
Abstract
Keywords
Introduction
Major salivary gland carcinomas (MSGCs) are a diverse and highly heterogeneous group of rare malignancies. 1 The major salivary gland squamous cell carcinoma (MSSCC) is a rare histological type of MSGCs, accounting for about 0.9% to 4.7%. 2 Surgery is the primary treatment method for resectable MSSCC. Postoperative radiotherapy can improve the local control rate and disease-free survival, but whether it can prolong the survival time is still unclear.3,4 MSSCC is prone to local recurrence, and the 5-year overall survival (OS) rate is less than 50% even for patients treated with surgery. 5 Owing to its rarity, most studies on MSSCC are small sample reports or MSSCC combined with other types of SGCs are analyzed as a whole.6,7 Up to now, the clinicopathological characteristics, treatment modalities, survival outcomes, and potential prognosis factors of MSSCC have not been fully elucidated.
The American Joint Committee on Cancer (AJCC) tumor–node–metastasis (TNM) stage is an important reference factor in the treatment selection of MSSCC, but it still has limitations in clinical application, especially in head and neck carcinoma. 8 Lymph node metastasis is considered as one of the most important prognostic factors for salivary gland carcinoma.9–11 Accumulating evidence suggests that lymph node number (LNN) and lymph node ratio (LNR) are associated with clinical outcomes in these patients.12–14 Nonetheless, no study has yet analyzed the prognostic value of LNN and LNR in MSSCC.
Thus, we performed a retrospective analysis of a large-scale population from the Surveillance, Epidemiology, and End Results (SEER) database to investigate the clinical value of LNN and LNR in MSSCC after resection. Furthermore, we established a satisfactory nomogram prediction model and stratified patients into different risk groups, which has greater clinical application value.
Methods
Data Collection
The demographic and clinicopathological data of patients initially diagnosed with MSSCC between January 1, 2004, and December 31, 2018, were retrieved from the SEER database. As the data for this study were derived from a public database, there was no need for the additional ethical application.
All patients had a clear pathological diagnosis, AJCC TNM stage, and detailed surgical information, including surgical method, tumor size, number of lymph nodes examined intraoperatively, and number of positive lymph nodes. The main inclusion criteria were as follows: (1) pathologically diagnosed as MSSCC; (2) age at diagnosis was over 18 years old; (3) first malignancy; (4) surgery performed; (5) definite T, N, M stage; (6) the number of examined lymph node (ELN)≥1. Patients with distant metastasis and unknown clinical features were excluded from our study. Besides, patients who did not receive surgical resection, and those who only received adjuvant chemotherapy were also excluded.
Variables Definition
LNR was defined as the ratio of positive lymph nodes to the total number of lymph nodes removed. OS was the interval from the diagnosis to the death caused by any reasons or the last follow-up. Disease-specific survival (DSS) was calculated as the time from the initial diagnosis to the date of cancer-specific death.
Statistical Analysis
Statistical analyses were performed using the SPSS software (version 23.0; IBM) and R software (version 4.1.1) and GraphPad Prism (version 9.0; GraphPad Software Inc). Appropriate thresholds were determined by minimum P value and maximum χ2 tests using X-tile software. The influence of each variable on OS and DSS was analyzed using the Kaplan-Meier method, and significance was evaluated by log-rank test. Univariate and multivariate Cox regression analyses were performed to assess the effect of each variable on prognosis, and nomogram models were established. The discriminative ability of the nomogram model was evaluated by Concordance index (C-index) and area under curve (AUC), and the Calibration plot was used to further evaluate the calibration ability between actual results and predicted probabilities. P < .05 was considered statistically significant.
Results
Basic Characteristics and Cutoff Values
A total of 815 patients were eligible for the present study. The basic characteristics are seen in Table 1. A total of 411 patients (50.4%) were diagnosed and treated from 2004 to 2011, and the remaining patients (49.6%) were admitted from 2012 to 2018. In the whole cohort, the predominant patients were man (79.5%) and white race (n = 421). The median age of patients was 70 years old. More than 90% of cases occurred in the parotid gland, followed by the submandibular gland (8.5%). The pathological grades of most cases were moderately differentiated (29.9%) and poorly differentiated (49.6%). The median tumor size was 3 cm, and there were 334 cases (41.0%) of T1 to 2 stage and 481 cases (59.0%) of T3 to 4 stage. The number of patients with positive lymph nodes slightly outnumbered those with negative lymph nodes (55.0% vs 45.0%). Most patients (78.5%) were at stage III to IV, suggesting that MSSCC is an aggressive malignancy of the salivary gland.
