
Abstract
Introduction
Lung cancer is a common malignant tumor worldwide. In 2008, lung cancer replaced liver cancer as the leading cause of death in China’s malignant tumor population. According to statistics, 600,000 people die of lung cancer in China every year. 1 The lung is a common metastatic site for malignant tumors throughout the body. Clarifying the histopathological type of tumor is the basis for judging its biological behavior, formulating a reasonable treatment plan, and prognostic evaluation. Therefore, accurately judging the type is the key to tumor staging and optimizing treatment. Although the histopathological examination is the gold standard for lung cancer classification, it must be obtained through invasive methods such as surgical resection or needle biopsy, which may not only cause many complications, but sometimes it is impossible to accurately determine the type. 2 Therefore, how to use noninvasive methods to determine the type of diseased tissue is always the goal of exploration.
Dual-energy computed tomography (CT), which has imaging characteristics such as multiparameter and quantitative analysis, is a new technology in the CT imaging field in recent years. It can objectively reflect the tissue characteristics of the lesion through the comprehensive application of multiple parameters and analysis tools. Therefore, it has a potential value in determining the tissue source and scope of the disease, differential diagnosis, and efficacy evaluation. It has also achieved preliminary results in research on lung cancer screening and the determination of benign and malignant lung nodules. 3 Dual-layer detector spectral CT (DLCT) is the latest generation of dual-energy CT technology and its images can be reconstructed on the basis of original data. Compared with other dual-energy CT based on tubes, DLCT has certain technical advantages, and its application is worthy of further exploration in clinical research. 4
Methods
Research Object
This retrospective, single-center study was approved by our institutional review board, and a waiver of informed consent was obtained. Before the examination, an enhanced CT consent form was routinely signed, and all patient details were de-identified during the research. A total of 84 cases (60 males and 24 females), including 72 patients who underwent DLCT scans in our hospital from June to December 2019 and were pathologically diagnosed with lung tumors, and 12 cases clinically diagnosed with metastatic tumors by CT were consecutively collected. Among these cases, there were 20 squamous cell carcinomas, 24 adenocarcinomas, 26 small cell lung cancer (SCLC), and 14 metastatic tumors. The primary sites of 14 cases of metastatic tumors were hepatocellular carcinoma, mesenteric leiomyosarcoma, bladder cancer, adrenal cortex cancer, cardia adenocarcinoma, breast cancer, laryngeal cancer, colon cancer, rectal cancer, urothelial cancer, kidney cancer, breast cancer, rectal cancer, and thymoma, respectively. Among the 84 cases, 51 cases did not receive treatment before the examination. Pathological findings included 33 cases of fiber optic bronchoscopy biopsy, 26 cases of lung biopsy, 5 cases of cervical lymph node puncture, 4 cases of surgical resection, 1 case of pleural effusion cytology, 1 case of pericardial effusion cytology, 1 case of mediastinal lymph node puncture, and 1 case of thoracoscopic biopsy. Twelve cases of metastatic tumors were clinically diagnosed by CT. Among the 84 patients, 56 patients were treated, including squamous cell carcinomas (n = 13), adenocarcinomas (n = 14), SCLC (n = 20), and metastatic tumors (n = 9).
Scanning Methods
All patients underwent a chest plain scan and enhanced scan by using the conventional mode of DLCT (iQon, Phillips). Contrast agent (Iomeprol, Imeron 400 MCT, 400 mg/mL; Bracco Imaging Deutschland GmbH) was administered intravenously at a dose of 1.2 ml/kg at a flow rate of 2 to 2.5 mL/s, and then injected 30 mL normal saline at the same flow rate. The scan delay time after the contrast agent injection is 35 s and 65 s, which are considered to be the arterial and venous phase scans respectively. Scanning parameters: 120 kVp; automatic tube current (37−84 mAs); matrix 512 × 512; collimation 64 × 0.625 mm; reconstruction thickness and interval 0.9 mm/0.9 mm. Regular and spectral images were reconstructed using iDose4 and spectral level 6 (Philips Healthcare) reconstruction algorithms. The average volume-weighted CT dose index and dose length product are 4.4 mGy and 180 mGy*cm, respectively, corresponding to an effective dose of 2.5 mSv (conversion coefficient: 0.014). The scanning range is from the apex of the lungs to the level of the septal muscles, and the patient is asked to complete it under breath-holding. All patients had signed an informed consent form before undergoing enhanced scanning.
