
Abstract
Keywords
Introduction
Due to the high degree of malignancy, the easy occurrence of local vascular invasion,e distant metastasis, and other reasons, the overall resection rate of pancreatic cancer is less than 20%, and the 5-year survival rate is less than 10%.e 1 Data from the National Comprehensive Cancer Network (NCCN) in 2019 shows that pancreatic cancer is the 10th leading cause of cancer-related death worldwide. Adenocarcinomas represent 85% of the pancreatic cancers originating from exocrine pancreatic ductal epithelial cells. The rest include acinar cell carcinoma derived from pancreatic exocrine acini and pancreatic neuroendocrine tumors derived from neuroendocrine cells. 2 Although the specific mechanism of its pathogenesis is not clear, a large number of epidemiological studies have shown that smoking, obesity, history of diabetes, and chronic pancreatitis are high-risk factors for pancreatic cancer.
At present, curative resection is the only way to cure pancreatic cancer. 3 Patients with unresectable tumors can be treated with therapies such as chemotherapy, radiotherapy, immunotherapy, and molecular targeted therapy. With the development in surgical techniques and the progress of anesthesia and monitoring, the postoperative complications of the pancreas showed an overall downward trend, and the perioperative mortality rate was less than 2%. 4 However, the onset of pancreatic cancer is insidious, and most patients have no specific symptoms. As a result, 80% of the patients have lost the chance of surgical resection at the time of diagnosis. 5 Even after R0 resection, the median survival time of patients eeremains only 12–20 months. 6 Hishinuma and others conducted autopsies on 27 patients with pancreatic cancer and found that 85% to 90% of the patients died due to tumor recurrence. 7 Pancreatic cancer usually relapses within 2 years after the operation; 8 therefore, there is an urgent need for potential markers that can predict postoperative prognosis and recurrence of pancreatic ductal adenocarcinoma (PDAC).
Serum carbohydrate antigen 19-9 (CA19-9) is a tumor marker with a high sensitivity to pancreatic cancer. Studies have found that distant metastasis of pancreatic cancer increases serum CA19-9 levels, and the degree of increase is closely related to the degree of metastasis. 9 The size of the tumor has always been considered to be an independent risk factor for prognosis after a surgical treatment because tumor size is related to invasiveness. Larger tumors are more likely to have local invasion and lymph node metastasis, and it is challenging to achieve R0 resection. The purpose of this study was to combine CA19-9 with total tumor volume (TTV) to investigate the effect of the CA19-9/TTV ratio on the long-term prognosis and tumor recurrence of PDAC in patients undergoing pancreaticoduodenectomy (PD).
Methods
This study has been reported using the STROBE checklist for cohort studies. 10
Inclusion and Exclusion Criteria
The data of patients with PDAC who underwent PD in the Department of Hepatobiliary Surgery of Beijing Chaoyang Hospital from January 2013 to December 2019 were analyzed retrospectively (n = 333). After implementing the relevant inclusion/exclusion criteria and NCCN guidelines, 2 200 patients with PDAC were enrolled (Figure 1).
