
Abstract
Objective:
We aimed to investigate the diagnostic value of the vaginal microecology, serum miR-18a, and programmed death ligand-1 (PD-L1) for human papillomavirus (HPV)-positive cervical cancer.
Methods:
Eighty-four patients with HPV-positive cervical cancer were assigned to the observation group, 107 HPV-positive patients without cervical cancer were assigned to the positive group, and 191 healthy women were assigned to the control group. Vaginal microecology and serum levels of miR-18a and PD-L1 on the surface of CD4+ and CD8+ T cells were compared among the 3 groups. The observation group was further divided into subgroups according to patients’ characteristics for comparison. The diagnostic value of miR-18a and PD-L1 for HPV-positive cervical cancer was investigated.
Results:
Women in the control group had better vaginal microecology and lower levels of miR-18a and PD-L1 than those in the observation and the positive groups (all P < 0.05). Compared with the positive group, the observation group had similar vaginal microecology (all P > 0.05) but higher levels of miR-18a and PD-L1 (all P < 0.05). Moreover, the patients at stage III had higher levels of miR-18a and PD-L1 than those at stage I and II (all P < 0.05). The values of area under the curve for miR-18a and PD-L1 in the diagnosis of HPV-positive cervical cancer were over 0.8 (all P < 0.001).
Conclusion:
Patients with HPV-positive cervical cancer have vaginal microbial dysbiosis and high serum levels of miR-18a and PD-L1. miR-18a and PD-L1 have diagnostic value for identifying HPV-positive cervical cancer.
Keywords
Introduction
Human papillomavirus (HPV) is mainly transmitted through sexual intercourse. In most cases, the infection can be cleared spontaneously, whereas in some cases, the infection can stay. It is believed that high-risk HPV when remaining at a high level in human body for a long time, can lead to cervical intraepithelial neoplasia or cervical cancer. 1 Epidemiological data have revealed that there were about 527,600 new cases of cervical cancer and 265,700 deaths from cervical cancer in 2012 worldwide. Moreover, the morbidity of cervical cancer keeps increasing, and patients affected are becoming younger. 2 Although studies have demonstrated that high-risk HPV infection is the main cause of cervical cancer, the pathogenesis and prognosis of this disease are also associated with other factors such as vaginal microecology, inflammatory factors, genetic factors, and immune function of the body. 3,4 In recent years, surgical methods, chemotherapy, and radiotherapy have become the main methods for treating early cervical cancer, and the 5-year survival rate can exceed 90%. However, in patients with advanced or recurrent cervical cancer, the 5-year survival rate is less than 20% and 5%, respectively. 5 Therefore, it is of great significance to find out a specific marker for detecting the occurrence and prognosis of cervical cancer.
Programmed death-1 (PD-1) and its ligand, programmed death ligand-1 (PD-L1), are negative immunoregulatory factors discovered in recent years. Activations of PD-1 and PD-L1 can prevent the activation of T cells in the tumor microenvironment, thereby helping the tumor cells to escape the immune surveillance and killing. 6 Studies have shown that PD-L1 is highly expressed in a variety of solid tumors. 7 microRNA (miRNAs) is an endogenous non-coding RNA at a length of 19-25 nucleotides. It can negatively regulate the target genes after transcription and has a regulatory role in the occurrence, development, and invasion of the tumor cells. 8,9 Since miRNAs can exist in body fluids in an abundant and stable form, serum and plasma can be used as test specimen instead of primary tumor tissue as the testing can be noninvasive and convenient in the early diagnosis of tumor. Research has revealed that miR-18a is overly expressed in many solid carcinomas, such as liver cancer and esophageal cancer, and high level of miR-18a can be detected in patients’ serum, suggesting that miR-18a may be a novel biomarker in tumor diagnosis and the prognosis assessment. 10 Since cervical cancer is also solid cancer, whether there is an over-expression of miR-18a in patients with cervical cancer and the diagnostic significance of miR-18a in HPV-positive cervical cancer drew our attention. Therefore, in this study, we investigated the diagnostic value of vaginal microecology, miR-18a, and PD-L1 for identifying HPV-positive cervical cancer.
Materials and Methods
Participants
Of the patients treated in our hospital from January 2017 to January 2019, 84 patients with HPV-positive cervical cancer were assigned to the observation group, and 107 HPV-positive patients without cervical cancer were assigned to the positive group. Meanwhile, 191 healthy women were assigned to the control group. The study was approved by the Ethics Committee of our hospital, and informed consent was obtained from the participants and their family members. See Supplementary File.