Image Postprocessing and Quantitative Measurement
A hospitalized radiologist with 3 years of radiology experience and a senior radiologist with 11 years of radiology experience jointly performed quantitative measurements of spectral data on an ISP workstation (IntelliSpace Portal v. 10.1, Philips Healthcare). In each patient, the lesion volume was semiautomatically segmented on the axial plane of the plain scan image, and the soft tissue window was set to produce the lung lesions of interest. Based on spectral image reconstruction, the software provides traditional CT images, effective atomic number images, and iodine density maps at the same time. For each patient, the following parameters of the solid part of the lesion of interest were obtained and recorded: the LCA of the lesion (mm2), the CT value (HU, HUa, HUv) of the plain, arterial and venous phases, iodine concentration (mg/ml) (ICa, ICv) and effective atomic number (Zeff[a], Zeff[v]) of the arterial and venous phases.
Statistical Analysis
SPSS22.0 software was used to analyze the measured data. All continuous variables were tested for normality and were represented by the mean ± standard deviation or median (interquartile range). Categorical variables were represented by numbers (%). Chi-square test, one-way variance analysis, or Kruskal–Wallis H test was applied to compare and analyze multiple groups. Bonferroni method was used in pairwise comparison. Differences between means were assessed by pairwise Welch's t-test to correct for unequal variances between groups. Multiple testings were computed using the Games–Howell test. P < .05 indicates that the difference is statistically significant.
Results
Comparison of Nonsmall Cell Lung Cancer, SCLC, and Metastases
There was no statistical difference in clinical characteristics of 84 patients, 20 squamous cell carcinomas, 24 adenocarcinomas, 26 SCLC, and 14 metastatic tumors (Table 1). A total of 8 CT indicators were included in the study, however, only the LCA between nonsmall cell lung cancer (NSCLC) and metastases, and between SCLC and metastases were discovered statistical differences, respectively (P < .05) (Table 1).
Comparison of Clinical Characteristics and CT Indexes of NSCLC, SCLC, and Metastatic Tumors.

Abbreviations: CT, computed tomography; NSCLC, nonsmall cell lung cancer; SCLC, small cell lung cancer; LCA, largest cross-sectional area.
*Compared with NSCLC, P < .05. #Compared with SCLC, P < .05.
Comparison of Squamous Cell Carcinoma, Adenocarcinoma, and SCLC
In 70 patients, the clinical characteristics of adenocarcinoma (n = 24), squamous cell carcinoma (n = 20), and SCLC (n = 26) were statistically different in gender (P = .003). And there is a statistically significant difference between the squamous cell carcinoma and the adenocarcinoma group in gender (P = .008) (Table 2). Among the 8 CT indicators, only LCA was statistically different among the 3 groups (P = .011), and between the squamous cell carcinoma group and the SCLC group (P = .012) (Table 2).
Comparison of Clinical Characteristics and CT Indexes of Squamous Cell Carcinoma, Adenocarcinoma, and SCLC.

Abbreviations: CT, computed tomography; SCLC, small cell lung cancer; LCA, largest cross-sectional area.
*Compared with squamous cell carcinoma, P = .008. #Compared with squamous cell carcinoma, P = .012.
