
Abstract
Objective:
This study investigated the relationships of tumor status (stage, renal involvement, bone marrow status, bulky disease, liver function), tumor gene polymorphism, and methotrexate (MTX) dosage (stratified by treatment group) with blood MTX levels and adverse reactions (ADR).
Methods:
We retrospectively reviewed 63 mature B cell lymphoma patients who were treated in our center. Genotyping of the MTHFR 677 and SLCO1B1 genes was carried out, and the relationships between tumor status, polymorphism of the genes, MTX level, and ADR were analyzed.
Results:
Altogether, 63 children were included. The mean blood MTX concentration was 0.25 ± 0.2 umol/L at 45 h. Liver dysfunction and bulky disease were both correlated with MTX level (both P < 0.05). ADRs were higher among patients with blood MTX > 0.5 mmol/l at 45 h than for the groups with lower blood MTX. The MTHFR 677 CT genotype was correlated with liver function damage (P = 0.04); the rs11045879 locus CC genotype of SLCO1B1, stage IV, and bulky disease at the time of diagnosis were correlated with 4° neutropenia (P < 0.05). Stage IV, bulky disease, leukemia stage at the time of diagnosis, and C2 treatment group were correlated with severe anemia (P < 0.05). Stage IV, bulky disease, leukemia stage, renal invasion at the time of diagnosis, and C2 treatment group were associated with severe thrombocytopenia (P < 0.05). Bulky disease and renal invasion at the time of diagnosis were associated with severe mucositis and severe infection (P < 0.05).
Conclusion:
Taken together, our data demonstrate that gene polymorphism, MTX levels, tumor status, and treatment group might be useful to optimize MTX therapy and estimate toxicity.
Keywords
Introduction
High-dose methotrexate (HD-MTX) has been widely used in pediatric non-Hodgkin’s lymphoma (NHL) regimens as a central nervous system (CNS) disease preventative or treatment agent. 1,2 The dosage ranges from 3-8 g/m2 according to CNS status. However, MTX is associated with severe toxicities that can sometimes delay chemotherapy and increase the risk of patient relapse. 3 -5 Therefore, investigation of MTX predictors is key to effectively adjust the MTX dosage and reduce toxicity.
There are many transporters and enzymes involved in methotrexate metabolism. Single nucleotide polymorphisms (SNPs) of somatic and enzyme encoded genes are responsible for the main causes of adverse reactions (ADR) induced by MTX. The SLCO1B1 gene, is involved in the transmembrane transport of various drugs from blood to liver cells, including MTX as one of its subproducts. Studies have shown that polymorphism of the rs11045879 site is related to the pharmacokinetic characteristics of MTX and can affect the area under the drug-time curve and clearance rate. 6 -9
Many articles have reported side effects of HD-MTX in pediatric acute lymphoblastic leukemia, but no studies have been reported on its side effects in pediatric lymphoma. Moreover, the dose and infusion time of HD-MTX in pediatric mature B-cell lymphoma are different from those in acute lymphoblastic leukemia. Additionally, HD-MTX is often used in the first course of chemotherapy because children often have huge tumor load at that time. Therefore, we need to discover the high-risk factors for severe toxicity of HD-MTX in the first course of chemotherapy in pediatric mature B-cell lymphoma. In the present study, we investigated the role of MTHFR 677 and SLCO1B1 polymorphisms and of tumor status (bulky disease, renal involvement, bone marrow status, staging, treatment group) in MTX blood concentration and toxicity during first induction therapy in children with newly diagnosed mature B-cell lymphoma receiving HD-MTX according to the BCH-2010-mature B-cell lymphoma protocol.
Materials and Methods
Patients and Therapy
Of 64 children with newly diagnosed mature B cell lymphoma treated at the Hematological Center of Beijing Children’s Hospital Affiliated to Capital Medical University between October 2018 and March 2020, 63 were evaluated in this study; we excluded one patient who died before induction therapy. This study passed the examination of the ethics committee of our hospital (IEC-C-006-A03-V.05).