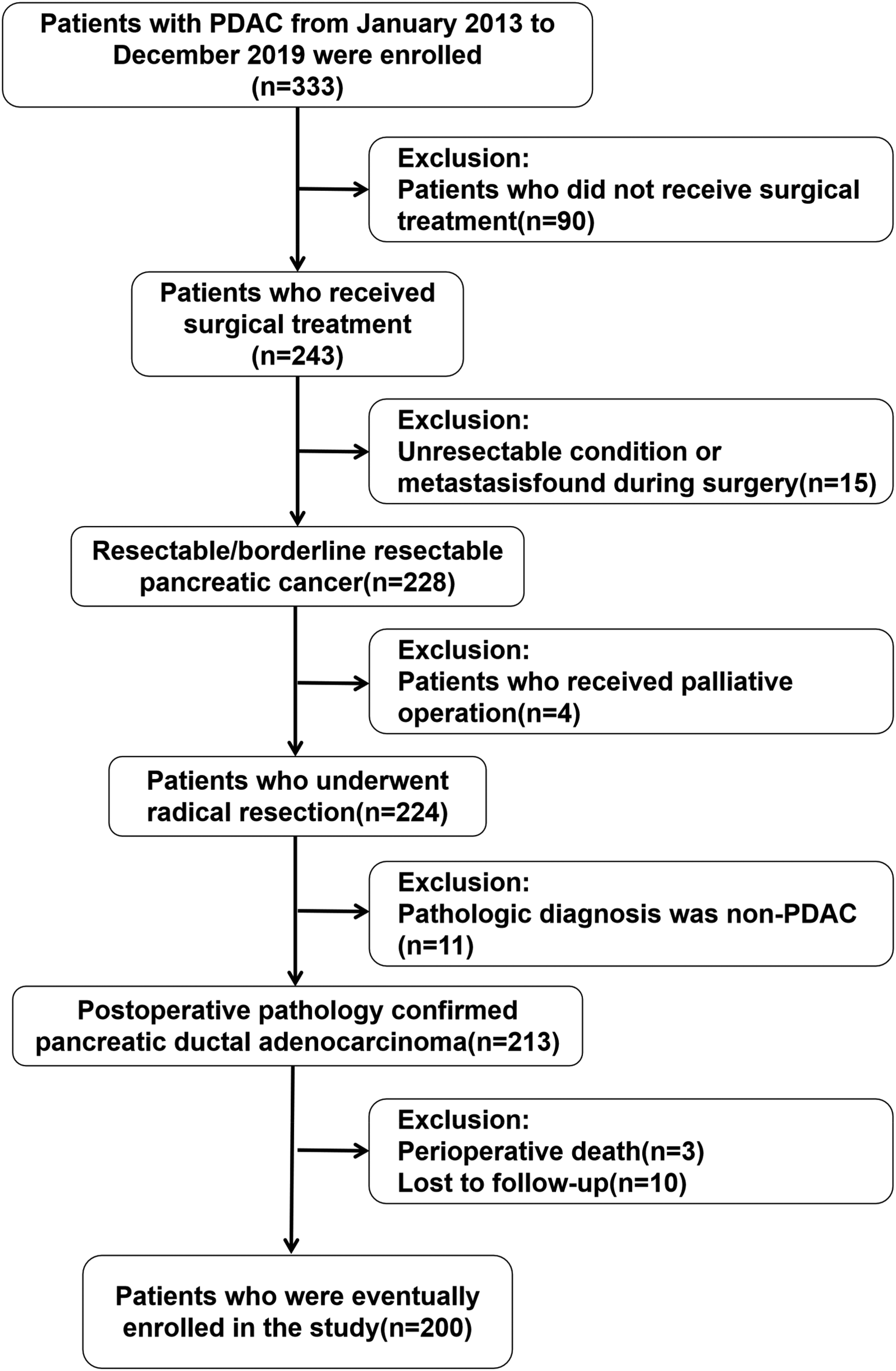
Flow chart of patients with PDAC.
The inclusion criteria were as follows: (1) Patients with PDAC who underwent PD between January 2013 and December 2019; (2) 20–85 years old; (3) assessed as resectable PDAC or borderline resectable PDAC according to the NCCN guidelines; (4) en bloc resection of the tumor during surgery; (5) postoperative pathology confirmed pancreatic ductal adenocarcinoma; (6) informed consent from the patients and their families regarding the mode of operation and treatment strategy.
The exclusion criteria were as follows: (1) unresectable condition or metastasis found during surgery; (2) surgical rule violations; (3) pathologic diagnosis other than conventional ductal adenocarcinoma; (4) postoperative follow-up data were incomplete or lost to follow-up; (5) perioperative deaths.