Comparison of Untreated NSCLC, SCLC, and Metastases
In the untreated 51 patients, there was no statistical difference in clinical characteristics among NSCLC (n = 30), SCLC (n = 12), and metastatic tumor (n = 9) groups. Among the 8 CT indexes, the LCA, the HUv, the ICa, and the Zeff(v) were statistically different among the 3 groups (P < 0.05). HUv and Zeff(v) were statistically different between NSCLC and SCLC (P = .045,.016). Between NSCLC and metastases groups, only LCA was statistically different (P < .001), And there was a significant difference in ICa between SCLC and metastases (P = .021) (Table 3).
Comparison of Clinical Characteristics and CT Indexes of Untreated NSCLC, SCLC, and Metastases.

Abbreviations: CT, computed tomography; NSCLC, nonsmall cell lung cancer; SCLC, small cell lung cancer; LCA, largest cross-sectional area.
*Compared with NSCLC, P < .05. #Compared with SCLC, P < .05.
Comparison of Untreated Squamous Cell Carcinoma, Adenocarcinoma, and SCLC
Among the 42 untreated patients, the gender of squamous cell carcinoma (n = 14), adenocarcinoma (n = 16), and SCLC (n = 12) were statistically different (P = .019). Among them, there were significant differences between the adenocarcinoma and squamous cell carcinoma group (P = .017). Among the 8 CT indicators, the LCA and the Zeff(v) were statistically different among the 3 groups (P < .05). Between the SCLC and the squamous cell carcinoma groups, significant differences were discovered in LCA and Zeff(v) (P = .022, .015). And between SCLC and adenocarcinoma groups, only Zeff is statistically different (P = .008) (Table 4).
Comparison of Clinical Characteristics and CT Indexes of Untreated Squamous Cell Carcinoma, Adenocarcinoma, and SCLC.
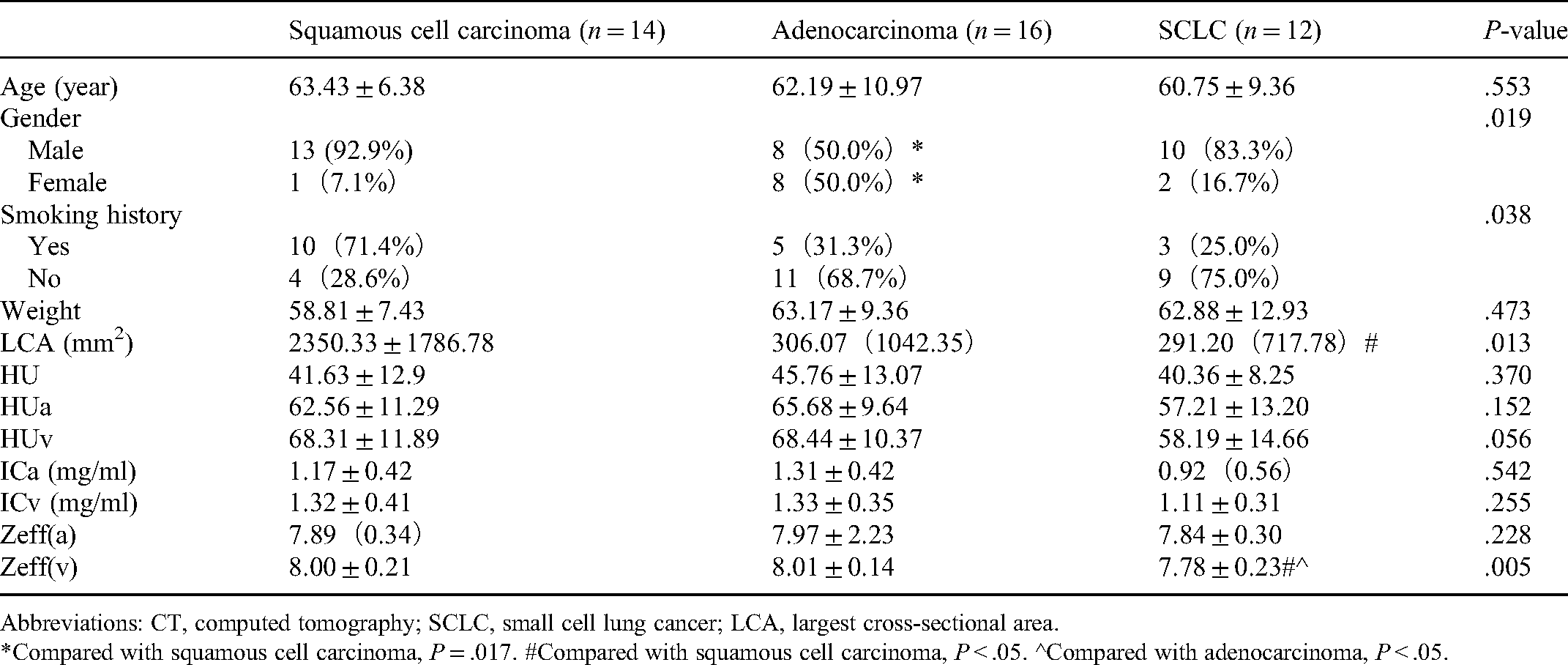
Abbreviations: CT, computed tomography; SCLC, small cell lung cancer; LCA, largest cross-sectional area.
*Compared with squamous cell carcinoma, P = .017. #Compared with squamous cell carcinoma, P < .05. ^Compared with adenocarcinoma, P < .05.
Comparison of Untreated NSCLC, SCLC, and Metastases with Similar LCA
