
Abstract
Purpose:
Approximately 5%–10% of men who receive prostate cancer radiotherapy will suffer from radiation cystitis. Bladder filling before the administration of radiotherapy results in lower radiation exposure to the bladder. BladderScan, an ultrasound-based bladder volume scanner, has the potential to evaluate bladder volume during radiotherapy; thus, a prospective pilot study was initiated.
Methods:
Eleven men receiving tomotherapy for localized prostate cancer were enrolled. The validity of BladderScan was evaluated by comparing the measurements from BladderScan with the calculated volume from megavoltage computed tomography (MVCT). With a crossover design to compare different methods in bladder filling, the radiotherapy was divided into 2 sequences. Conventional method: the patient was asked to drink water after voiding urine. The amount of water and the duration of waiting were the same as in the setting of the simulation. BladderScan feedback method: the bladder filling procedure depended on the BladderScan measurements.
Results:
There were 314 sets of data from 11 patients. The correlation coefficient between VBS and VCT was 0.87, where VBS is the mean volume of 3 measurements by BladderScan and VCT is the bladder volume derived from MVCT. The BladderScan feedback method resulted in a significant larger bladder volume than the conventional method, with a mean difference of 36.9 mL. When the failure was defined as VCT <80% of planned volume, the BladderScan feedback method brought about a relative reduction in the failure rate with an odds ratio of 0.44 and an absolute reduction of 9.1%.
Conclusion:
The accuracy of BladderScan was validated by MVCT in our study. The BladderScan feedback method can help patients fill the bladder adequately, with a larger bladder volume and a lower failure rate.
Introduction
Radiotherapy is one of the definitive treatments for men with localized prostate cancer. The long-term local control rate with radiotherapy is similar to that obtained with radical surgery. 1 However, approximately 5%–10% of men receiving prostate radiotherapy will suffer from radiation cystitis, a late toxicity that causes intermittent hematuria. 2,3 A way of limiting radiation cystitis is bladder filling before the administration of radiotherapy, which results in less radiation exposure to the bladder. To achieve a reproducible full bladder, the conventional practice consisted of asking the patient to drink the same amount of water and wait for the same duration on each treatment day was adopted. However, the bladder volume varies widely by clinical observations. Thus, a more objective way to reproduce the bladder volume was needed.
Tomotherapy provides megavoltage computed tomography (MVCT) images, on which the physician can see the radiation target and the organs before each treatment. If the bladder filling is poor, the patient is asked to drink more water. However, this procedure is time consuming, and the repeated MVCT leads to more radiation exposure. BladderScan, an ultrasonography-based bladder volume scanner, was originally designed for evaluating residual urine in patients with obstructive uropathy. It has also been utilized in evaluating bladder volume during prostate cancer radiotherapy. 4 -10 In these studies, the bladder volume calculated from the computed tomography (CT) simulation scan was used as the comparative standard to validate the BladderScan measurement, and each patient contributed one set of data. In contrast, when tomotherapy is used for patients with prostate cancer undergoing radiotherapy, at least 20 sets of MVCT scans are acquired during the treatment course. A model that considers both fixed and random effects can be established by collecting more data.
The aim of this study was to produce a sufficient and reproducible bladder volume in prostate cancer radiotherapy. The validity of BladderScan was evaluated by comparing the measurements of BladderScan with the calculated volume from MVCT. Then we hypothesized that the BladderScan feedback method would help patients fill the bladder adequately. Thus, a prospective pilot study with a single-arm crossover design was initiated.
Materials and Methods
From December 1, 2017 to March 31, 2019, eleven men were enrolled in the Far Eastern Memorial Hospital, Taiwan. The inclusion criteria were that patients planned to receive radiotherapy by tomotherapy as the primary definitive treatment for prostate cancer. The patients who had metastatic disease or could not appropriately follow instructions to fill the bladder were excluded. This study was approved by the Institutional Review Board of the Far Eastern Memorial Hospital (106110-E). Written informed consents were obtained from all participating patients.
