
Abstract
Keywords
Introduction
Esophageal cancer is one of the most common malignant tumors in the world with a high mortality rate. 1 According to histopathological classification, esophageal cancer mainly includes squamous cell carcinoma (ESCC) and adenocarcinoma, and more than 90% of patients are squamous cell carcinoma in Asia countries, such as China. In recent years, despite great progress in the diagnosis and treatment of esophageal cancer, the overall survival (OS) of ESCC remains poor, with a 5-year survival of 15% to 20%. 2 The main reason for the failure of esophageal cancer treatment is recurrence and distant metastasis. 3 Therefore, more efforts still need to make in the diagnosis and treatment to improve the prognosis of ESCC.
In clinical practice, prediction of the prognosis with ESCC is usually based on tumor differentiation, lymph node (LN) metastasis, and Tumor–Node–Metastasis (TNM) stage. 4 However, 10%-20% of esophageal cancers were found to have insufficient staging after surgical resection, and their biological behavior was more aggressive than predicted based on clinical staging alone. 5 Like other solid tumors, esophageal cancer is inseparable from the nutritional support provided by new blood vessels in the process of growth and evolution. Abundant neovascularization also provides a pathway for tumor cells to enter the blood or lymphatic circulation for transport to metastatic sites. Metastasis through the vasculature is the main mode of esophageal cancer recurrence. Lymphovascular invasion (LVI) is a histopathological condition usually defined as the presence of tumor cells within lymphatics or blood vessels.6,7 The formation of LVI is a multifactor and multistage complex pathophysiological process. When tumor cells break through the basement membrane and invade the surroundings, they may invade small blood vessels and lymphatic vessels, especially in the process of tumor growth. Tumor microangiogenesis provides a good anatomical basis for tumor cells to enter the blood circulation and form LVI. 8 LVI plays an important role in tumor recurrence and LN metastasis, and increases the risk of micrometastasis. 9 Previous study has reported that LVI could predict insufficient preoperative staging and LN metastasis. 10 In addition, LVI is also a risk factor for poor prognosis and LN metastasis in patients with esophageal cancer. Patients with LVI have poor OS and progression-free survival.11,12 Therefore, early identification of patients with high risk of recurrence is crucial for the development of individualized treatment approaches in ESCC. 13
Currently, LVI is only based on postoperative pathological diagnosis, and preoperative prediction of LVI status is extremely difficult.14,15 Computed tomography (CT) remains the initial imaging method for clinical staging of esophageal cancer, evaluating local spread into adjacent structures and the presence of distant metastases. The sensitivity of conventional CT protocols in localizing esophageal cancer, especially early-stage cancer, is not satisfactory, perhaps because conventional CT cannot afford optimal conspicuity of esophageal cancers against the normal esophageal wall. Some studies found that contrast-enhanced CT (CECT) is helpful for the detection of lesions and can show the relationship between lesions and surrounding tissue structures, which is of great value for the diagnosis and staging of esophageal cancer. 16 Several studies have shown that preoperative CECT may provide a noninvasive method to predict LVI in gastric and rectal cancer by measuring quantitative parameters.14,17–19 We hypothesize that the risk of LVI can be predicted based on the CECT-related parameters of the arterial phase in ESCC. Therefore, the aim of this study was to evaluate the feasibility for predicting LVI in ESCC by quantitative parameters of CECT.
Materials and Methods
Patient Population
A total of 228 patients with ESCC (151 males and 77 females, age range: 41-84 years; median age: 67 years, interquartile range: 62-72 years) were admitted to our institution between June 2017 and December 2020. Inclusion criteria: (a) Patients undergoing radical resection of esophageal cancer; (b) Preoperative contrast-enhanced CT was performed; and (c) Histologically confirmed esophageal squamous cell carcinoma. Exclusion criteria: (a) Absence of preoperative clinicopathological data and contrast-enhanced CT in this hospital; (b) The pathological diagnosis was esophageal adenocarcinoma, small cell neuroendocrine carcinoma, or other pathological tumors; (c) Poor visualization of the tumor due to insufficient distension or peristaltic motion of the esophagus, limited area to draw regions of interest (ROI) owing to too small tumor size; (d) Preoperative radiotherapy, chemotherapy or other treatment; and (e) Multiple esophageal lesions. The reporting of this study conforms to STROBE guidelines. 20
CT Protocol
Among the 228 patients, CT was performed with a dual-source CT scanner (Siemens Somatom Definition). Scanning covered the entire esophagus region during a single breath-hold with the patient supine. Imaging acquisition parameters were as follows:120kVp; 130mAs; rotation time: 0.5s; collimation width: 64 × 1.25mm, pitch: 1.5:1, field of view (FOV): 350 × 350 mm, matrix: 512 × 512; Layer thickness: 5mm, layer spacing: 5mm. The following CECT scans were obtained 25 to 30s (arterial phase), 55 to 60s (venous phase) after an infusion of 1.5mL/kg of iohexol or ioversol contrast material (Hengrui Medicine) at a rate of 2.5 to 3.0 mL/s with an automatic power injector. The original image was uploaded to Syngo CT 2012B image workstation (Siemens) for multiplanar reformation (MPR) and obtained the coronal plane and sagittal plane images.