Among the 27 untreated patients of NSCLC (n = 11), SCLC (n = 7), and metastases (n = 9) (LCA < 300 mm2), HUa was statistically different among the 3 groups (P = .008). In multiple comparisons, statistical differences were discovered between NSCLC and SCLC (P = .004) (Table 5).
Comparison of CT Indexes of NSCLC, SCLC, and Metastatic Tumor (LCA < 300 mm2).

Abbreviations: CT, computed tomography; NSCLC, nonsmall cell lung cancer; SCLC, small cell lung cancer; LCA, largest cross-sectional area.
*Compared with NSCLC, P = .004.
Comparison of Untreated Squamous Cell Carcinoma, Adenocarcinoma, and SCLC with Similar LCA
Among the 27 untreated patients of squamous cell carcinoma (n = 5), adenocarcinoma (n = 12), and SCLC (n = 10) (LCA < 1000 mm2), the HUa and the Zeff(v) were statistically different among the 3 groups (P < .05). In addition, a significant difference was discovered in the Zeff(v) between SCLC and adenocarcinoma groups (P = .029). But in the post hoc tests of HUa, no significant difference was discovered between SCLC and adenocarcinoma group (P = .065) (Table 6).
Comparison of CT Indexes of Untreated Squamous Cell Carcinoma, Adenocarcinoma, and SCLC (LCA < 1000 mm2).

Abbreviations: CT, computed tomography; SCLC, small cell lung cancer; LCA, largest cross-sectional area.
#Compared with adenocarcinoma, P < .05.
Comparison of NSCLC, SCLC, and Metastases After Treatment
In the 56 patients after treatment (including the posttreatment data of 23 patients in the untreated group), there was no statistical difference in clinical characteristics and CT indexes among NSCLC (n = 27), SCLC (n = 20), and metastatic tumor (n = 9) groups (Table 7).
Comparison of Clinical Characteristics and CT Indexes of NSCLC, SCLC, and Metastases After Treatment.

Abbreviations: CT, computed tomography; NSCLC, nonsmall cell lung cancer; SCLC, small cell lung cancer; LCA, largest cross-sectional area.
Comparison of Squamous Cell Carcinoma, Adenocarcinoma, and SCLC with Similar LCA After Treatment
In 47 patients, the clinical characteristics and CT indexes showed no statistical differences among squamous cell carcinoma (n = 13), adenocarcinoma (n = 14), and SCLC (n = 20) (P > .05) (Table 8).