Basic Characteristics.
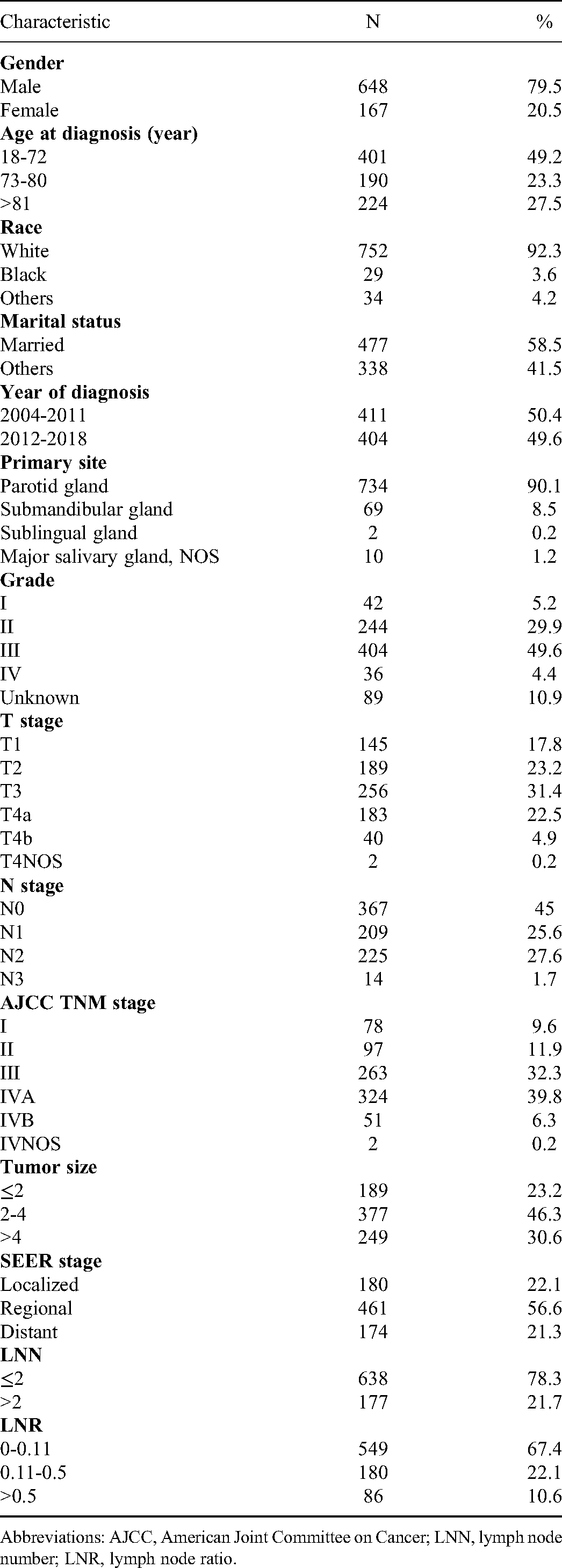
Abbreviations: AJCC, American Joint Committee on Cancer; LNN, lymph node number; LNR, lymph node ratio.
The median ELN and LNN were 16 (range: 1-90) and 1 (range: 0-90), respectively. As shown in the results of Kaplan-Meier curves and log-rank tests, the subgroup differences were most significant using these optimal truncation values identified from the X-tile program (Supplementary Figure 1). The cutoff values of age were 72 and 80 (n = 401 vs 190 vs 224, χ2: 119.0250, relative risk: 1.00/1.42/1.90, P < .001). The cutoff value of LNN was 2 (n = 638 vs 177, χ2: 27.8064, relative risk: 1.00/1.34, P < .001). Besides, the cutoff value of LNR were 0.11 and 0.5 (n = 549 vs 180, χ2: 21.8657, relative risk: 1.00/1.18/1.39, P < .05).