The patients were unrelated ethnic Chinese children 1-16 years old, with a mean age at diagnosis of 7.3 ± 3.4 years. All patients underwent biopsies from the tumor site or bone marrow, and a histopathologic diagnosis was determined using the Revised European-American Lymphoma (REAL) classification. Central pathology review consisted of a review of morphological, immunophenotypical, and genetic data from the original diagnostic biopsy. Fluorescence in situ hybridization (FISH) analysis for MYC gene rearrangement was performed on all specimens submitted for cytogenetic analysis. Staging was performed using the International Pediatric Non-Hodgkin Lymphoma Staging System. The treatment followed by the 2010-BCH-B-NHL regimen, which was modified by the FAB/LMB 96 study, and did not include CNS irradiation. Patients are stratified by risk into 4 treatment groups (A, B, C1, and C2) according to stage, CNS status, and so on; there were no group A patients in the current study. The treatment details are outlined in Table 1. The MTX doses in first induction differed by treatment group: groups B and C1 received 3 g/m2, while group C2 received 5 g/m2. In addition, all patients received other drugs concurrently. Leucovorin rescue was given at 24, 30, 36, 42, and 48 h from the start of MTX infusion. High plasma MTX levels after 45 h (<0.15 mmol/L was standard for all groups) were defined as an indication for prolonged rescue. Demographic data were collected on age at diagnosis, gender, pathology subtype, stage, bulky disease, renal involvement, bone marrow status, liver function before chemotherapy, and treatment group.
The Beijing Children’s Hospital Regimen for Mature B cell Lymphoma in 1st Induction Stratified by Different Treatment Groups.
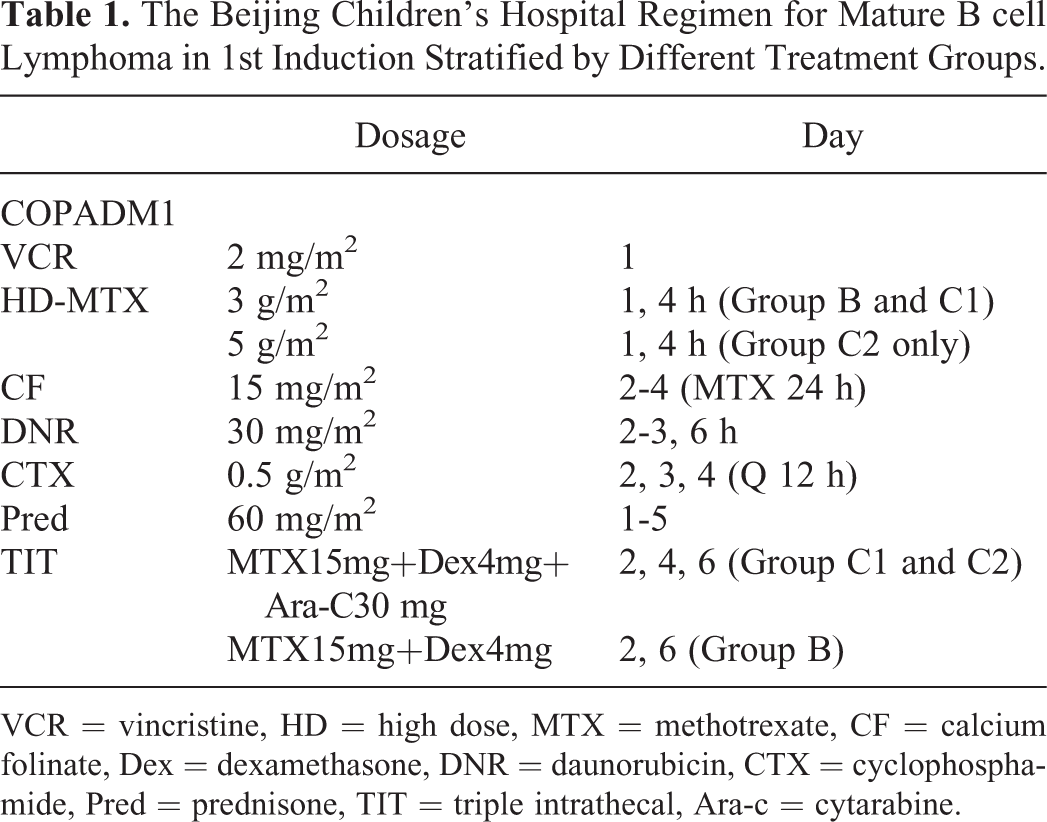
VCR = vincristine, HD = high dose, MTX = methotrexate, CF = calcium folinate, Dex = dexamethasone, DNR = daunorubicin, CTX = cyclophosphamide, Pred = prednisone, TIT = triple intrathecal, Ara-c = cytarabine.