To achieve a reproducible full bladder, each patient followed the instructions on how to fill the bladder after voiding urine. The protocol was for the patient to drink 400–500 mL of water and wait for about 30 minutes prior to the CT simulation scan. If a larger bladder volume was necessary for an adequate CT simulation, the patient was asked to drink more water prior to the next scan. The total amount of water consumed and the duration of waiting were recorded. Two approaches, BladderScan and CT, were applied to assess bladder volume. BladderScan (BVI 6100, Verathon Medical, Bothell WA, USA) was used to measure the bladder volume before CT. For the procedure, a probe with gel was placed on the patient’s abdomen approximately 3 cm above the symphysis pubis. After scanning, the calculated bladder volume was displayed on a screen. The manufacturer recommended scanning at least 3 times per examination to ensure the highest degree of accuracy. For the reproducibility, we marked the scanning site on the day of simulation. All procedures were performed within 2 minutes by a well-trained radiation therapist. In the CT assessment, a physician delineated the bladder on each CT image. Subsequently, the bladder volume was reconstructed and calculated by the planning system. We considered this value to represent the actual volume of the bladder.
The planning target volume of radiotherapy was created by expanding the prostate volume with 0.5–1.0 cm margin. For patients with higher risk, the seminal vesicles and the pelvic nodal region could be included. Both conventional fractionation (78 Gy in 39 fractions) and hypofractionation (60 Gy in 20 fractions) were permitted. The intensity-modulated radiotherapy plan and radiation delivery were executed by the tomotherapy system. The radiotherapy section for each enrolled patient was divided into 2 sequences by different methods of bladder filling (conventional and BladderScan feedback) after the baseline volume determination (CT simulation) as demonstrated in Figure 1.
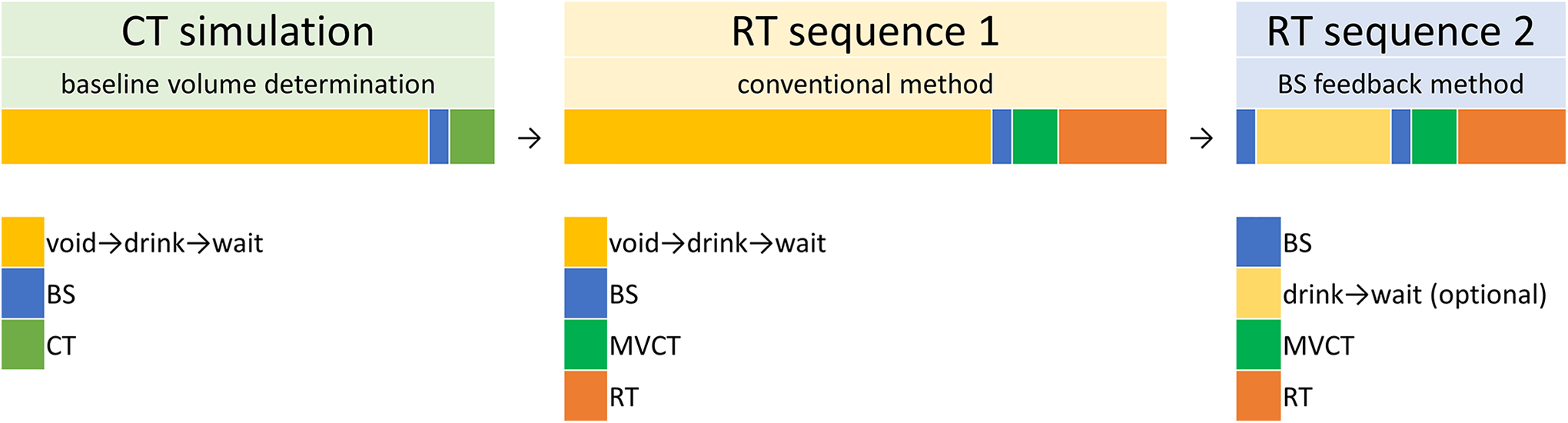
The protocol for the single-arm crossover design. BS, BladderScan; CT, computed tomography; MVCT, megavoltage computed tomography; RT, radiotherapy.