The Optimal Cut-Off of CA19-9/TTV and Grouping Basis
When available, the tumor volume was measured by volumetric computed tomography (CT) scan or magnetic resonance imaging or calculated using the following formula: 4/3 × 3.14 × (maximum tumor radius in cm). 3 The distribution of TTV is shown in Supplemental Figure 1. Chemiluminescence microparticle immunoassay was used to detect serum CA19-9 in tumor diagnosis, and its normal value was less than or equal to 37 U/mL. The receiver operating characteristic curve was drawn based on CA19-9/TTV and 1-year survival, and the best cut-off value was 5.62 (area under the curve [AUC]: 0.633, 95% CI: 0.548-0.718) (Figure 2). Patients with CA19-9/TTV ≤ 5.62 were labeled as group 1, and patients with CA19-9/TTV > 5.62 were group 2. There were 61 patients in group 1 and 139 patients in group 2.
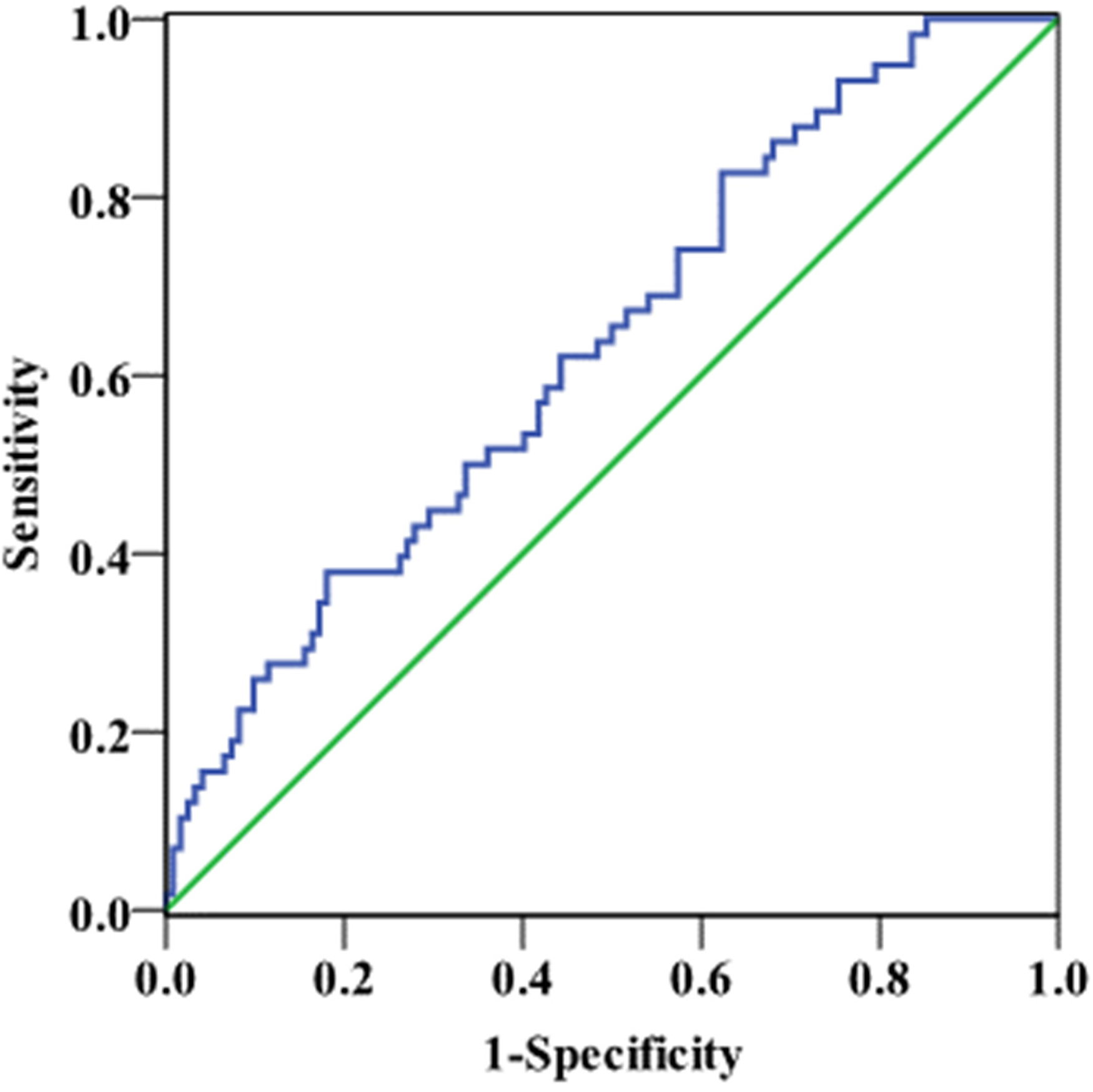
ROC curve of CA199/TTV and 1-year survival.