Treatment Patterns
In terms of treatment modalities, 567 patients underwent adjuvant radiotherapy after surgery, and 196 patients underwent adjuvant chemotherapy. More specifically, as shown in Supplementary Figure 2, the majority of patients (47.2%) were treated with surgery plus adjuvant radiotherapy, while 241 patients (29.6%) received surgery alone and 189 patients (23.2%) received surgery plus adjuvant chemoradiotherapy. Among 175 patients with early-stage, only 11 (6.3%) patients received chemoradiotherapy after surgery, and most patients were treated with surgery with or without radiotherapy. Of those with stage III to IV, 170 (26.6%) patients underwent surgery alone; 292 (45.6%) patients were offered surgery and adjuvant radiotherapy, 178 (27.8%) patients received surgery and adjuvant chemoradiotherapy. Additionally, Supplementary Figure 2 also showed treatment trends of patients with MSSCC in the SEER databases from 2004 to 2018.
Survival Outcomes
The median follow-up period of the entire cohort was 80.0 months. Among these patients, 224 patients died from MSSCC, and 211 patients died from other causes, including diseases of heart, cerebrovascular diseases, lung and bronchial diseases, and diabetes mellitus. The median OS was 59.0 months, and the median DSS was not reached (Supplementary Figure 3). The overall 1-, 3-, 5-, and 10-year OS rates of patients with MSSCC were 82.9%, 61.1%, 49.5%, and 32.0%, respectively. The DSS rate of 1-, 3-, 5-, and 10-year were 87.5%, 72.9%, 67.7%, and 62.7%, respectively. In addition, the Kaplan-Meier curves of OS and DSS among the different AJCC TNM stage and SEER combined stage are also presented in Supplementary Figure 3.
Prognostic Factors
The results of univariate and multiple Cox regression models for OS and DSS are presented in Tables 2 and 3. Univariate analysis revealed that older age, advanced T stage, large tumor size, and more LNN, higher LNR, and no radiotherapy were associated with decreased OS (all P < .05), whereas gender, race, marital status, year of diagnosis, primary site, histologic grade, N stage, and chemotherapy were not prognostic factors. In multiple Cox regression models, age at diagnosis, T stage, tumor size, LNN, LNR, and radiotherapy were independent prognostic factors for OS (all P < .05) (Table 2).
Univariate and Multivariate Survival Analysis on OS for Patients With MSSCC After Surgery.

Abbreviations: OS, overall survival; MSSCC, squamous cell carcinoma of the major salivary gland; HR, hazard ratio; CI, confidence interval; LNN, lymph node number; LNR, lymph node ratio.
Univariate and Multivariate Survival Analysis on DSS for Patients With MSSCC After Surgery.

Abbreviations: DSS, disease-specific survival; MSSCC, squamous cell carcinoma of the major salivary gland; HR, hazard ratio; CI, confidence interval; LNN, lymph node number; LNR, lymph node ratio.
Furthermore, the results showed that patients older than 72 years had shorter DSS than patients younger than 72 years. Compared with those with lesions in the parotid gland, patients with lesions in the submandibular gland had a 1.5-fold increased risk of death (P = .049). Besides, patients with moderately differentiated (P = .012) and poorly differentiated (P = .026) exhibited approximately a 3-fold increased risk of death compared with those with well-differentiated. In addition, DSS of patients with MSSCC after surgery also showed statistically significant differences among different T stage, N stage, tumor size, LNN, and LNR groups. However, chemotherapy had no significant effect on prognosis, suggesting that patients did not seem to benefit from additional chemotherapy. In addition, there was no statistically significant difference in DSS among patients in different years of diagnosis and treatment. Further, Cox regression analysis also revealed that age, T stage, tumor size, LNN, LNR, and radiotherapy were independently prognostic for DSS (all P < .05) (Table 3).
Nomogram Construction and Validation
Based on the results of the above multivariate Cox regression analysis, we integrated these independent prognostic factors to establish our nomogram model to predict OS and DSS of patients with MSSCC. By calculating total scores, the prognosis of patients with different clinicopathological features can be predicted. As shown in Figure 1, the corresponding score of each variable can be confirmed by the vertical line between the variable and the point axis. Putting all the points together and placing them in the total subscale of our individualized nomogram, the estimated probabilities for 1-, 3-, and 5-year OS and DSS could be obtained.

Nomogram model of OS (A) and DSS (B) in patients with MSSCC after surgery. Abbreviations: OS, overall survival; DSS, disease-specific survival; MSSCC, squamous cell carcinoma of the major salivary gland.