Inclusion and Exclusion Criteria
Inclusion criteria
Inclusion criteria for the control group were as follows: 1) women who had normal menstrual cycle; 2) women who had a sexual partner or history of sexual intercourse; 3) women who did not receive any antimicrobial medicine over the past 3 months. 5
Inclusion criteria for the positive group were: 1) women who had positive HPV-DNA test result, and the HPV type was HPV16 or 18; 2) women who did not receive any antimicrobial medicine over the past 3 months; 3) women who had normal menstrual cycle; 4) women who had a sexual partner or history of sexual intercourse.
Inclusion criteria for the observation group were: 1) women who had cervical cancer confirmed by pathological examination, and the HPV type was HPV-16 or HPV-18; (2) women who did not receive any radiotherapy, chemotherapy, or immunotherapy; 3) women who did not have other malignant tumors or other infectious diseases; 4) women who had a sexual partner and sexual intercourse.
Exclusion criteria
Exclusion criteria for the control group were: 1) women who had other severe diseases such as immune or endocrine system diseases; 2) women who were menstruating or had irregular vaginal bleeding; 3) women who were pregnant or lactating; 4) women with poor compliance; 5) women who received uterine or cervical surgery in the past; 6) women with vaginitis or other inflammatory diseases that may affect the results of the study.
Exclusion criteria for the positive group were: 1) women with cervical cancer; 2) women who had other severe diseases such as immune or endocrine system diseases; 3) women who were menstruating or had irregular vaginal bleeding; 4) women who were pregnant or lactating; 5) women with poor compliance; 6) women who received uterine or cervical surgery in the past; 7) women with vaginitis or other inflammatory diseases that may affect the results of the study.
Exclusion criteria for the observation group: 1) women who received radiotherapy, chemotherapy, or immunotherapy; 2) women who had other severe diseases such as immune or endocrine system diseases; 3) women who were menstruating or had irregular vaginal bleeding; 4) women who were pregnant or lactating; 5) women with poor compliance; 6) women who received uterine or cervical surgery in the past; 7) women with vaginitis or other inflammatory diseases that may affect the results of the study.
Outcome Measures
Main outcome measures
The main outcome measures included the serum levels of miR-18a and PD-L1 on the surface of CD4+ and CD8+ T cells as well as vaginal microecology (cleanliness, presence of candida and trichomonas, pH value, lactobacillus level, and microbiota diversity and density). The diagnostic performance of the serum levels of miR-18a and PD-L1 on the surface of CD4+ and CD8+ T cells in detecting HPV-positive cervical cancer was analyzed using receiver operating characteristic (ROC) curves.
Secondary outcome measures
Patients in the observation group were further divided into subgroups based on their age, pathological type, differentiation degree, tumor size, vascular invasion, and clinical stage. The expression levels of serum miR-18a and PD-L1 on the surface of CD4+ and CD8+ T cells were compared between the groups.
Methods
Vaginal Microecological Examination
On the next day after grouping, the vaginal secretion of each participant was collected using 3 disposable swabs. One swab was used to make Wright-Giemsa stained dried smear for detecting the lactobacillus level and microbiota diversity and density under the oil immersion lens; another swab was placed in 0.85% sodium chloride for measuring the cleanliness of the secretion and levels of candida, trichomonas, and lactobacillus; the third swab was used to detect PH value of the vaginal secretion.
The interpretation of the results is listed in Table 1. 11 The microbiota diversity or density was considered as positive if its grade was II or above.
Classification of the Results of the Markers.

Abbreviation: HPF, high power field.