Toxicity
We graded toxicities by the National Cancer Institute (NCI) Common Toxicity Criteria version 1.0, which included hematological toxicity (anemia, thrombocytopenia, neutropenia) and nonhematological toxicity (oral mucositis, renal toxicity, hepatic toxicity). Clinical data on toxicity were collected from electronic patient files. The highest grade of toxicity was observed in each patient during the first induction therapy period; no patients died from drug toxicity.
Plasma Concentration of MTX
MTX concentrations were evaluated at 45 h from the start of the first dose of MTX infusion. Measurement of MTX plasma level was performed by fluorescence polarization immunoassay.
Genotyping
DNA was extracted using a Genomic DNA Isolation Kit (U-gene, Anhui, China). Genotyping for the MTHFR 677 polymorphisms was performed as previously described. 4,5 The SLCO1B1 TaqMan SNP genotyping kit was used to detect the genotype of the SLCO1B1B gene at rs11045879 and rs4149056 using a 7500 real-time quantitative PCR instrument for direct sequencing, with the genotypes determined according to the kit instructions.
Statistical Analysis
SPSS 21.0 software was used for statistical analysis. The test for normality of the measurement data used the Shapiro-Wilk method. The data conforming to the normal distribution are reported as mean ± SD, with t-tests used for comparison between groups. Data that did not conform to normal distribution were represented by their median, with the Kruskal-Wallis rank-sum test used for comparison between groups. Enumeration data were expressed by case number or rate, and comparison between groups was made by t-test. The Wald progressive method was used to analyze the correlation between each influencing factor and adverse reactions in children with binary logistic regression. P < 0.05 was considered statistically significant.
Results
Baseline Information
Among the 63 cases, there were 50 males (79.4%) and 13 females (20.6%) (Table 2). The pathological classification included 43 cases (68.3%) of Burkitt lymphoma (BL), 9 cases (14.3%) of diffuse large B-cell lymphoma (DLBCL), and 11 cases (17.5%) of high-grade B-cell lymphoma (HGBCL). There were 9 (14.3%) Stage II cases, 33 (52.4%) Stage III cases, and 21 (33.3%) Stage IV cases. The numbers of patients in each treatment group were 15 (23.8%) in B, 37 (57.7%) in C1, and 11 (17.5%) in C2. Regarding bone marrow (BM) status at the beginning of the disease, 46 cases (73%) had no BM invasion while 17 cases (27%) had BM invasion, 6 of them at the leukemia stage. Liver function before treatment was normal in 41 cases (65.1%), while 14 cases (22.2%) had 1-2° liver dysfunction and 8 cases (12.7%) had 3-4° liver dysfunction. Regarding bulky disease (tumor diameter > 10 cm) before chemotherapy, 30 cases had no bulky disease (47.6%) while 33 cases (52.4%) did. Finally, 50 cases (79.4%) had no renal involvement, while 13 cases (20.6%) did. These data are summarized in Table 2.