Subsequently, the established nomogram model was evaluated by using several methods, including the C-index, AUC values, and calibration plot. The results showed that the C-index of the nomogram for OS was higher than that of the AJCC stage system (0.71 vs 0.59) and SEER combined stage (0.71 vs 0.55). Similar results were obtained for the C-index of the DSS nomogram model. The C-index of the nomogram of DSS is also than that of the AJCC stage system (0.71 vs 0.63) and SEER combined stage (0.71 vs 0.59).
For the 1-, 3-, and 5-year OS rate, the AUC values indicated better discriminative ability for our nomogram model (1-, 3-, and 5-year: 0.759, 0.754, and 0.768) than for the traditional AJCC TNM stage system (1-year: 0.637, 3-year: 0.614, and 5-year: 0.597) and the SEER combined stage (1-year: 0.579, 3-year: 0.573, and 5-year: 0.559) (Figure 2). Similarly, the AUC values of our nomogram model at 1-, 3-, and 5-year DSS were 0.769, 0.734, and 0.739, respectively (Figure 2), which were also higher than those of traditional AJCC TNM stage system and SEER combined stage. Furthermore, calibration plot for 1-, 3-, and 5-year OS and DSS prediction based on the nomogram model indicated a favorable consistency between the actual and predicted outcomes. The details are seen in Figure 3.
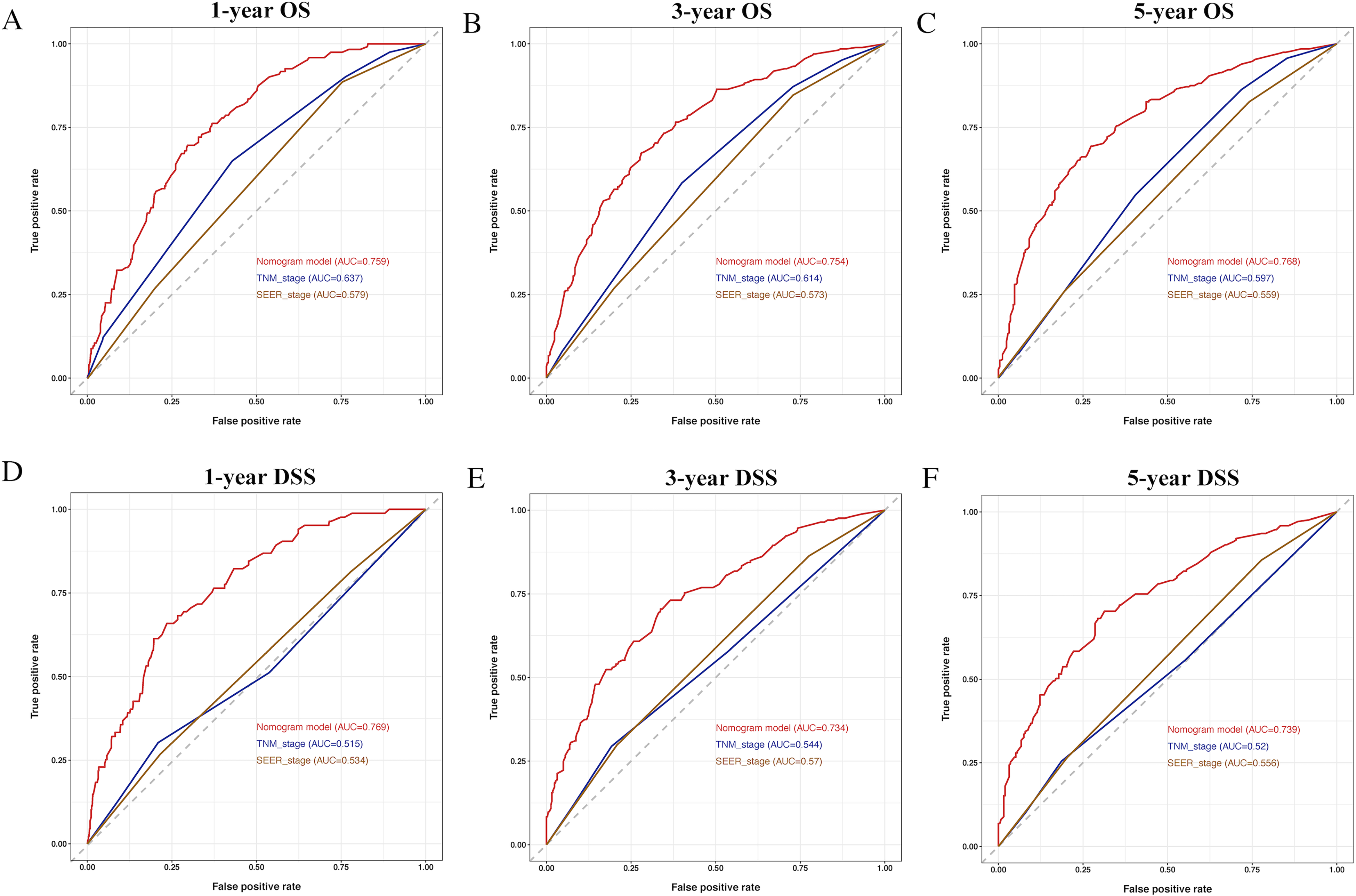
The ROC curve for 1-, 3-, and 5-year OS and DSS. (A-C) Comparison of the ROC curves of the nomogram, the TNM stage, SEER stage for 1-year OS (A), 3-year OS (B), and 5-year OS (C). D-F. Comparison of the ROC curves of the nomogram, the TNM stage, SEER stage for 1-year DSS (D), 3-year DSS (E), and 5-year DSS (F). Abbreviations: OS, overall survival; DSS, disease-specific survival; ROC, receiver operator characteristic; TNM, tumor–node–metastasis; SEER, Surveillance, Epidemiology, and End Results.

