
Abstract
Keywords
Background
Breast cancer treatment is a comprehensive treatment, in which radiotherapy is a key link in the treatment of early breast cancer. Studies have shown that adjuvant radiotherapy (RT) for early breast cancer patients after breast-conserving surgery (BCS) has the same local control rate and overall survival rate as simple radical mastectomy, but the cosmetic outcomes were better. 1
Commonly, the RT regime after BCS is conventional fractionation (CF) whole breast irradiation (WBI): WBI ± integrated boost. However, the unconventional fraction has become the main research topic in the field of RT, due to some patients with poor clinical compliance, CF WBI with long and frequency RT, high medical cost, and the continuous progress of breast cancer radiobiology research. The Standardization of Breast Radiotherapy (START) trials confirmed that lower total doses of radiotherapy delivered in fewer, larger doses (fractions) did not compromise safety and efficacy.2,3 Hypofractionated whole breast irradiation and intraoperative electron radiotherapy are large doses per fraction methods in breast cancer RT. 4 At present, there is no unified consensus on the dose and timing of tumor bed boost after WBI. In 2011, ASTRO pointed out that there was almost no data to clarify those patients receiving tumor bed boost had serious toxic reactions. When there was an indication for tumor bed boost, HF WBI alone was not appropriate, but the doses (fractions) for HF and tumor bed were not definite. 5 Therefore, some studies put forward conventional fractionation simultaneous integrated boost (CF-SIB) and hypofractionated simultaneous integrated boost (HF-SIB) RT models. Some trials have proved the efficacy of CF-SIB: 1.8 Gy × 28 fractions to the whole breast with 2.15 Gy/f SIB to the tumor bed. 6 Nowadays, hypofractionated whole-breast irradiation is the standard of care in the management of patients with early breast cancer. However, Ratosa et al 7 showed that half of the patients with breast cancer are treating conventionally in Europe. The course of CF-SIB RT usually takes several weeks, hence HF-SIB regimens should be considered during the COVID-19 epidemic pandemic in order to reduce treatment duration and minimize the risk of infection. But HF-SIB RT models were rarely reported.
Furthermore, Chadha et al 8 revealed that patients receiving HF-SIB RT had a lower incidence of ≥ grade 2 skin toxicity (P = .0015) and breast pain compared with patients receiving CF RT. No significant difference in the incidence of breast edema or hematologic adverse outcomes was observed between the 2 groups. However, HF-SIB RT has not yet been clinically promoted, because reports on HF-SIB after BCS are few, and the acute and late toxicity and adverse cosmetic outcomes after RT have not yet reached unanimous recognition.
In this study, clinical experience of HF-SIB, compared with the CF, in breast cancer patients after BCS with emphasis on skin toxicity, myelosuppression, radiation pneumonia, and cosmetic outcomes were being presented. This is the first retrospective double-arm report on HF-SIB in China.
Methods
Patients
Between May 2015 and July 2019, 185 patients with early breast cancer receiving RT after BCS at Shandong First Medical University Affiliated Cancer Hospital were enrolled in this retrospective cohort study.
Inclusion criteria: (1) age > 18 years, female, Karnofsky performance status (KPS) ≥ 70%; (2) operation method: BCS + axillary lymph node dissection (ALND) or sentinel lymph node biopsy (SLNB); 5 to 10 silver clips; negative Pathological resection margin and safety margin ≥ 2 mm; no lymph node envelope invasion, no vascular tumor thrombus; (3) TNM: pTis-2, pN0 to 1, M0 (AJCC6 and UICC jointly developed); (4) Postoperative pathology: invasive carcinoma. Exclusion criteria: bilateral breast cancer, recurrent breast cancer, inflammatory breast cancer, multifocal breast cancer, merging with other malignant tumors or severe medical diseases, history of chest RT.