Clinical Pathology Information and MTX Level at 45 h.

MTX Blood Concentration
All 63 children were treated with MTX (3-5 g/m2) for 4 hours. Intrathecal injection was performed at 24 hours after chemotherapy. The blood concentration of MTX was measured at 45 h, with an average of 0.25 ± 0.2 umol/L. Table 2 shows the relationship between the pre-chemotherapy state of tumor and blood MTX concentrations. There was a relationship between the degree of pre-chemotherapy liver dysfunction and MTX blood concentration (P < 0.05), with 4° liver function dysfunction before chemotherapy appearing to promote an increase of blood drug concentration. There was also a relationship between the presence of bulky disease and the plasma concentration of MTX (P < 0.05). Relative MTX concentrations for different pathologies were BL > HGBCL > DLBCL; for different stages were IV > II > III; for treatment groups were C2 > C1 > B; and for renal invasion were positive > negative. However, none of those differences were statistically significant.
Genotyping Results
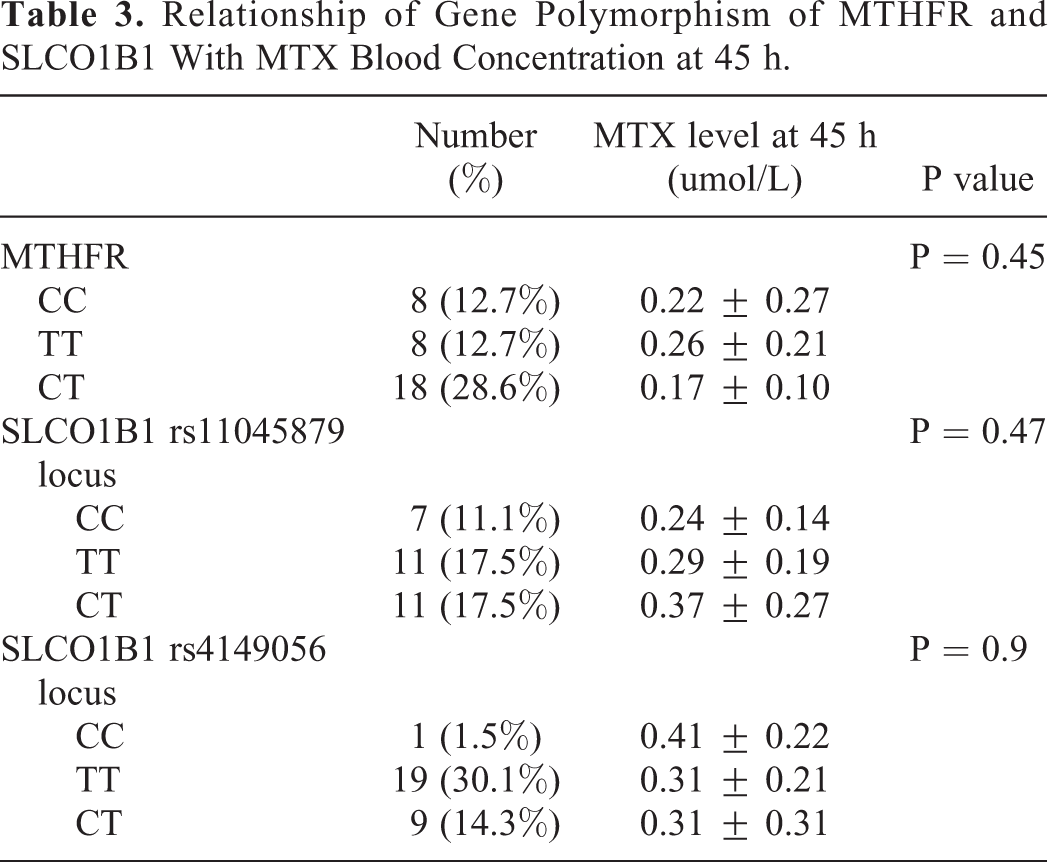
In this study, the MTHFR 677 gene (rs1801133 locus) was detected in 34 children, and the rs11045879 locus and rs4149056 locus in the SLCO1B1 gene were detected in 29 children (Table 3). The MTHFR 677 genotypes were CC, TT, and TC in 8, 8, and 18 cases, respectively. SLCO1B1 genotypes were CC, TT, and TC were found in the 2 loci. Among them, the CC, TT, and CT genotypes of rs11045879 occurred in 7 cases, 11 cases, and 11 cases, respectively, while the CC, TT, and CT genotypes of rs4149056 locus were 1 case, 19 cases, and 9 cases, respectively. Details are presented in Table 3.