The calibration plots for 1-, 3-, and 5-year OS and DSS. (A) 1-year calibration plot for OS nomogram; (B) 3-year calibration plot for OS nomogram; (C) 5-year calibration plot for OS nomogram; (D) 1-year calibration plot for DSS nomogram; (E) 3-year calibration plot for DSS nomogram; (F) 5-year calibration plot for DSS nomogram. Abbreviations: OS, overall survival; DSS, disease-specific survival.
Clinical Application of Nomogram Risk Stratification
The total score of the patients was calculated based on the established nomogram model and then divided into 3 groups. For OS, patients were divided into 3 groups including low risk (n = 293, 0-86.63), moderate risk (n = 375, 87.70-165.90), and high risk (n = 147, 166.88-285.25) groups (χ2: 207.1315, relative risk: 1.00/2.16/2.82). With respect to DSS, the 3 cohorts were as follows: (1) low risk: n = 415, 0-170.11; (2) moderate risk: n = 307, 170.38-280.51; (3) high risk n = 93, 281.50-433.93 (χ2: 128.7367, relative risk: 1.00/2.06/3.66). As shown in Figure 4, the 5-year OS rate of patients in the low-, moderate-, and high-risk groups were 75.7%, 42.1%, and 15.5%, respectively. Besides, the 5-year DSS in the low-risk subgroup versus that in the moderate-risk subgroup versus that in the high-risk subgroup was 81.9% versus 59.6% versus 26.0%, respectively. Significant statistical differences in OS and DSS of patients among different groups were observed, indicating that our prediction model had a good grading ability (P < .001).

The OS (A) and DSS (B) of patients among the low-, moderate-, and high-risk groups. Abbreviations: OS, overall survival; DSS, disease-specific survival.
Discussion
To the best of our knowledge, our study is the first to explore risk models based on the individual characteristics of patients with MSSCC after surgery. The nomogram models for predicting survival can be used to calculate the survival probability of each patient through an intuitive graph and divide them into different risk groups according to the score, so as to better stratify the prognosis of these patients and have important clinical guiding value.