Comparison of Clinical Characteristics and CT Indexes of Squamous Cell Carcinoma, Adenocarcinoma, and SCLC After Treatment.
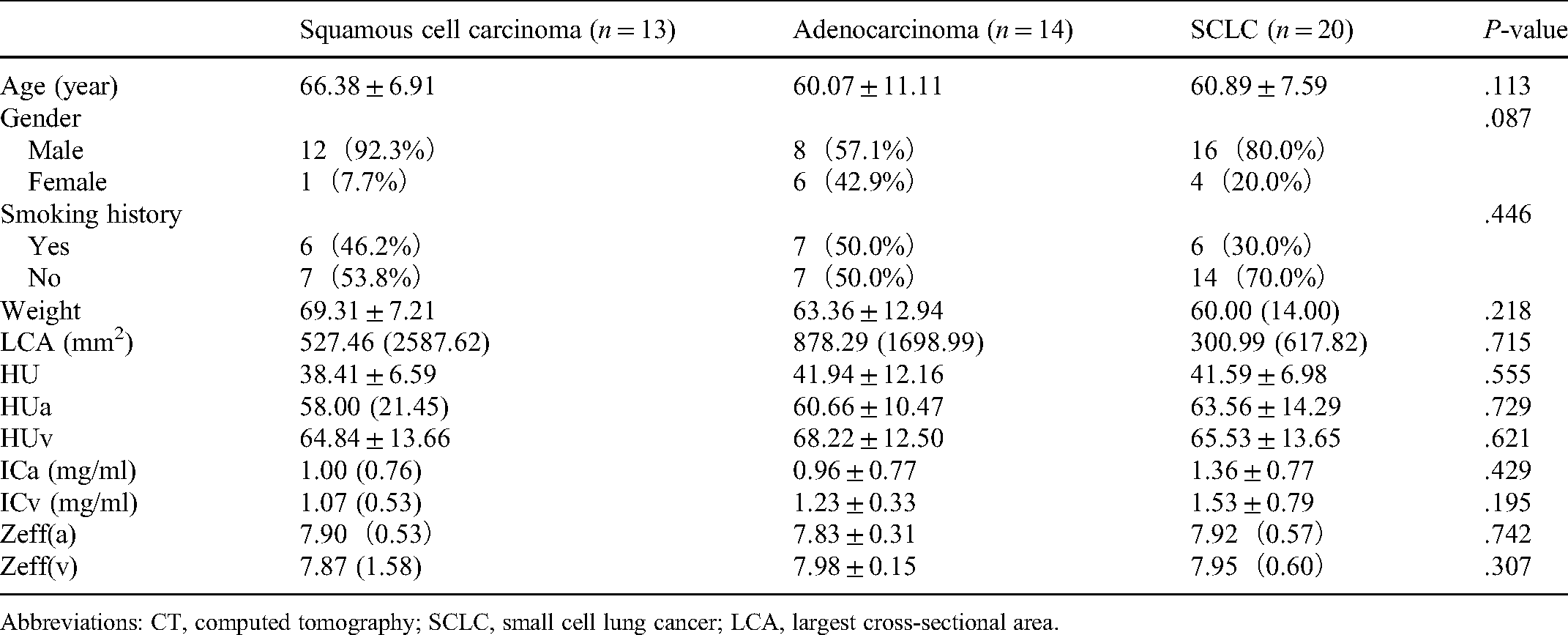
Abbreviations: CT, computed tomography; SCLC, small cell lung cancer; LCA, largest cross-sectional area.
Discussion
According to the histological type, lung cancer is divided into 2 main subtypes: NSCLC and SCLC, and then the most common types of NSCLC are squamous cell carcinoma and adenocarcinoma. Lung metastases are also very common and sometimes difficult to distinguish from the primary lung tumor. As the preferred imaging method for chest diseases, CT has an important value in the diagnosis of lung tumors. Ordinary CT diagnosis of lung tumors mainly focuses on morphology, and the pathological classification is mainly based on clinical experience to make preliminary inferences.