Relationship of Gene Polymorphism of MTHFR and SLCO1B1 With MTX Blood Concentration at 45 h.
Relationship Between Gene Polymorphism and Blood MTX Concentration
The relationship between MTHFR 677 genotype and MTX blood concentration was TT > CC > CT, but there were no statistically significant differences. In the rs11045879 locus of the SLCO1B1 gene, the plasma drug concentration of the CT genotype was higher than for the other 2 genotypes, and that of the rs4149056 locus TT was higher than for the other 2 genotypes, but again there were no statistically significant differences.
Relationship Between MTX 45 h Blood Concentration and ADRs
The relationships between MTX blood concentration and side effects are cataloged in Table 4. The 63 children were divided into 3 concentration groups, with 23 patients in the < 0.15 umol/L group, 32 patients in the 0.15-0.5 umol/L group, and 8 patients in the > 0.5 umol/L group. Although the proportion of 4° neutropenia in the > 0.5 umol/L MTX group was higher than that in the 2 groups with lower concentrations (7/8 vs. 18/23 vs. 23/32), there was no significant difference (P = 0.62); likewise, while the proportion of 3-4° thrombocytopenia in the > 0.5 umol/L group was higher than in the other 2 groups (7/8 vs. 8/23 vs. 7/32), there was no significant difference (P = 0.07). The proportion of 3-4° mucositis in the > 0.5 mmol/L MTX group was higher than that of the other 2 groups (5/8 vs. 8/23 vs. 14/32), but with no significant difference (P = 0.57), and the proportion of severe infection in the > 0.5 umol/L group was higher than the other 2 groups (6/8 vs. 8/23 vs. 16/32), but with no significant difference (P = 0.14).
Relationships of MTX Level at 45 h With ADR.

Relationships of Gene Polymorphism of MTHFR 677C>T and SLCO1B1 rs11045879 and rs4149056 Locus With ADR
The relationship between drug metabolism genes and side effects is detailed in Table 5. The degree of liver damage is clearly related to different MTHFR 677C>T genotypes and side effects. Liver damage with the CT genotype is greater than with the CC genotype and TT genotype (P = 0.04), rs11045879 locus is related to neutropenia, and 4° neutropenia ratio of CC genotype is > TT genotype and CT genotype (P = 0.03).
Relationships of Gene Polymorphism of MTHFR and SLCO1B1 With ADR.

Relationship of Tumor Status With ADR
The relationships between pre-chemotherapy tumor status and the occurrence of side effects are shown in Table 6. Two factors were significantly related to 4° neutropenia: stage IV and bulky disease (both P < 0.05). Four factors were significantly related to 3-4° anemia after chemotherapy: Stage IV, C2 treatment group, bulky disease, and leukemia stage (all P < 0.05). Post-chemotherapy 3-4° thrombocytopenia was significantly related to Stage IV, treatment group C2, bulky disease, leukemia stage, and renal invasion (all P < 0.05). Post-chemotherapy 3-4° mucositis after chemotherapy was significantly related to bulky disease and renal invasion (both P < 0.05). Finally, severe post-chemotherapy infection was significantly related to bulky disease and renal invasion (both P < 0.05).