Consistent with the existing literature,15,16 most of the patients are men over 60 years old, and the parotid gland is the main site of the disease. For these elderly patients, clinicians should pay more attention to the comorbidities and quality of life of the patients during the treatment process. As was shown in our results, MSSCC is a clinically aggressive malignant tumor with a high incidence of tumors at the advanced stage with lymph node involvement. It has been reported that lymph node–related parameters are important for the prognosis of head and neck tumors. 17 Therefore, we identified optimal cutoffs for LNN and LNR and further explored their clinical significance in MSSCC. The results indicated that the prognostic value of LNN and LNR was better than N stage. After adjusting for other variables, LNN and LNR were still closely associated with OS and DSS, suggesting that they were more reliable and accurate in guiding the prognosis of patients with MSSCC. A growing amount of evidence supported the clinical significance of LNR in SGCs, 12 oral squamous cell carcinoma (OSCC),18,19 and other non-head and neck carcinoma.20,21 It has been reported that positive LNN and LNR provided the most accurate prediction of disease-free survival (DFS) and OS for OSCC patients treated with surgery ± adjuvant therapy. 22 In Park et al study, patients with carcinoma of unknown primary (CUP) undergoing surgery and adjuvant radiotherapy were reviewed and the prognostic value of nodal parameters in CUP was further explored. 23 Univariate analysis showed that LNR > 0.14 were associated with poor outcomes in DFS and OS, and in multivariate analysis, LNR was further identified as a significant predictor for DFS. 23 This study provides additional evidence that LNR is superior to conventional N stage in cervical lymph node metastases. Of note, another study noted that the prognostic significance of LNR varied by anatomical subsite, which may be partly related to the significant differences in local recurrence rates and distant metastasis rates among different anatomical subsites in head and neck tumors. 24 In the study by Suzuki et al, 25 minor SGCs patients with high-risk LNR had worse clinical outcomes than patients with low-risk LNR, suggesting that LNR may be a negative predictor of survival. Elhusseiny et al 26 also revealed that patients with LNR > 0.33 belonged to the high-risk subgroup and associated with poorer survival in major SGCs. Likewise, Meyer et al demonstrated the great impact of LNR on the prognosis of patients with parotid gland carcinoma. 27 In their analysis, 128 postoperative patients were evaluated and a median LNR of 0.11 was determined. Patients with an LNR of 0.001 to 0.1 had a significantly lower 5-year OS rate compared with patients with an LNR of 0 (5-year OS rate: 88% vs 77%). In addition, a statistically significant difference between the survival curves was also observed in patients with LNR 0.11 to 0.5 and LNR > 0.5 (5-year OS rate: 50% vs 37%). 27 After adjusting for other variables, LNR remained the only independent predictive factor affecting OS, indicating that the use of LNR could reliably stratify clinical outcome. 27 As anatomical subsites play a crucial role in its impact on clinical outcomes, we performed the current analysis to explore the value of LNR in MSSCC. ELN may vary with the extent of neck dissection, but insufficient neck dissection may result in incomplete treatment or even worse outcomes; however, the LNR takes into account the total LNN resected, which measures tumor burden adjusted for lymph node yield. This may be one of the reasons for the excellent performance of LNR in our study, which was evident in both survival analysis and multivariate Cox model. Based on the above, LNR could be considered for inclusion in the current staging system and as a factor in risk assessment and treatment decisions. Further evaluation of real-world data with large samples is necessary to further improve its clinical utility.
Histological subtypes of SGCs are not considered in all current treatment guidelines, and the more than 20 subtypes of SGCs are not distinguished from each other in terms of recommended treatment, except for adenoid cystic carcinoma. 28 Surgery is the most definite and effective treatment for resectable SGC including MSSCC. 29 Nevertheless, local recurrence rates remain high even after patients undergo surgery, with a median survival of less than 15 months.30–33 Therefore, improving the postoperative local control rate is the key to prolonging the survival of patients. Postoperative management strategies for MSSCC are still controversial.32,34,35 It has been reported that the 5-year disease-free survival rate of patients receiving surgery combined with radiotherapy is better than that of patients treated with surgery alone. 33 Several studies have also indicated that surgery plus adjuvant radiotherapy was related to improved OS compared with radiotherapy alone, but not when compared to treatment with surgery alone.3,36 Radiotherapy can improve local control rates to some extent, but it can also increase treatment-related adverse events, including functional damage of skin, mucosa, microvascular, and muscle fibrosis. 37 MSSCC is common in elderly patients,36,38 and most of them may have poor performance status and comorbidities. These adverse events can have a negative impact on quality of life and even shorten survival time. Strikingly, in our study, surgery combined with adjuvant radiotherapy is the primary treatment method for MSSCC regardless of early or advanced stage. Postoperative radiotherapy was shown to significantly improve OS and DSS in patients with this rare malignancy. The presentation of this conclusion may provide new support for the development of treatment guidelines for this uncommon malignancy.