According to different dose-fractionation, the patients were divided into HF-SIB group (104 patients) and CF group (81 patients). Patient general characteristics are described in Table 1. The retrospective study was approved by the Shandong First Medical University Affiliated Cancer Hospital Ethics Committee (the committee's reference number: SDTHEC2021009003). Informed consent was exempted by the board due to the retrospective nature of this research. All methods were performed in accordance with the relevant guidelines and regulations. Patient records were anonymized and de-identified before analysis of the data.
Patients and Treatment Characteristics.

Abbreviation: ER, estrogen receptor; HER-2, human epidermal growth factor receptor 2; PR, progesterone receptor.
Radiotherapy
All patients signed the informed consent form for RT. Then, the BrillianceTM Big Bore CT (Philips, the Netherlands) was used to scan from the cricothyroid membrane to the lower edge of the lung, when the patients lied on the breast bracket in supine or prone position (CIVCO HorizonTM breast bracket special used in prone position). The images were transferred to Eclipse Treatment Planning System (Varian Medical Systems, USA) to contour target volumes and organs at risks (OARs) according to RGOT Guideline. Specifically, clinical target volume (CTV) included the soft tissues of the whole breast down to the deep fascia, gross target volume (GTV) referenced surgical clips, seroma, imaging of preoperative MRI, postoperative positioning CT, and surgical scar. PTV-high was delineated by uniform margins of 15 mm around the GTV.
Both groups used 6-MV X-rays and adopted fixed-jaw intensity-modulated radiotherapy (IMRT). HF-SIB included 104 patients and the dose of whole-breast radiation reached 42.56 Gy in 16 fractions and simultaneously tumor bed boost to 48 Gy in 16 fractions, which course of radiotherapy was 22 days. The 81 patients of the CF group received whole breast radiation to 50 Gy in 25 fractions and followed by tumor bed boost to 10 Gy in 5 fractions, which course of radiotherapy was 40 days.
Dose limiting of OARs: ipsilateral lung: Dmean < l0 Gy, V20 < 30%, V5 < 55%; contralateral lung: V5 < 5%; heart (left breast cancer): Dmean < 5 Gy, V30 < 10%,V40 < 5%; spinal cord: Dmax < l0 Gy; contralateral breast: Dmean < l Gy. Quantitative evaluation of plans was performed by dose volume histogram (DVH).
The RT was carried out once a day from Monday to Friday every week by Clinic Vital Beam linear accelerator (Varian, USA) in Shandong First Medical University Affiliated Cancer Hospital and verified by cone-beam Computer Tomography (CBCT).
Outcome Assessment
Local recurrence was defined as recurrence of the ipsilateral breast and/or lymphatic recurrence in the ipsilateral internal breast, supraclavicular and axillary regions. Distant metastasis was defined as any new lesions outside of the above-mentioned site. Disease-free survival (DFS) was defined as the time from the end of RT to local recurrence or distant metastasis, or death from any causes. Overall survival (OS), the study endpoint, started from the end of RT to death or last available follow-up.
Both acute (within 3 months from the start of RT to the end) and late (from 3 months after the end of RT to the end of follow-up) toxicities were assessed. Hematological toxicity, radiation skin toxicity, and radiation lung injury were scored according to the Radiation Therapy Oncology Group (RTOG)/European Organization for Research on Treatment of Cancer (EORTC) radiation morbidity scoring system. 9 Cosmetic outcomes at 6 months and 2 years after radiotherapy were noted according to the Harris criterion.
According to age, chemotherapy, position method, we divided patients of the HF-SIB group into different groups: ≤ 50 years old and > 50 years old, chemotherapy and nonchemotherapy, supine position, and prone position. The CTV excluding the upper and lower clavicle area is the breast volumes. The breast volume of the HF-SIB group was divided into 3 levels ranging from 180 to 1011 cc.
Follow-up
During the RT period, the outpatient consultation, physical examination, and blood routine examination were conducted to evaluate acute adverse reactions weekly. After the RT, the outpatient review was performed every 3 months for the first 2 years, and once every 6 months since the third year.