CT Images Analysis
The CECT images were retrospectively analyzed by 2 senior attending radiologists. The observers were blinded to clinical and pathological data. On CECT images, the tumor tissue showed localized thickening of the esophageal wall or a mass-like appearance with marked enhancement. Localized thickening of the esophageal wall ³ 5 mm was identified as abnormal thickening. 21 Then, to observe and record the following parameters:(a)Tumor location: The upper segment is above the lower edge of the azygos vein arch, the middle segment is between the lower edge of the azygos vein arch and the level of the left lower pulmonary vein, and the lower segment is the left lower pulmonary vein and within 2cm below the gastroesophageal junction; (b)Tumor size: Measure the tumor length, maximum tumor thickness based on CECT (if the lumen is completely occluded, measure 1/2 of the maximum diameter of the tumor in the most significant section of the lesion); (c) tumor-to-normal wall enhancement ratio (TNR): The TNR was calculated by dividing the mean attenuation value of the tumor by that of the normal wall to quantify the degree of difference in contrast enhancement between the tumor and normal wall. The ROIs were placed in areas where tumor enhancement is most pronounced in the arterial phase of the largest cross-section, avoiding vascular structures, ulceration, and necrosis (Figures 1(A and B) and 2(A and B)). (d) Clinical T stage (cT stage) was referred to as the CT staging criteria proposed by Griffin et al 21 The clinical N stage (cN stage) is based on the No. of metastatic LNs in different regions, and the determination of metastatic LNs is based on the shortest diameter of enlarged LNs combined with the LN axial ratio. The long-axis and short-axis diameters of the regional LNs with a short diameter exceeding 3mm were measured and axial ratios were calculated (short-axis/long-axis diameters). For analysis by size, the records sorted by short-axis diameter (1-mm increments, range: 3-10 mm). Receiver operating characteristic (ROC) analysis was performed to obtain an optimal LN axial ratio criterion (axial ratio was calculated by dividing the short diameter by the long diameter). As axial ratio can reflect the shape of the node, LNs with an axial ratio exceeding the cut-off were considered LN metastasis.22,23 The clinical American Joint Committee on Cancer stage (cAJCC stage) were based on the AJCC/International Union Against Cancer (UICC) Eighth Edition Cancer Staging Manual. 24 In addition, the gross tumor volume (GTVs) were manually delineated by 2 radiologists on the 3D Slicer software (version 4.3, http://www.slicer.org) to delineate the visible tumor at each slice, and the GTVs were calculated automatically.