Index Analysis and Follow-up Strategy
The clinical and pathological data were extracted from the medical records, and perioperative data of the different groups were compared. The results of the CA19-9 test were taken from the patient's last blood sample before surgery. In the cases of patients treated for reducing jaundice, we rechecked CA19-9 the day before surgery; the frequency of postoperative follow-up was 1 and 3 months after the operation, once every 3 months within 2 years, and once every half a year for more than 2 years. The endpoints of follow-up were tumor recurrence and death. The contents of follow-up mainly included blood examination (including routine blood analysis, blood biochemistry, and tumor markers), imaging examination (including abdominal enhanced CT, pulmonary CT, and ECT), follow-up treatment, tumor recurrence and survival, and comparison of the long-term prognosis of the patients in different groups.
Statistical Analysis
The results are presented as mean ± standard error of the mean. Nominal data were compared using the χ2 tests, and continuous variables were compared using the Student's t-test. Survival outcomes were calculated using the Kaplan–Meier method and compared using the log-rank test. Only variables statistically significant by univariate analysis were included in the multivariate analysis performed using a Cox proportional hazards regression model. All statistical analyses were performed using SPSS, version 22.0 (IBM), and two-sided P < 0.05 was considered to be statistically significant.
Results
Clinicopathological Data of Perioperative Period
The 200 enrolled patients included 111 males and 89 females aged between 29 and 83 (62.8 ± 10.7) years. The initial symptoms were jaundice in 80 patients, abdominal pain in 83, atypical gastrointestinal symptoms in 10, and physical examination in 27 cases; 65 (32.5%) patients had a history of smoking and 67 (33.5%) had a history of diabetes. Among the 80 patients with jaundice symptoms, 37 patients were treated with jaundice reduction before the operation, including nine cases of ERCP and 28 cases of PTBD. Six patients received neoadjuvant therapy in group one (mFOLFIRINOX four cases, gemcitabine hydrochloride + nab-paclitaxel therapy two cases), and four patients in group two (mFOLFIRINOX three cases, gemcitabine hydrochloride + nab-paclitaxel therapy one case). All patients completed the operation, and the intraoperative blood loss was 500 (quartile, 400, 800) mL (range, 100-2000 mL). Blood transfusion was performed in 83 patients (39.5%). The operation time was (10.0 ± 3.0) h (range 4-18 h). Twenty-seven patients received postoperative chemotherapy in group one (mFOLFIRINOX 15 cases, combined gemcitabine hydrochloride + nab-paclitaxel therapy 12 cases), and 30 patients in group two (mFOLFIRINOX 17 cases, gemcitabine plus albumin-bound paclitaxel 13 cases). The comparison of clinicopathological data between Group 1 and Group 2 in Table 1 shows that there was no significant difference in clinicopathological data between the two groups.
The Data of Clinicopathological in Patients with Pancreatic Carcinoma.