Taken together, our study identified that age, T stage, tumor size, LNN, and LNR can affect the OS and DSS of patients with MSSCC after resection. Based on these independent prognostic factors, we first constructed a satisfactory OS and DSS nomogram model for evaluating the clinical outcome of postoperative MSSCC patients. Compared with the AJCC TNM stage and SEER stage, our individual nomogram model was more accurate in predicting prognosis, as confirmed by higher C-index, better AUC values, and more consistent calibration plots. Importantly, our nomogram model can significantly stratify patient survival outcomes according to low-, moderate-, and high-risk groups. As the risk grade increased, OS and DSS of these patients decreased significantly. Given the outstanding predictive ability of our nomogram, we further confirmed the importance and great clinical application value of these models.
There are several limitations in the present study. Some clinically relevant variables and details of adjuvant therapy were not available from SEER database, such as patient's own performance status and comorbidities, as well as adjuvant therapy regimen and dose. Thus, the results should be interpreted with some caution. Although we established nomogram model based on the classical clinicopathologic feature to predict the survival rate of patients with MSSCC after surgery, molecular biological prognostic indicators and external validation are still needed to further improve its reliability. It should be emphasized that some prospective large-scale clinical studies are required before applying nomograms in clinical practice. Regardless, our established prognostic model and risk stratification still provide clinicians with additional information beyond the existing criteria that can be used to characterize this rare malignancy.
Conclusions
LNN and LNR exhibited favorable efficacy in predicting the prognostic value of MSSCC. The nomogram integrated clinicopathological parameters including LNN, LNR, and treatment method and showed higher accuracy than TNM stage and SEER stage in predicting OS and DSS.
Supplemental Material
sj-tif-1-tct-10.1177_15330338221117405 - Supplemental material for Nomogram-Based Prediction of Overall and Disease-Specific Survival in Patients With Postoperative Major Salivary Gland Squamous Cell Carcinoma
Supplemental material, sj-tif-1-tct-10.1177_15330338221117405 for Nomogram-Based Prediction of Overall and Disease-Specific Survival in Patients With Postoperative Major Salivary Gland Squamous Cell Carcinoma by Lixi Li, Di Zhang and Fei Ma in Technology in Cancer Research & Treatment
Supplemental Material
sj-tif-2-tct-10.1177_15330338221117405 - Supplemental material for Nomogram-Based Prediction of Overall and Disease-Specific Survival in Patients With Postoperative Major Salivary Gland Squamous Cell Carcinoma
Supplemental material, sj-tif-2-tct-10.1177_15330338221117405 for Nomogram-Based Prediction of Overall and Disease-Specific Survival in Patients With Postoperative Major Salivary Gland Squamous Cell Carcinoma by Lixi Li, Di Zhang and Fei Ma in Technology in Cancer Research & Treatment
Supplemental Material
sj-tif-3-tct-10.1177_15330338221117405 - Supplemental material for Nomogram-Based Prediction of Overall and Disease-Specific Survival in Patients With Postoperative Major Salivary Gland Squamous Cell Carcinoma
Supplemental material, sj-tif-3-tct-10.1177_15330338221117405 for Nomogram-Based Prediction of Overall and Disease-Specific Survival in Patients With Postoperative Major Salivary Gland Squamous Cell Carcinoma by Lixi Li, Di Zhang and Fei Ma in Technology in Cancer Research & Treatment
Supplemental Material
sj-docx-4-tct-10.1177_15330338221117405 - Supplemental material for Nomogram-Based Prediction of Overall and Disease-Specific Survival in Patients With Postoperative Major Salivary Gland Squamous Cell Carcinoma
Supplemental material, sj-docx-4-tct-10.1177_15330338221117405 for Nomogram-Based Prediction of Overall and Disease-Specific Survival in Patients With Postoperative Major Salivary Gland Squamous Cell Carcinoma by Lixi Li, Di Zhang and Fei Ma in Technology in Cancer Research & Treatment
Footnotes
Abbreviations
Authors’ Note
Di Zhang and Lixi Li contributed equally to this work. We used data from public databases, and approval of ethics committee was not required as it did not include human or animal trial. All data can be retrieved from public SEER database.
Acknowledgements
The authors acknowledge the efforts of the SEER database in the creation of the SEER database and thank all the patients analyzed in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.