Relationship of Tumor Status With ADR.

ADR = adverse reaction, BL = Burkitt’s lymphoma, DLBCL = diffuse large B cell lymphoma, HGBCL = high grade B cell lymphoma, BM = bone marrow.
Relationships of Gene Polymorphism and Tumor Status With Prognosis
The relationships between gene polymorphism and tumor status with prognosis are shown in Table 7. There were 6 patients died of prognosis disease, all of them were early relapse (relapse time <6 m post chemotherapy). In gene polymorphism, MTHFR gene: 3 were CT genotype, 2 were TT genotype, 1 was CC genotype. In rs11045879 lotus, each genotype had 2 relapsed cases. In rs4149056 locus,3 patients were CC genotype,1 was TT genotype, 2 were CT genotype. In tumor status, 5 patients were BL, 6 patients were all stage Ⅳ and with bulky disease, 4 cases were in group C2, 3 cases were leukemia stage (blasts ≥ 25% in BM).
Relationships of Gene Polymorphism and Tumor Status With Prognosis.

Fours factors were significantly related to prognosis: BL subtype, stage IV, Group C2 and bulky disease (both P < 0.05).
Discussion
Mature B-cell lymphoma is the most common pathological type of non-Hodgkin’s lymphoma in children and is characterized by rapid clinical progress, high invasiveness, and severe symptoms. With a short course of high-intensity chemotherapy treatment (the current most commonly used treatment schemes in the international community being the LMB96 and BFM95 protocols), prognosis has been greatly improved. Mature B-cell lymphoma in children includes Burkitt lymphoma, diffuse large B-cell lymphoma, and high-grade B-cell lymphoma. At present, the LMB96 regimen combined with rituximab has achieved more than 85% 5-year event-free survival. Depending on their tumor evaluation status before chemotherapy, patients are divided into 4 treatment groups: A, B, C1, and C2. Each treatment group gets a different dose of chemotherapeutic drug and intrathecal injection, achieving a good hierarchical treatment. According to our hospital’s treatment experience for many years, in the first chemotherapy (high-dose MTX infused for 4 hours in groups B and C1-2), although the blood concentration of MTX at 45 h did not significantly increase, many children develop complications including severe oral mucositis, gastrointestinal mucositis, bone marrow suppression, and infection. Accordingly, this paper summarizes the clinical and pathological features of mature B-cell lymphoma in our hospital. To discover the causes of increased MTX blood concentration, we investigated the patients’ clinical characteristics, tumor status before chemotherapy (including stage, bone marrow invasion, renal invasion, and bulky disease), pre-chemotherapy liver function, treatment groups (MTX dose of 3 g/m2 in group B, 3 g/m2 in group C1, and 5 g/m2 in group C2 in first induction), and genes affecting MTX drug metabolism (MTHFR gene and SLCO1B1 gene). The risk factors for severe bone marrow suppression, liver function damage, mucositis, and severe infection can guide clinicians to take effective and feasible preventive measures for children with high-risk factors, reduce complications and improve the expected prognosis.
The mean MTX concentration was 0.25 ± 0.2umol/L at 45 h, with the mean MTX concentration in the Burkitt lymphoma being higher than that in the other 2 pathologies. The MTX concentration was higher in Stage IV patients than Stage II and III patients and was higher in treatment group C2 than in B and C1 (indicating a correlation between MTX dose and concentration). The MTX concentration in patients with renal invasion was higher than that in patients without renal invasion. Regarding genotypes, the MTX concentration was higher with the TT genotype of MTHFR 677 than with the other 2 genotypes, and with CT genotype in the rs11045879 locus in SLCO1B1 gene than with the other 2 genotypes. We also found that the MTX level was significantly higher in patients with severe liver dysfunction than in patients with normal liver function (P < 0.05), and in patients with rather than without bulky disease (P < 0.05). Therefore, it is necessary to protect the liver, carry out hydration and diuresis before chemotherapy, and strictly monitor the volume and renal function of the patients.