A well-known shortcoming of ordinary CT is that different substances and tissues may show similar attenuation levels at a single radiation energy level, that is, different tissues have similar CT values. Dual-energy CT (DECT), which uses material decomposition, is a noninvasive functional imaging method that can quantitatively measure tissue perfusion parameters and energy spectrum parameters and can noninvasively and quantitatively reflect changes in the metabolism and blood flow of the lesion. It has important clinical value in many aspects.3,5,6
DLCT has several advantages compared with other DECT. Firstly, because the original data obtained by DLCT can be used to retrospectively reconstruct traditional CT images at the projection level, there is no need to choose between traditional and spectral imaging before scanning. Hokamp et al 7 showed that the attenuation characteristics of the 72 keV single-energy image are almost the same as the traditional image, while the image quality has been improved. Secondly, the high- and low-energy level imaging is obtained in the same space and angle at the same time, so the imaging of moving organs is more ideal. Thirdly, because DLCT can be reconstructed on the basis of the original data, other DECT mostly reconstruct at the image level, for example, spectral imaging can be reconstructed at the projection level, but time and angle interpolation are required before reconstruction, its low-energy class-level virtual single-energy image quality is better, which is more conducive to the selection of measurement positions. 8
In this study, after analyzing all cases that have undergone radiotherapy, chemotherapy, or targeted therapy, no statistically different indicators were found except for LCA. The untreated subgroup analysis showed that compared with NSCLC, the HUv and the Zeff(v) of SCLC were significantly low (P < .05), and the untreated subgroup analysis of similar LCAs showed that HUa of SCLC is significantly lower than NSCLC’s (P < .05), which may be related to the lower capillary permeability of SCLC. Spira et al 9 used volume perfusion CT and histopathological results to assess the vascular correlation of lung cancer, and confirmed that compared with adenocarcinoma, the transmission constant of the parameter representing capillary permeability in SCLC was reduced.
In this study, although no statistical difference was observed, compared with NSCLC, the arterial phase CT value, arteriovenous phase iodine concentration, and arterial phase effective atomic number of SCLC were lower. These differences can be explained by the obvious differences in blood vessels and vasculature between SCLC and NSCLC. Compared with SCLC, the vascular beds of adenocarcinoma and squamous cell carcinoma are composed of many large blood vessels, which allow larger tumor blood volume and higher CT values in the arteriovenous phase.10,11 In addition, compared with NSCLC, tumor necrosis in SCLC is more common and widespread. Shi et al 12 also discovered that compared with SCLC, the dynamic volume perfusion CT parameters, including blood volume, blood flow, and permeability adenocarcinoma and squamous cell carcinoma were significantly higher.
Moreover, the untreated subgroup analysis showed that the arterial iodine concentration of metastases was significantly higher than that of SCLC (P < .05). Although no statistical difference was found, the iodine concentration and the effective atomic number in the arterial and venous phase of metastases were higher than that of the primary lung tumor, which is consistent with the results of Deniffel et al 13 study, showing the degree of vascularization of metastatic tumors was higher than that of the primary tumor.
Relevant literature shows that in lung squamous cell carcinoma, the tumor cells grow rapidly in piles, the tissue structure is dense, and the microvessel density is low. Adenocarcinoma has a loose tissue structure, high microvessel density, and rich blood supply, so the degree of enhancement and the iodine content in the lesion are high.14,15 Most literature, such as Bevilacqua A, etc, reported that the blood supply, enhanced scanning arteriovenous phase CT value, iodine content, and effective atomic number of adenocarcinoma was higher than squamous cell carcinoma.