For the first half of the radiotherapy course (i.e., the first 10 of a total 20 fractions, or the first 20 of a total 39 fractions), each patient was assigned to sequence 1 with the conventional method for bladder filling. On each treatment day, the patient was asked to void urine and then drink water. The amount of water and the duration of waiting were the same as in the setting of the CT simulation. BladderScan was subsequently used to collect the data, and the MVCT was applied for image-guidance. After that, the patient received the radiotherapy. For the rest of the radiotherapy course (i.e., from the 11th to the 20th fractions of a total 20 fractions, or from the 21th to the 39th fractions of a total 39 fractions), the patient was assigned to sequence 2 using the BladderScan feedback method. On each treatment day, the patient did not need to void urine before BladderScan was applied, in contrast to sequence 1. The goal was to achieve at least 80% of the volume measured by BladderScan on the day of CT simulation. If the measurement was <80%, the patient would be asked to fill the bladder and then repeat the BladderScan procedure about 30 minutes later until 80% of volume was achieved. The patient subsequently underwent MVCT and radiotherapy.
The bladder volume assessed in each fraction of radiotherapy was measured by BladderScan and the MVCT and represented by VBS and VCT, respectively. VBS was the mean volume of 3 records by BladderScan before MVCT. The difference of the records per examination should be within 10%. VCT was derived from the reconstructed CT images as mentioned previously, and is considered as the actual bladder volume. A binary outcome has been defined whether the bladder filling procedure was acceptable. On each treatment day, if VCT was <80% of the planned volume, the bladder filling was defined as a “failure.”
Because of the repeated-measures study design in comparing the 2 approaches for the determination of bladder volume, a linear mixed model was applied with the fixed effect depicting VBS compared with VCT and the random effect capturing the baseline heterogeneity for each subject.

where
To assess the effect of introducing BladderScan in patients with an adequately full bladder, we compared VCT in each fraction between the conventional and BladderScan feedback methods using another liner mixed model. With regard to the evaluation in bladder filling by the 2 methods, in terms of a predefined binary outcome, a generalized linear mixed model using the logit link was applied. Statistical analyses were performed using the SAS software. A p-value of <0.05 denoted statistical significance.
Results
Characteristics of Enrolled Subjects
The patient characteristics are summarized in Table 1. Only 3 patients were in low or intermediate risk group. For most of the patients, the radiotherapy field included only the prostate, and androgen deprivation therapy was delivered concurrently. On the day of CT simulation, the mean amount of water consumed by patients for bladder filling was 482 mL, and patients waited an average of 35 minutes before imaging. The mean bladder volume reconstructed on the simulated CT scan was 151 mL. The patients then received fractionated radiotherapy by tomotherapy. Each patient received fractionated radiotherapy and contributed at least 20 sets of VBS and VCT data.
Patient Characteristics.

ADT, androgen deprivation therapy; BMI, body mass index; PSA, prostate-specific antigen; RT, radiotherapy.
Validation of the BladderScan Measurement
After excluding 2 sets of missing data, there were 314 sets of data from 11 patients. Figure 2 shows the distribution and correlation between VBS and VCT. The average bladder volumes as assessed via MVCT and BladderScan were 167.9 mL and 176.8 mL, respectively. The variation of VBS (

Linear correlation between VBS and VCT. “id” refers to patient number. VBS, measurements by BladderScan. VCT, bladder volume derived from the MVCT. There was a positive correlation between VBS and VCT.
Table 2 shows the estimated results for the correlation between VBS and VCT using the linear mixed model. The correlation represented by the slope parameter was estimated as 0.65 (95% CI = 0.60–0.69). The estimated results revealed a positive linear correlation of the bladder volume measurement between BladderScan and MVCT. While the baseline variation was estimated as 53 mL (95% CI = 39–68 mL), there was significant heterogeneity across subjects (
Correlation Between VBS and VCT Using a Linear Mixed Model.

VBS, mean volume of 3 records by BladderScan; VCT, bladder volume derived from the MVCT.