Relationship Between MTX 45 h Blood Concentration and ADR
In the group of patients with > 0.5 mmol/L MTX, the proportions of 4° neutropenia, 3-4° thrombocytopenia, 3-4° mucositis, and severe infection were all higher than in the other 2 groups. Therefore, actively reducing the concentration of MTX at 45 h < 0.5 mmol/L should effectively reduce the degree of myelosuppression, mucositis, and severe infection.
The Relationship Between the MTX Gene and ADR
For the rs1801133 locus of the MTHFR 677, the CT genotype was associated with the most severe liver damage (P = 0.04), and for the rs11045879 locus of SLCO1B1, the CC genotype had a higher rate of 4° neutropenia than the other 2 genotypes (P = 0.03). Thus, children with the CC genotype of rs11045879 locus of the SLCO1B1 gene can be given active liver protection treatment to avoid serious liver function damage. After chemotherapy, positive granulocyte stimulating factor can be given to stimulate bone marrow hematopoiesis, promote leukemia recovery as soon as possible, and avoid serious infection.
Relationship Between Tumor Status Before Chemotherapy and ADR
The results showed that stage IV and the presence of bulky disease were influencing factors of 4° neutropenia after chemotherapy (P < 0.05). Stage IV, C2 treatment group, bulky disease, and leukemia stage were all influencing factors of 3-4° anemia after chemotherapy (P < 0.05). Stage IV, C2 treatment group, bulky disease, leukemia stage, and renal invasion were all influencing factors of 3-4° thrombocytopenia (P < 0.05). The presence of bulky disease and renal invasion were influencing factors of 3-4° mucositis (P < 0.05). The presence of bulky disease and renal invasion were the influencing factors of severe infection (P < 0.05). We would thus recommend that clinicians appropriately adjust the treatment of patients with the above high-risk factors to reduce adverse reactions. For example, they can be given active transfusion of red blood cells and platelets after chemotherapy, give prophylactic antibiotics to prevent infection, improve active oral and anal mucosa care to reduce the occurrence of complications, shorten the time of bone marrow suppression, and begin the second course of chemotherapy as soon as possible. All of these maneuvers should improve the patients’ long-term prognosis.
Relationships of Gene Polymorphism and Tumor Status with Prognosis
There are 4 factors were significantly related to prognosis: BL subtype, stage IV, Group C2 and bulky disease (both P < 0.05), but there was no relationship between gene polymorphism whatever MTHFR gene or SLCO1B1with prognosis, maybe it’s because of the small number of patients, a lot of work is still needed to confirm.
Taken together, our data demonstrate that genotyping of MTHFR and SLCO1B1, measurement of blood MTX levels, full assessment of tumor status before chemotherapy, and consideration of treatment groups may be critical in attempts to optimize MTX therapy and to reduce or at least estimate toxicity.
Footnotes
Authors’ Note
Guarantor of integrity of entire study: Huang Shuang. Study concepts: Huang Shuang and Jin Ling. Study design: Huang Shuang, Zhang yonghong. Literature research: Huang Shuang, Yang Jing, Duan yanlong. Statistical analysis: Huang Shuang, Zhang Meng. Manuscript editing: Huang Shuang, Zhou Chunju. Manuscript revision/review Huang Shuang, Zhou Chunju, Zhang Yonghong. Manuscript final version approval: Zhang Yonghong. Medical ethics committee of Beijing Children’s Hospital Affiliated to Capital Medical University (IEC-C-008-A08-V.05.1). Obtained the consent from parents. Disclosure forms provided by the authors are available with the full text of this article.
Acknowledgments
This work was supported by the special fund of the Pediatric Medical Coordinated Development Center of Beijing Children’s Hospital Authority (XTZD20180204).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The special fund of the pediatric medical coordinated development center of Beijing children’s hospital authority (XTZD20180204).