16
However, in this study, no statistical difference was found in the arteriovenous CT value, iodine concentration, and effective atomic number between the adenocarcinoma and squamous cell carcinoma groups, which may be caused by the following reasons:
Squamous cell carcinoma is often accompanied by irregular necrosis within the tumor. To avoid necrosis, the surrounding area of the tumor is selected for measurement. The proliferation of blood vessels around the tumor is more active, resulting in higher enhancement values of squamous cell carcinoma. Adenocarcinoma is easily accompanied by mucus production, leading to uneven enhancement of the tumor which will result in no statistical differences in the arterial and venous phase CT value, iodine concentration, and the effective atomic number between squamous cell carcinoma and adenocarcinoma. Some primary tumors of lung cancer have large tumor bodies and uneven distribution of tumor blood vessels. Therefore, measurement errors are inevitable when selecting the substantial part. Since there is no absolute limit for the increase or decrease of iodine concentration, and different DECT suppliers have different accuracy of iodine measurement, the measurement of iodine density is usually relative to the difference between the lesion area of interest and the adjacent normal tissue. For example, the iodine density measurement value of small lesions with low enhancement in the high attenuation value area is extremely inaccurate and the data obtained from different image acquisition platforms cannot be compared. Research by Jacobsen et al
17
showed that the minimum iodine concentration that can be accurately detected by all DECT data acquisition platforms is 0.5 mg/mL. Dual-source CT can reach 0.2 mg/mL due to the best spectral separation, even if it is used the optimal thickness of the filter between 2 layers, the spectral energy separation of DLCT is still not ideal, which causes a large amount of energy overlap, and the iodine concentration value that can be accurately detected is large.
17
Insufficient samples of squamous cell and adenocarcinoma.
While the effective atomic number depicts the material make-up of each pixel and provides a higher degree of discrimination than attenuation in HU, in the comparative analysis of adenocarcinoma, squamous cell carcinoma, and SCLC, when the HUv does not show a statistical difference, the Zeff(v) is more sensitive in discovering the difference (Figure 1 shows 3 cases of Zeff images). And the statistically significant difference discovered between metastases and SCLC in ICa also indicates an additional value of spectral indexes than conventional CT.

Three cases of Zeff images (arterial phase and venous phase)
The findings of our study have some limitations. First, the analysis was retrospective and limited to a small sample size. Second, the number of included CT scans for similar LCAs was relatively low and, although we assessed a multitude of tumor types, no benign pulmonary lesions, and not all malignant pulmonary tumors are considered. Third, no other DECT technology was used besides DLCT as different systems are not available at our institution. Fourth, we acknowledge that additional imaging characteristics such as tumor location, size, calcifications, or presence of necrotic areas, which are an integral part of any clinical CT assessment, could have improved the credibility of our study. This study is a first step in demonstrating the difference in spectral indexes among different pathological types of lung tumors. Additionally, there are subtle differences in tissue composition that are more evident by HU quantification. So the assessment of pulmonary tumors of unknown origin should not be limited to single parameters but a combination of CT attenuation and DECT-derived parameters. Machine learning algorithms handling multiple predefined input variables or deep learning models that are capable of automatically learning and extracting imaging features are an interesting avenue for future research but will ultimately require larger data sets. 13
Conclusion
The energy spectrum parameters of DLCT have a certain clinical value in distinguishing NSCLC from SCLC in the Zeff(v) and distinguishing SCLC from a metastatic tumor in the ICa of the parenchymal part of lung tumor. It can assist in the evaluation of pathological types when pathological biopsy specimens are not available. Because this study is a single-center retrospective study and the sample size is small, and there are currently few studies using double-layer detectors to identify the pathological types of lung tumors, multicenter, and large-sample data are still needed to further confirm and explore its value.
Footnotes
Abbreviations
Acknowledgements
Not applicable.
Author Contributions
All authors contributed to data collection, research design, and revision of research content. All authors have approved its submission.
Authors’ Note
Xia Ma and Ming Xu contributed equally to this work. This retrospective, single-center study was approved by our institutional review board, and a waiver of informed consent was obtained.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research and/or authorship of this article.