Detection of Serum Levels of Mir-18a and PD-L1 on the Surface of CD4+ and CD8+ T Cells
The fasting venous blood samples (3 ml * 2 tubes) were drawn from each participant the next morning after grouping. The blood samples were centrifuged at 3,000 rpm for 15 min. After separating the supernatant, the percentage of PD-L1 on the surface of CD4+ and CD8+ T cells in the peripheral blood was detected using a flow cytometer (BD FACSCalibur, USA). Meanwhile, total mRNAs were extracted from the blood sample in another tube for detecting the expression levels of miR-18a by RT-PCR (PCR kit: Takara, Japan). The primers (designed and synthesized by Dingguo Biotech, Beijing, China) are listed in Table 2. The universal downstream primers of miR-18a were from the reverse transcription kit (Mir-XTM miRNA First Strand kit, Takara, Japan). The reverse transcription and RT-PCR were performed according to the manufacturer’s instructions of the kits (RT-PCR kit: SYBR RT-PCR kit, Takara, Japan). The reaction conditions of the PCR were as follows: pre-denaturation at 95°C for 30 s, denaturation at 95°C for 5 s, and annealing at 60°C for 30 s; the cycles were repeated 35 times. The relative expression levels of miR-18a and U6 in each group were measured using the 2-ΔΔCt method with GADPH as the internal reference. Each sample was tested 3 times to calculate the average value.
Primer Sequences.

Statistical Analysis
SPSS 22.0 was applied for statistical analysis. Count data are presented as number or percentage and were compared by chi-square test and partitions of chi-square (α = 0.0167); measurement data are presented as mean ± standard deviation and were compared by one-way analysis of variance and Bonferroni post-hoc test. ROC curve was plotted to analyze the clinical value of serum miR-18a and PD-L1 in the diagnosis of HPV-positive cervical cancer. P < 0.05 indicated a statistically significant difference.
Results
Baseline Data
No intergroup differences were found in the baseline data (all P > 0.05). See Table 3.
Baseline Data in the 3 Groups.

Abbreviations: HPV, human papillomavirus; BMI, body mass index.
Vaginal Microecology in the 3 Groups
There were no intergroup differences in the presence of candida and trichomonas (both P > 0.05). However, the patients in the control group had better vaginal microecology in terms of cleanliness, pH value, lactobacillus level, and microbiota diversity and density than the patients in the observation and the positive groups (all P < 0.05). Meanwhile, no differences were found in the microecology between the observation and the positive groups (all P > 0.05). See Table 4.
Vaginal Microecology in the 3 Groups.

Note. **P < 0.01 vs. the control group.
The Expression Levels of Serum MIR-18a and PD-L1 on the Surface of CD4+ and CD8+ T Cells in the 3 Groups
Compared with the control group, the expression levels of serum miR-18a and PD-L1 on the surface of the CD4+ and CD8+ T cells were much higher in the observation and the positive groups (all P < 0.05). Moreover, the observation group had higher levels of these markers than the positive group (all P < 0.05). See Table 5.
The Expression Levels of Serum miR-18a and PD-L1 on the Surface of CD4+ and CD8+ T Cells in the 3 Groups.

* P < 0.05 vs. the control group; #P < 0.05 vs. the positive group.
The Expression Levels of Serum miR-18a and PD-L1 in Patients with HPV-Positive Cervical Cancer
The observation group was further divided into subgroups of age, pathological type, differentiation, tumor size, vascular infiltration, and clinical-stage for comparison of miR-18a and PD-L1 levels. The patients at stage III had higher levels of miR-18a and PD-L1 levels than patients at stage I-II (all P < 0.05). No differences were observed in the levels of these markers between patients with different characteristics in other subgroups (all P > 0.05). See Table 6.
The Expression Levels of Serum miR-18a and PD-1 in Patients With HPV-Positive Cervical Cancer.