Overall Prognosis
The median follow-up time was 45 months up to June 2020. By the date of follow-up, a total of 143 cases recurred after surgery, including 37 cases in group 1 and 106 cases in group 2. The recurrence rate in group 2 was significantly higher than that in group 1(76.3% vs 60.7%, P = 0.024), but there were no differences in the recurrence patterns (local, hepatic, lung, and other distant, P = 0.965). The overall median disease-free survival (DFS) was 14 months. The 1-, 3-, and 5-year DFS rates were 53.9%, 22.1%, and 16.7%, respectively (Figure 3A). The median overall survival (OS) of the patients was 18 months, and the overall 1-, 3-, and 5-year survival rates were 65.1%, 26.0%, and 15.5%, respectively (Figure 3B).

A Kaplan-Meier curve for disease-free survival. B Kaplan-Meier curve for overall survival.
Comparison of Long-Term Prognosis Between Two Groups
The median DFS of patients in groups 1 and 2 was 24 months and 12 months, respectively, and the 1-, 3-, and 5-year DFS rates were 69.5%, 38.7%, 25.6%, and 46.8%, 14.8%, and 12.7%, respectively (P = 0.002, Figure 4A). The median OS of patients in Group 1 and Group 2 was 26 months and 15 months, respectively, and the 1-, 3-, and 5-year OS rates were 81.6%, 42.8%, 26.0% and 57.5%, 19.0%, 11.2%, respectively (P = 0.002, Figure 4B).

A Kaplan-Meier curve for disease-free survival in patients with different groups. B Kaplan-Meier curve for overall survival in patients with different groups.
Univariate Analysis of Postoperative Long-Term Prognosis and Tumor Recurrence
Sex, age, diabetes, preoperative serum bilirubin, preoperative serum CEA, R0 resection, nerve invasion, lymph node metastasis, tumor diameter, pathological differentiation, TNM stage, postoperative chemotherapy, CA19-9/TTV, postoperative CA19-9 value, intraoperative hemorrhage, and blood transfusion were included in the univariate analysis. The log-rank test showed that lymph node metastasis, nerve invasion, pathological differentiation, CA19-9/TTV level, postoperative CA19-9, and TNM stage were risk factors that might affect long-term prognosis and tumor recurrence (P < 0.05, Tables 2 and 3).
Univariate Analysis of Postoperative Long-term Prognosis.

Univariate Analysis of Postoperative Tumor Recurrence

Multifactor Analysis of Postoperative Long-Term Prognosis and Tumor Recurrence
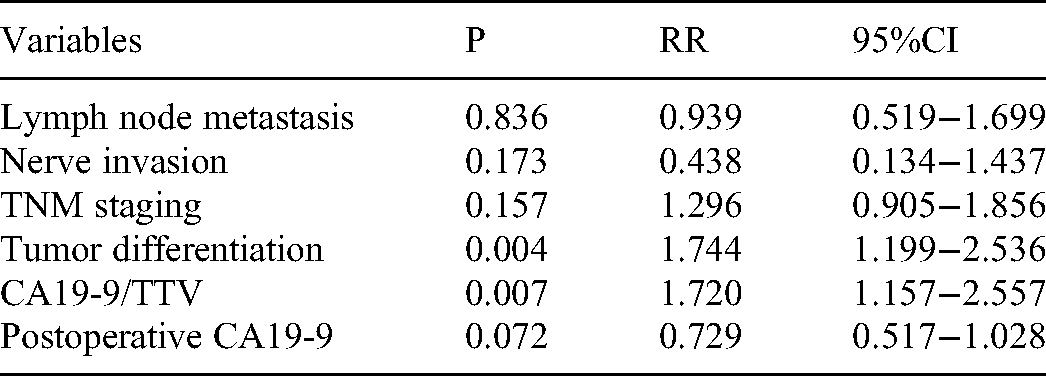
The Cox proportional hazard model included lymph node metastasis, nerve invasion, pathological differentiation, CA19-9/TTV level, postoperative CA19-9, and TNM stage, all of which are factors that may affect the long-term prognosis and tumor recurrence. The results showed that tumor differentiation and CA19-9/TTV were independent risk factors for the long-term prognosis of PDAC (P = 0.004, P = 0.007) (Table 4), as well as for tumor recurrence (P = 0.008, P = 0.008) (Table 5).