Comparison Between Conventional Method and BladderScan Feedback Method in Bladder Filling
To assess the effect of introducing BladderScan measurement on adequately full bladder, we compared VCT between the conventional method in sequence 1 and the BladderScan feedback method in sequence 2. Figure 3 is the boxplot of VCT using the 2 methods for filling bladder, subgrouped by each patient. The average VCT was 150 mL with the conventional method. There was an increasement of 36.9 mL (95% CI = 24.5–49.3 mL) with the BladderScan feedback method (Table 3). However, when the baseline bladder volume was <120 mL, the effect was obscure.

Bladder volume boxplot, constructed with the conventional and BladderScan feedback methods for bladder filling. “id” refers to patient number. VCT, bladder volume derived from megavoltage computed tomography. Sequence 1, with conventional method. Sequence 2, with BladderScan feedback method. The BladderScan feedback method resulted in a larger bladder volume.
Comparison Between Conventional Method and BladderScan Feedback Method in Bladder Filling.

VCT, bladder volume derived from megavoltage computed tomography.
We also evaluated the bladder filling based on a predefined binary outcome. When the failure was defined as VCT <80% of the planned volume, the estimated failure rate was 16% and 7% in each sequence, respectively (Table 3). The BladderScan feedback method resulted in a relative reduction in the failure rate with an odds ratio of 0.44 (95% CI = 0.19–0.72) and an absolute reduction of 9.1% (95% CI = 0.2–19.9%).
Time Needed to Reach an Adequate Bladder Volume
The clinical utility of BladderScan was further explored by comparing data for the time needed to reach an adequate bladder volume before daily radiotherapy. Note that in sequence 1 (conventional method), the patients had to wait for the same length of time as observed for the setting of the CT simulation, whereas in sequence 2 (BladderScan feedback method), the bladder filling procedure depended on the BladderScan measurements. If the bladder volume was adequate, the radiotherapy could be immediately administered. In sequence 2, patients had to drink more water in only 22% (35/156) of the treatment fractions. The BladderScan feedback method resulted in a reduction of mean waiting time from 36 (range: 20–60) minutes to 6 (range: 0–73) minutes.
Discussion
Although only 11 patients were included in our study, more than 300 sets of MVCT images were derived from daily treatment. This is the largest data set to access the accuracy of BladderScan in prostate radiotherapy. Results of other published studies revealed a positive correlation between the BladderScan measurement and the reconstructed bladder volume on CT images, with Pearson’s correlation coefficients ranging from 0.80 to 0.95. 4 -10 In our study, we applied a random effects model to capture the correlated data structure for the repeated-measures design. The estimated correlation coefficient of 0.87 was in line with these previous findings, thereby supporting BladderScan as a valid tool for measuring bladder volume.
A significant positive correlation was noted between VCT and VBS from the linear mixed model. As a perfect measuring tool, the linear correlation should reflect VCT = VBS. The slope parameter of 0.65 indicated an inflated standard deviation of VBS, which may have originated from a heterogeneous process in applying the BladderScan approach. The radiotherapy course lasted for 1–2 months in our study. Thus, fewer than 4 therapists would have operated the equipment for each patient. Unfortunately, we did not evaluate the inter-observer variability in our study design. However, results of other studies have shown that the interoperator variability of BladderScan was 11.3% and that the repeatability was not affected by the size of the bladder volume. 5,6 The characteristics of the subjects, such as body mass index, may have an effect on the accuracy of BladderScan measurements, but we did not find the significance with limited case numbers. In linear correlation, some outliers may affect the slope significantly. The VBS of most points on the Figure 2 ranges from 100 to 200 mL. Within this range, the BladderScan can predict the bladder volume more accurately.
In our study, through a crossover design, the BladderScan feedback method resulted in a larger bladder volume and a lower failure rate compared to the conventional method. We arbitrarily defined “failure” in bladder filling as VCT <80% of the planned volume. This concept was originally presented in another study, 9 in which the failure was defined as “less than 50% or too large.” However, we considered 50% too low a cutoff value; instead, we used 80% for both VBS and VCT. When assessing the VCT by delineating the bladder, we found that the position of the prostate did not vary significantly with the bladder size. A larger bladder size would have resulted in a lower percentage of irradiated bladder volume, without affecting tumor control. Thus, we did not define an upper limit for bladder volume.