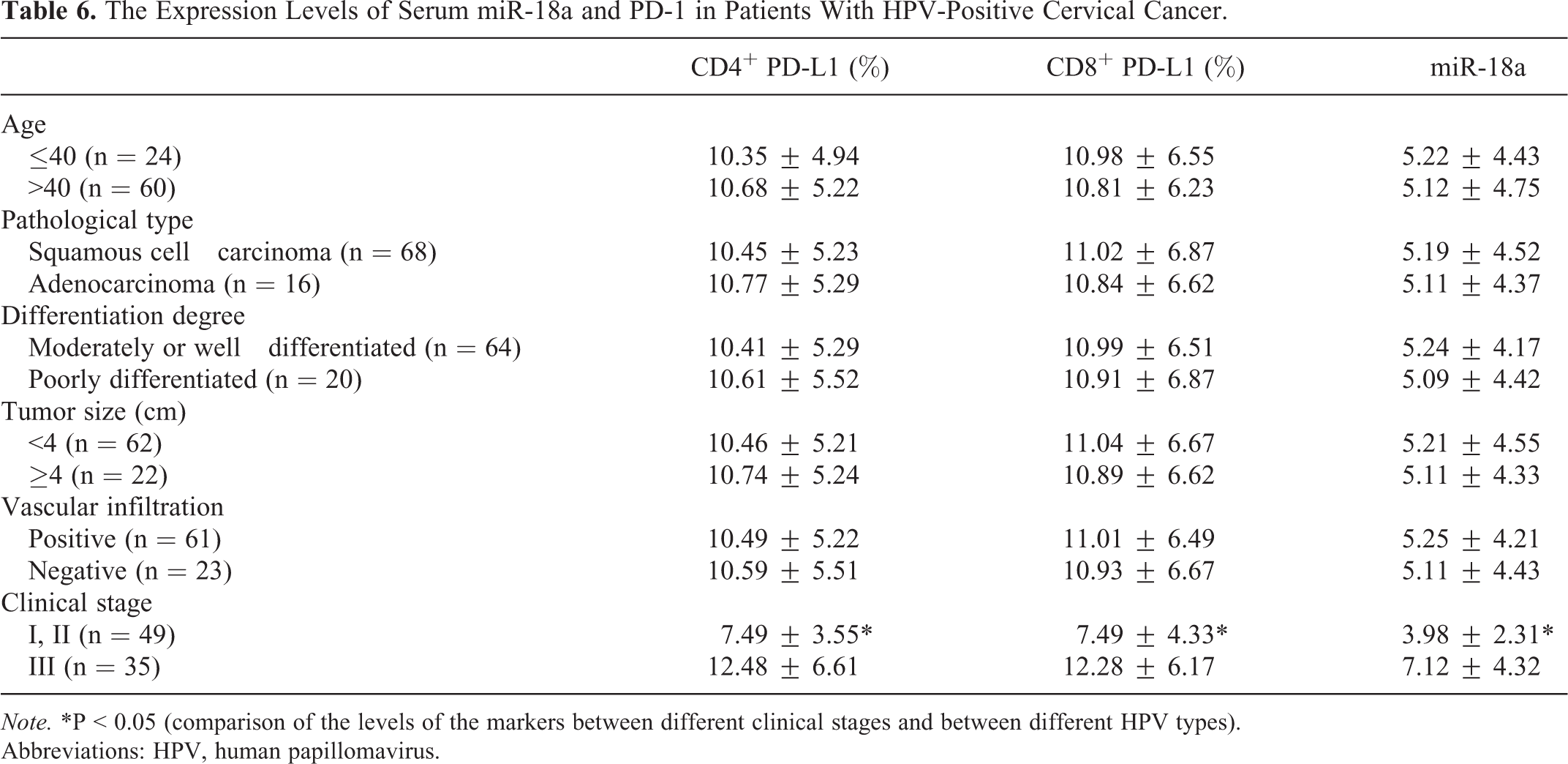
Note. *P < 0.05 (comparison of the levels of the markers between different clinical stages and between different HPV types).
Abbreviations: HPV, human papillomavirus.
ROC Curve Results
The values of the area under the curve (AUC) of miR-18a and PD-L1 in the diagnosis of HPV-positive cervical cancer were all over 0.700. See Table 7 and Figure 1.
ROC Curve Results.

Abbreviations: ROC, receiver operating characteristic; AUC, area under the curve; CI, confidence interval.

ROC curve results. ROC, receiver operating characteristic.
Discussion
Studies have shown that vaginal microbial dysbiosis is closely associated with HPV infection. The vaginal infection caused by microorganisms can lead to the damage of reproductive tract mucosa, thereby increasing the risk of HPV invasion. Moreover, HPV infection can exert a negative impact on the mucosal metabolism and immune system to further damage the vaginal microecology, thus forming a vicious circle. 12,13 It has been reported that vaginal microbial dysbiosis is one of the main factors affecting the clearance rate of HPV. Lactobacilli are the predominant bacteria that help to maintain normal vaginal microecology. Studies have demonstrated that the dysbiosis of vaginal microecology is closely related to bacterial vaginosis. 14 The lack of lactobacilli can weaken the body’s ability to inhibit the pathogenic microorganisms, thus increasing the risk of HPV infection and reproductive tract inflammation and even causing cervical lesions in some severe cases. 15 Liu et al., 16 after diagnosing 4,290 patients with bacterial vaginosis, found that bacterial vaginosis is closely associated with high-risk HPV infection. In our study, we found that compared with healthy women, patients who were HPV positive alone or who had HPV-positive cervical cancer were lack of lactobacilli and had much higher microbiota density and diversity, which aligns with the results of the previous studies. However, the correlations of trichomonas vaginalis and candida with HPV infection have not been elucidated. The results of our study showed no intergroup differences in the positive rates of trichomonas and candida among the 3 groups, and this result might be influenced by the sample size, sample source, and testing methods. Therefore, more studies need to be carried out in the future for verification.