Multifactor Analysis of Postoperative Long-term Prognosis.
Multifactor Analysis of Postoperative Tumor Recurrence.

Discussion
Based on the NCCN guidelines, pancreatic carcinoma can be divided into resectable, borderline resectable, and non-resectable pancreatic cancer. 2 Curative resection is considered to be the only effective way to cure this type of disease. However, resectable pancreatic cancer often relapses after surgical treatment. Previous studies have found that the median disease-free time of patients with resectable pancreatic cancer was 7.0–21.0 months,11–14 the median survival time was 20.1–22.8 months, and the 5-year survival rate was only 20.7–22.5%. 15 In view of the poor prognosis and high recurrence rate after the diagnosis, we hope to implement early intervention for high-risk patients. It is essential to identify markers that can indicate postoperative patients’ long-term prognosis and recurrence risk with PDAC.
During tumorigenesis, abnormal glycosylation often occurs on the cell surface. CA19-9 is an oligosaccharide antigen secreted by adenocarcinoma cells into the blood through the thoracic duct. It is abnormally elevated in the serum of patients with pancreatic cancer, gallbladder cancer, and cholangiocarcinoma. 16 Magnani JL 17 found that CA19-9 was expressed regularly in cells of the pancreaticobiliary system and was initially detected by monoclonal antibody 19-9 18 at a very low level in the serum of normal individuals (< 37 U/mL). Expression of CA19-9 in many cancers, such as colorectal, gastric, ovarian, cholangiocarcinoma, and pancreatic carcinoma, has been determined since.
A retrospective analysis by O’Brien et al. 19 showed that within 2 years of diagnosis of pancreatic cancer, CA19-9 levels were significantly upregulated with a specificity of 95% and a sensitivity of 53%. CA19-9 is being used as a common auxiliary diagnosis and prognostic index for pancreatic cancer. Some studies have shown that with an increase in the degree of malignancy of pancreatic cancer, the level of serum CA19-9 increases. This is of great value for condition monitoring and evaluation. 20 The study by Liu 21 asserted that the positive rate of CA19-9 in the serum of patients with pancreatic cancer was 84.54%. In addition to indicating the occurrence and progression of pancreatic cancer, CA19-9 levels can also predict tumor recurrence. Nishio et al. reported that preoperative serum CA19-9 ≥ 529 U/mL is an independent risk factor for pancreatic cancer recurrence after radical resection. 22 Studies by Asaoka et al. 23 showed that the overall 2-year survival rate of patients with high CA19-9 (≥ 230 U/mL) was 37.5%, while that of the low-level group was 89.9%, with the difference being significant. Nevertheless, serum CA19-9 levels are elevated in pancreatic cancer and other cancers, and some inflammatory diseases. It has been reported that high CA19-9 levels as diagnostic criteria may lead to false-negative diagnoses in patients with a negative Lewis blood group phenotype. 24 Therefore, the sensitivity and specificity of CA19-9 as a diagnostic and prognostic tool are low. Hence, the sensitivity and specificity of CA19-9 as a diagnostic and prognostic tool are limited, and it is difficult to determine the level of CA19-9 that should be considered as a diagnostic criterion for pancreatic cancer.25–27
A small tumor size indicates that the tumor is at an early stage of differentiation; tumor size has long been considered an independent risk factor for pancreatic cancer surgery prognosis. Satake et al. 28 pointed out that a 4 mm pancreatic tumor is micro-pancreatic cancer, and early detection of micro-pancreatic cancer can improve the overall prognosis of pancreatic cancer. However, micro-pancreatic cancer is not an early pancreatic cancer that can be cured by surgery alone. Benassai et al. 29 believed that a tumor diameter of > 3 cm would lead to a poor prognosis. This might be related to the fact that the larger the tumor, the more likely it is to invade surrounding tissues, nerves, and extra-pancreatic tissues.