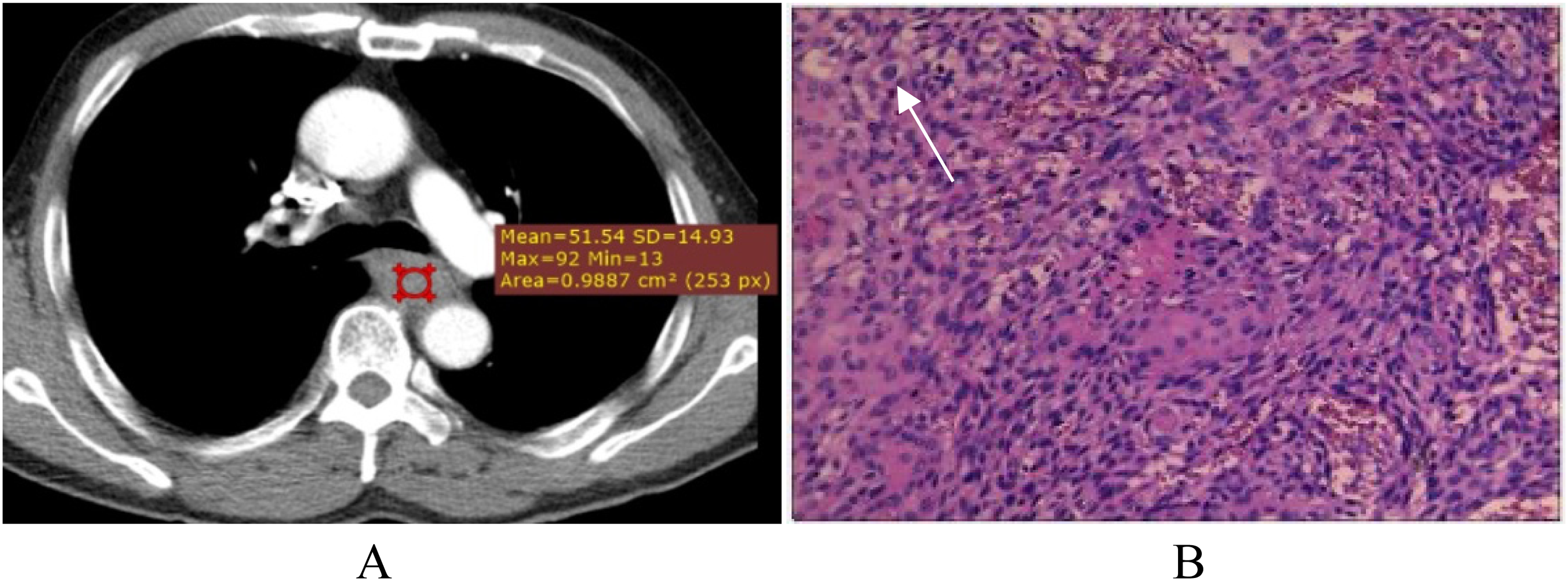
A 63-year-old female with esophageal squamous cell carcinoma (ESCC). (A) Computed tomography (CT) image in the arterial phase. (B) Hematoxylin and eosin (H&E) staining showed lymphovascular invasion (LVI) (white arrows).
A 59-year-old male with esophageal squamous cell carcinoma (ESCC). (A) Computed tomography (CT) image in the arterial phase. (B) Hematoxylin and eosin (H&E) staining showed lymphovascular invasion (LVI) (white arrows).
Pathological Evaluation
Hematoxylin and eosin (H&E) staining and immunohistochemistry (IHC) were performed on the gross specimens resected by the operation, and the pathologists performed examination and analysis. The pathological T stage (pT stage) and pathological N stage (pN stage) were based on the AJCC/UICC Eighth Edition Cancer Staging Manual. 24 LVI was defined as the presence of tumor thrombi within small blood vessels and lymphatic vessels. All of these structures are called LVI because they cannot be distinguished under the microscope on H&E-stained slides. 8
Statistical Analysis
Statistical analyses were performed with SPSS, version 22.0 (IBM), and R software packages, version 3.1.2 (The R Foundation for Statistical Computing, http://www.r-project.org/). The power calculation has been done for the estimation of sample size selected for the study. The intraclass correlation coefficient (ICC) was used to assess the reproducibility of parameter measurements between observers. ICC > 0.70 was considered good agreement. For categorical variables such as gender, age, tumor location, tumor differentiation, pT stage, pN stage, cT stage, cNstage, and cAJCC were analyzed with the chi-square test between the 2 groups. For continuous variables such as tumor length, tumor thickness, GTV, and TNR were expressed as the mean ± standard deviation (M ± SD). The Kolmogorov–Smirnov method was used for the normality test, and the Levene's test was used for the variance homogeneity test. The CECT-derived parameters that conform to normal distribution or homogeneity of variance, the independent sample t-test is used, while for parameters that are not normally distributed or homogeneous for variance, the Mann–Whitney U test is used. The univariate analysis was used to derive independent predictors for LVI, and their combination model was constructed by multivariate logistic regression analysis. In addition, ROC curve analyses were performed to determine the area under the curve (AUC), accuracy (ACC), sensitivity (SEN), specificity (SPE), positive predictive value (PPV), and negative predictive value (NPV). A two-sided P value of <.05 was considered to be statistically significant.