PD-L1 level is closely related to the viral load of high-risk HPV. Persistent infection of high-risk HPV can inhibit the local immunity of the cervix transformation zone against HPV, and HPV may evade the host’s immune response by activating the immunosuppression of PD-1 / PD-L1, which eventually leads to the cervical disease. 17 It has been reported that the levels of PD-1 and PD-L1 in T-lymphocytes of patients with cervical lesions are markedly increased. 18 The results of our study showed that compared with the healthy women, the HPV-positive patients without cervical cancer and the patients with HPV-positive cervical cancer had much higher levels of PD-L1 on the surface of T-lymphocytes; moreover, the magnitude of increase in the PD-L1 levels was greater in the patients with HPV-positive cervical cancer than in the HPV-positive patients without cervical cancer. Also, the levels of PD-L1 in the patients with high-risk HPV were higher than those with low-risk HPV. These results are consistent with the previous studies. In addition, we also investigated the clinical significance of PD-L1 in the diagnosis of HPV-infected cervical cancer. The ROC curve results showed high sensitivity and specificity of PD-L1 on the surface of CD4+ and CD8+ T cells and demonstrated the clinical value of PD-L1 in the diagnosis of HPV-infected cervical cancer.
miR-18a belongs to the miR-17-92 cluster. It has been revealed that miR-18a can be a tumor suppressor gene. By regulating its downstream target gene, miR-18a can inhibit the in vitro proliferation of tumor cells, induce G1-phase arrest, and promote the apoptosis of tumor cells. 19,20 However, some studies have found that the expression levels of miR-18a are increased in breast cancer, glioblastoma, and other tumors. 21 The overexpression of miR-18a can activate cylinD1 via the PTEN-PI3K-AKTmTOR pathway, thereby promoting the proliferation of esophageal cancer cells. 22 The results of our study showed that the serum levels of miR-18a increased markedly in the HPV-positive patients and the patients with HPV-infected cervical cancer, and the levels of miR-18a in the patients with high-risk HPV were higher than those with low-risk HPV. These results suggest that miR-18a may participate in the pathogenesis of HPV-mediated cervical cancer. The ROC curve result showed high diagnostic performance of serum miR-18a. Since the sampling and testing methods are easy to be performed, miR-18a may serve as a good biomarker in the screening for HPV-infected cervical cancer.
In conclusion, patients with HPV-positive cervical cancer can have vaginal microbial dysbiosis and markedly increased serum levels of miR-18a and PD-L1. Moreover, the levels of PD-L1 and miR-18a rise with the increase of the HPV risk level. miR-18a and PD-L1 have clinical value in the diagnosis of HPV-positive cervical cancer. However, since the sample size was small and the levels of various indicators were not compared between patients with different HPV types, more studies need to be carried out in the future for further verification.
Supplemental Material
Supplemental Material, sj-xlsx-1-tct-10.1177_1533033821995281 - Diagnostic Value of Vaginal Microecology, Serum miR-18a, and PD-L1 for Identifying HPV-Positive Cervical Cancer
Supplemental Material, sj-xlsx-1-tct-10.1177_1533033821995281 for Diagnostic Value of Vaginal Microecology, Serum miR-18a, and PD-L1 for Identifying HPV-Positive Cervical Cancer by Yumei Zhang, Sujuan Qiu, Yueli Guo, Jiaqin Zhang, Xiaoqing Wu and Guolin Hong in Technology in Cancer Research & Treatment
Footnotes
Abbreviations
Authors’ Note
Yumei Zhang, Sujuan Qiu, and Guolin Hong are co-first authors and contributed equally to this work. The study was approved by the Ethics Committee of our hospital (approval number of the institutional review board: 2016052). All informed consent was obtained from the participants and their family members.
Acknowledgments
This work was supported by the National Natural Science Foundation of China (81772287).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Received financial support from National Natural Science Foundation of China (81772287).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.