Hazem et al. 30 have discussed the relationship between serum alpha-fetoprotein/TTV and tumor recurrence after hepatectomy for liver cancer. A total of 286 patients were included in the study, and the patients were divided into AFP/TTV ≤ 2 and AFP/TTV > 2 groups. The 1-, 3-, and 5-year DFS rates of the two groups were 79.3%, 65.8%, 48.1%, and 69.6%, 41.1%, and 32.1%, respectively, suggesting that AFP/TTV > 2 can indicate the recurrence of liver cancer after hepatectomy. The study led us toward the question of whether the concentration of CA19-9 per unit volume of the tumor could better predict postoperative recurrence and prognosis in patients with pancreatic cancer than the reference serum level of CA19-9 and tumor volume alone. In our study, the multivariate analysis showed that tumor differentiation and CA19-9/TTV were independent risk factors for tumor recurrence and poor prognosis of patients with PDAC after PD. The long-term prognosis of group 2 was significantly worse than that of group 1, and the recurrence rate was considerably higher. We believe that the lower the level of tumor differentiation, the higher is the degree of malignancy of the tumor, and the worse would be the prognosis; Furthermore, there are limitations in determining the prognosis of PDAC patients by tumor size or serum CA19-9 alone. Tumor volume cannot fully account for the tumor'sits biological characteristics; serum CA19-9 levels are often affected by other factors such as bile duct obstruction. It is of great significance that the combination of the two can eliminate many confounding factors. CA19-9/TTV is also of great value in the postoperative prognosis of patients with pancreatic cancer. Based on our study, patients with a higher ratio of CA19-9/TTV should receive preoperative treatment, strengthened postoperative follow-up, and appropriate adjuvant therapy to improve the long-term prognosis of PDAC following PD.
The limitation of this study is that it was a retrospective study conducted at a single center. The sample size of patients with pancreatic cancer is insufficient, the time span is long, and the experience level of surgeons is different. The above limitations may lead to a bias in the results; hence, more data from multiple centers are required for further verification of our results.
In conclusion, CA19-9/TTV and tumor differentiation are independent risk factors for the prognosis of PDAC. CA19-9/TTV > 5.62 predicts a poor prognosis and may be a new marker for lower survival benefits.
Supplemental Material
sj-png-1-tct-10.1177_15330338221078438 - Supplemental material for Ratio of CA19-9 Level to Total Tumor Volume as a Prognostic Predictor of Pancreatic Carcinoma After Curative Resection
Supplemental material, sj-png-1-tct-10.1177_15330338221078438 for Ratio of CA19-9 Level to Total Tumor Volume as a Prognostic Predictor of Pancreatic Carcinoma After Curative Resection by Junming Xu, Shaocheng Lyu, Yang Zhao, Xinxue Zhang, Zhe Liu, Xin Zhao and Qiang He in Technology in Cancer Research & Treatment
Footnotes
Abbreviations
Acknowledgements
We will thank the patients for their great help in this report. This paper is supported by Dr HQ.
Ethics Approval
The conduct of the study complied with the Declaration of Helsinki and was approved by the Ethics Committee of Beijing Chaoyang Hospital (Acceptance No.: 2020-5-20-4; Number: 2020-CO-302). It's a project with waived informed consent.
Availability of Data and Materials
The data used and analyzed in this study is included in the article or are available from the corresponding and first authors on reasonable request.
Authors’ Contributions
Contributions: (I) Conception and design: Junming Xu,Shaocheng Lyu and Yang zhao; (II) Administrative support: Qiang He; (III) Provision of study materials or patients: Xinxue Zhang, Zhe Liu; (IV) Collection and assembly of data: Junming Xu and Zhe Liu; (V) Data analysis and interpretation: Xinzhao and Shaocheng Lyu; (VI) Manuscript writing: All authors.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.