Two studies have addressed whether the application of BladderScan improved the procedure of bladder filling. 5,9 Stam et al used a biofeedback protocol to provide daily bladder volume information to patients and drinking advice on the next treatment day instead of providing instant feedback. They concluded that the biofeedback method did not substantially reduce the variation of bladder volume. 5 Cramp et al found that the BladderScan method for bladder filling was useful in achieving a consistent, appropriately sized bladder volume by accessing the passing rate of bladder requirements. 9 In both studies, the patients were not randomly assigned into 2 groups. With limited number of cases, the data did not indicate whether variations in compliance or bladder capacity among patients affected the outcome. A crossover design to compare the different methods of bladder filling in individual patients could diminish these variations.
In general, a randomized controlled crossover design with 2 arms is preferred because the time may be a confounding factor of the outcome. In fact, Stam et al found that bladder volume decreased over time during irradiation; it decreased by up to 31% without manipulation during the latter part of the radiotherapy course. 5 There were 2 reasons for using a single-arm design in our study. First, most of the prostate cancer patients were elderly. The trial design was simplified to facilitate the enrollment and execution. Second, while the BladderScan feedback method was used in sequence 2, in which the bladder volume would decrease without manipulation, and the results were still positive, the benefit of this method should be convincible.
The BladderScan feedback method could save time in filling the bladder and provide potential benefits. For example, magnetic resonance-guided radiation therapy (MRgRT) has been developed in recent years and features real-time imaging without additional radiation doses and has online adaptive capabilities. 11 MRgRT is therefore an ideal tool to evaluate the bladder size and modify the treatment plan in prostate radiotherapy. Although the MRgRT can aid in recontouring and replanning, a bladder that fills poorly will receive more radiation exposure. Besides, MRgRT is high-priced, and any delay in treatment increases the cost. If a patient has to control the bladder size, BladderScan is useful as a first-line screening tool. The procedure lasts only 2 minutes, which is much shorter than the time needed for MR scanning and replanning.
This study had some limitations. First, we attempted to determine the bladder-filling kinetics initially. However, these characteristics vary widely day by day, as in the conventional method mentioned in the manuscript. An individualized drinking protocol is difficult to establish. Second, we did not use an objective score to assess each patient’s lower urinary tract symptoms. Such symptoms include problems with voiding (e.g., hesitancy, straining, and dribbling) and storage (e.g., frequency, urgency, and nocturia), 12 which are related to the function of bladder filling. Third, this pilot study included only 11 patients, and the regression model was simple. Thus, we cannot predict whose measurement of BladderScan is less accurate. However, for the purpose of bladder filling assistance, BladderScan does not require extreme precision.
Conclusions
Our study confirmed that BladderScan is effective for patients receiving prostate radiotherapy in bladder filling. The accuracy of BladderScan was validated by MVCT images with repeated measurements study design. The BladderScan feedback method would help patients to fill the bladder adequately, with a larger bladder volume and a lower failure rate. The potential of improving the treatment quality and process by reducing the percentage of irradiated bladder volume and the waiting time of patients can be expected.
Supplemental Material
Supplemental Material, sj-pdf-1-tct-10.1177_1533033821995277 - BladderScan Feedback Method in Predicting Bladder Filling for Prostate Radiotherapy: A Prospective Study
Supplemental Material, sj-pdf-1-tct-10.1177_1533033821995277 for BladderScan Feedback Method in Predicting Bladder Filling for Prostate Radiotherapy: A Prospective Study by Deng-Yu Kuo, Chen-Yang Hsu, Wei-Chun Wang, Hsiu-Hsi Chen and Pei-Wei Shueng in Technology in Cancer Research & Treatment
Footnotes
Abbreviations
Acknowledgments
We thank Prof. Yen, Ming-Fang for the advice regarding the study design and Enago’s editorial support in this paper.
Ethics
The study was approved by the Far Eastern Memorial Hospital for ethical approval (approval no. 106110-E). Written informed consents were obtained from all participating patients.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported in part by Far Eastern Memorial Hospital grants (FEMH-2018-C-054).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.