Results
Clinicopathological Characteristics of the Patients
Clinical and pathological data analysis of the 228 enrolled patients is summarized in Table 1. There were 36 patients (15.79%) with LVI and 192 patients (84.21%) without LVI. There were statistically significant differences between the 2 groups in age and pN stage (P < .05). Regarding gender, tumor location, differentiation, and pT stage, there were no statistically significant differences between the 2 groups (P > .05).
Clinical and Pathological Characteristics of the 228 Patients.

Data are number of patients (%) or P value.
Abbreviations: LVI, lymphovascular invasion; pT stage, pathological T stage; pN stage, pathological N stage; pAJCC, pathological AJCC.
Intra-Observer Repeatability of CECT Parameter Measurements
There were no significant differences between the 2 observers in CECT parameter measurements (P = .326-.738). ICC (95% CI) for tumor length, thickness, and TNR varied from .785 (.756-.853) to .874 (.868-.919). All of them were in good agreement.
Univariate and Multivariate Analysis for Clinical and CECT-Derived Parameters
The results of the univariate analysis for clinical and CECT-derived parameters between the 2 groups are presented in Table 2. Univariate analysis of clinical features and CECT-derived parameters revealed that age, TNR, and cN stage were significantly associated with LVI. All 3 risk factors for LVI were taken into a multivariable logistic regression model to identify the independent predictors. The results demonstrated that age (odds ratio [OR]: 5.323, 95% confidence interval [CI]: 2.224-12.743, P<.001), TNR (OR: 5.399, 95% CI: 1.609–18.110, P = .006), and cN stage (cN1: OR: 2.874, 95% CI: 1.182-6.989, P = .02; cN2: OR: 6.876, 95% CI: 2.222-21.277) were identified to be independent predictors for LVI (Figure 3).

The forest plot of the multivariable regression analysis for lymphovascular invasion (LVI).
Univariate Analysis to Identify Significant Factors for LVI in Esophageal Squamous Cell Carcinoma (ESCC).

*Overall P value.
Abbreviations: CI, confidence interval; cN stage, clinical N stage; cT stage, clinical T stage; cAJCC, clinical AJCC stage; GTV, gross tumor volume; NA, not available; OR, odds ratio; TNR, tumor-to-normal wall enhancement ratio.
Diagnostic Performance of Clinical and CECT-Derived Parameters Predictors and Their Combination
The diagnostic performance of age, TNR, cN stage, and their combination are listed in Table 3. Although TNR showed relatively higher sensitivity, the specificity of detection of LVI was relatively lower than that of age, cN stage, and their combination. The combination of age, TNR, and cN stage achieved a relatively higher AUC (0.798), ACC (65.4%), PPV (77.4%), and NPV (71.6%) than those of age, TNR, and cN stage. Delong test shows that the AUC value of the combination was significantly higher than the AUC values of the age, TNR, and cN stage (P = .0001, .0264, and .0001). The ROC analysis of age, TNR, cN stage, and their combination for predicting LVI in ESCC is shown in Figure 4.

ROC curves of age, TNR, cN stage, and their combination for predicting LVI in ESCC. Abbreviations: cN stage; clinical N stage; ESCC, esophageal squamous cell carcinoma; ROC, receiver operating characteristic; LVI, lymphovascular invasion; TNR, tumor-to-normal wall enhancement ratio.
The Diagnostic Performance of age, TNR, cN Stage, and Their Combination.

Abbreviations: ACC, accuracy; AUC, area under the curve; cN stage, clinical N stage; NPV, negative predictive value; PPV, positive predictive value; SEN, sensitivity; SPE, specificity; TNR, tumor-to-normal wall enhancement ratio.
Discussion
As a routine examination, CECT plays an important role in the diagnosis, preoperative clinical staging, and efficacy evaluation of patients with esophageal cancer.21,25–27 This study demonstrated that some quantitative CECT-derived parameters may serve as independent predictors for LVI in ESCC, and that clinical features combined with CECT-derived parameters may improve the predictive power. This novel noninvasive approach is expected to provide risk prediction and decision support in the clinical management of ESCC patients.
