB, and TC, as a new inflammation-nutrition scoring system, reflecting the systemic inflammatory response and nutritional status. The mechanisms that may affect the prognosis are as follows: Neutrophils, as the most important mediators in the immune system, play a critical role in the innate immune defense and are the first line of defense in the body. 14 Under homeostatic conditions, only 1% to 2% of neutrophils are usually present in the blood, but cancer patients increase neutrophils in the blood and tissues by adding transforming growth factor-β.9,15 In the TME of NSCLC, neutrophils constitute approximately 20% of the CD45+ population. 16 Neutrophils increase the hazard of cancer progression by regulating the activity of matrix metalloproteinases, degrading elastin, fibrinogen, and collagen, promoting neovascularization, and creating a microenvironment suitable for tumor survival.13,17 In addition, monocytes and differentiated tumor-associated macrophages degrade the extracellular matrix, thereby attracting more monocytes and macrophages, inducing immunosuppression and tumor angiogenesis, and increasing the probability of tumor metastasis. 8
Huang et al 18 reported that the pretreatment lymphocyte percentage could independently predict the prognosis of patients with NSCLC, which has an excellent clinical application value. As one of the crucial components of the immune system, lymphocytes are principal in immune surveillance and mediating cancer immune destruction and can secrete a series of cytokines to inhibit tumor growth.19,20 Neutrophils secreted factors such as IL-10 can inhibit cell proliferation, inhibit the function of cytotoxic cells, cause the decrease of lymphocytes, and weaken the immune response. 21 Therefore, NLR and LMR can be used as biomarkers for the prognosis of lung cancer patients, and NSCLC patients with elevated NLR and decreased LMR have a poor prognosis.
Naples Prognostic Score also covers ALB and TC. ALB concentration plays a vital role in various scoring systems as a marker of patient nutritional and inflammatory status, and low albumin is a consequence of malnutrition. ALB is a harmful acute-phase protein, and inflammation inhibits albumin synthesis, resulting in lower albumin levels. 22 It not only reflects the nutritional reserve of the patient but also reflects the severity of the systemic inflammatory response. 23 Multiple studies have suggested that low concentrations of TC are linked to a worse prognosis in lung cancer patients.24,25 Our findings showed similar results, with multivariate cox regression analysis showing TC (OS, HR = 0.51, 95% CI = 1.07-3.29, P = .018). The possible reason is that cholesterol is an essential component of cell membranes, and low cholesterol levels reduce the fluidity of cell membranes and impair the ability of cell surface receptors to transmit transmembrane signals. 11 Studies have shown that the lung may be a part of cholesterol metabolism with a specific metabolic mechanism. A high cholesterol diet has a protective effect on mouse-induced lung cancer, but further experimental studies are needed to clarify the specificity of lung cholesterol metabolism. 26 Serum albumin and TC, as important indicators to measure human nutritional status, are closely related to the degree of malnutrition. The decline in their levels indicates a poor prognosis for patients.
As a new scoring system, NPS integrates a variety of biomarkers, covering more comprehensive nutritional and inflammatory immune indicators, showing better predictive efficacy. Previous studies by Li et al 27 demonstrated that NPS, as a risk stratification tool, can guide treatment and improve outcomes in lobectomy patients with NSCLC. Guo et al 28 showed that NPS could be used as the basis for individualized risk classification of patients with unresectable stage III NSCLC. The above studies confirmed NPS as a prognostic indicator in patients with NSCLC, helping treatment decisions. Contrary to Li's study, we included patients with resectable stage III and Tis stages and independently analyzed patients with resectable stage III NSCLC. Apart from this, our study endpoints were different from Li's study, which showed that NPS could predict patient's RFS. The findings suggest that NPS may predict long-term survival outcomes in patients with stage III resectable NSCLC cancer. And compared to other scoring systems, NPS has higher accuracy.
Our study also has certain flaws. First, this study is a single-center retrospective study and the relatively small flow may have contributed to selection bias. Second, although some critical factors were associated with OS and RFS in NPS and NSCLC patients, some potential confounding factors such as economic conditions may be missing. Finally, the determination of relevant indicators in the blood may be affected by various states, etc, reducing its accuracy.
Conclusion
Our study provided that preoperative NPS showed a significant prognostic role in NSCLC following video-assisted thoracic surgery, high group NPS predicted worse OS and RFS. Naples Prognostic Score is a good prognostic factor for patients with stage III NSCLC following surgery. But, future multicenter and prospective studies are needed to prospectively validate our results.
Footnotes
Abbreviations
Authors’ Note
Ethical approval to report this study was obtained from Heibei General Hospital (Approval ID: 2022059). Due to the retrospective design of this study, we waived patients’ informed consent.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.