At present, the clinicopathological factors used to judge the prognosis of patients with ESCC mainly include the depth of tumor invasion, the degree of differentiation, and regional LN metastasis. Preoperative prediction of LVI status is very important for the development of an active treatment plan for patients. 28 Several studies have incorporated LVI into the TNM staging system for other tumors.29,30 Previous studies have shown that LVI is an independent risk factor for prognosis in ESCC.27,31 Clinically, patients with suspected tumor LVI require more aggressive treatment, such as expansion of surgical scope or preoperative adjuvant therapy. 9
Our study showed that age was an independent predictor of LVI status in patients with ESCC. However, Wang et al believed that there is no correlation between age and LVI status in ESCC. 12 This is inconsistent with the results of our research. The reason may be that there were more older patients in our study and the relatively small sample size of LVI-positive patients, which may bias the study results. Our study also showed that TNR of the arterial phase was an independent predictor for LVI. Komori et al showed that TNR was correlated with tumor angiogenesis and lymphatic vessel invasion, 19 consistent with our results. Previous studies indicated that the vascular endothelial growth factor (VEGF) family induced angiogenesis and lymphangiogenesis actively, 31 and tumor neovascularization was closely related to LVI in esophageal cancer.32,33 Theoretically, the arterial phase, which reflects changes in blood vessels and hemodynamics, may reflect the presence of LVI. 34 This theory can explain our results.
LN metastasis is the most important prognostic factor in esophageal cancer. 35 The LVI plays a vital role in LN metastasis and the spread of cancer, and it is thought to increase the risk of regional micrometastasis spreading. 9 In this study, the multivariate analysis showed that cN stage based on CECT is another predictor for LVI in ESCC. This result suggests that CECT-reported LN status is closely related to LVI in patients with ESCC. According to conventional standards, conventional CT has low sensitivity in detecting LN status. A new diagnostic criteria based on CECT have improved the sensitivity in detecting LN status, making the cN stage based on CECT more in line with clinical practice. 23 Clinically, LVI may be an upgrade factor for cN stage, especially in patients with negative LN metastasis, 11 because it is an important factor affecting their prognosis. Although the cN stage based on CECT as an independent predictor for LVI in this study, CECT-reported LN status alone showed unsatisfactory discrimination (AUC = 0.651). The efficacy of size criteria in the assessment of LVI is still limited.
In our study, although age, TNR, cN stage were independent predictors for LVI, their independent predictive value is limited (AUC: 0.619, 0.664, and 0.651). However, the combination of age, TNR, and cN stage achieved a relatively higher AUC (0.798), ACC (65.4%), PPV (77.4%), and NPV (71.6%) than those of age, TNR, and cN stage. Therefore, we believe that the combination of clinical and CECT-derived parameters may be used as a noninvasive predictor for LVI in patients with ESCC. Of course, our results require further validation of external data, which will also be our next research direction.
Currently, maximum tumor diameters have been considered to be a good indicator for predicting LVI in hepatocellular carcinoma. 36 However, unidirectional measurements are highly variable and unreproducible. Lee et al37 reported that tumor volume measurement could make up for this shortcoming. Our study compared the GTVs between 2 groups with and without LVI in ESCC. The results showed that LVI was not correlated with the size of the tumor volume, and even small tumors had the risk of micrometastasis and recurrence.
Our study has some limitations. First, this study is a single-center retrospective study, and the enrolled cases included only those patients who underwent surgery, which may cause selection bias. Second, this study lacks plain and venous phase scan images, and may lack some more meaningful quantitative parameters. Finally, due to tumor heterogeneity, the radiomics features based on CECT may be better to predict the LVI status of patients in ESCC, which will also be our next research direction.
Conclusion
The quantitative features based on CECT may serve as potential noninvasive indicators for predicting LVI in ESCC. The combination of clinical features and CECT-derived parameters may be effective in predicting LVI status preoperatively in ESCC.
Footnotes
Abbreviations
Acknowledgements
First and foremost, I would appreciate the organization of the First Affiliated Hospital of Soochow University which gives me a comfortable learning atmosphere. Second, I would like to show my deepest gratitude to Prof. Chunhong Hu, a respectable, responsible, and resourceful scholar, who has provided me with valuable guidance in every stage of the writing of this thesis. His keen and vigorous academic observation enlightens me not only in this thesis but also in my future study. Last but not least, I shall extend my thanks to all my teachers and colleagues who have helped me to develop fundamental and essential academic competence.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by the ethics committee of Huai’an First People's Hospital (KY-2022-045-01). As a retrospective study, the requirement for informed consent was waived.