Statistical Analysis
The recorded indexes were analyzed by SPSS 26.0 software. Rank sum test and chi-square test were used to evaluate adverse reactions and cosmetic outcomes. Spearman rank correlation analysis was used to evaluate the correlation between breast volume and adverse reactions. In all cases, statistical significance was considered for P < .05. The reporting of this study conforms to STROBE guidelines. 10
Results
As of February 2020, all patients have completed the follow-up, and no cases were lost to follow-up. Among 81 patients of CF, there were 2 recurrences within 2 years, 1 supraclavicular lymph node recurrence, and 1 internal mammary lymph node recurrence. All the above 2 patients have received salvage treatment. The 2-year survival rate was 100% (81 of 81), and the 2-year recurrence rate was 2.2% (2 of 81). 2 patients of the HF-SIB group were diagnosed with leukemia, the second primary malignant tumor, 11 months after the end of RT. They were still receiving chemotherapy at the local hematology department until the end of follow-up. Statistically, until the end of the follow-up, the survival rate and recurrence rate were 100% (104 of 104) and 0% (0 of 104). There were 80 patients of the HF-SIB group and 81 patients of the CF group who were followed up for 2 years. The 1-year survival rate of both groups was 100%, and no recurrence cases within 1 year (0 of 104, 0 of 81). Maximum adverse reaction grades are listed in Table 2, cosmetic outcomes are listed in Table 3. Because 24 patients in the HF-SIB group did not reach the 2-year follow-up period, only 80 patients were evaluated for their cosmetic outcomes 2 years after radiotherapy.
Maximum Adverse Reaction Grades of HF-SIB Group and CF Group.

There was no grade 3/4 late skin reaction in both groups.
Cosmetic Effects of HF-SIB Group and CF Group 6 Months and 2 Years After RT.

Because 24 patients in the HF-SIB group did not reach the 2-year follow-up period, only 80 patients were evaluated for their cosmetic effects 2 years after radiotherapy.
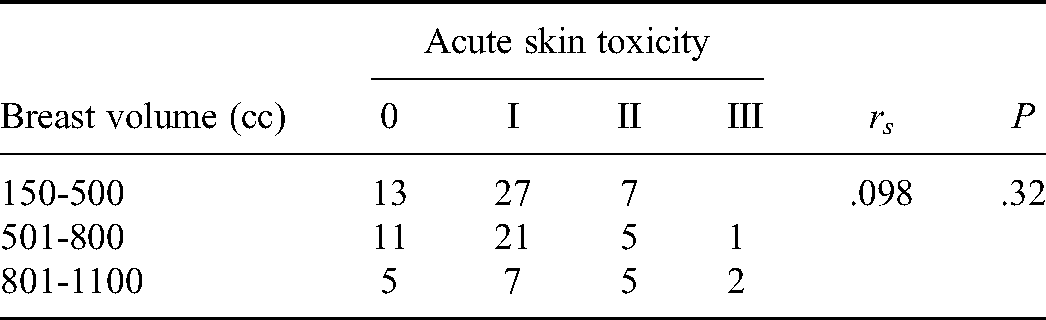
The incidence of acute skin toxicity of grade 0 to 1 in the HF-SIB group was 81.7%, the symptoms were breast swelling, skin redness, increased skin temperature, and hyperpigmentation; that of grade 0 to 1 in the CF group was 70.4% and the symptoms of grade 2 were flaky wet peeling of breast. For late skin toxicity, the incidence of the HF-SIB group was higher than that of the CF group. There was no statistical difference (P > .05, rank-sum test) in acute and late skin toxicity between the 2 groups. And age, chemotherapy, and position were not statistically significant for acute and late skin toxicity. Moreover, Spearman rank correlation analysis revealed breast volume was not correlated with acute (rs = .098, P = .32) (Table 4) and late skin toxicity.
Breast Volume and Acute Skin Toxicity of HF-SIB Group.
During RT, a blood routine examination was done once a week to record the maximum grade of myelosuppression. Grade 1, Grade 2, and Grade 3 myelosuppression in the HF-SIB group accounted for 16.3%, 12.5%, and 3.8%, respectively, which were less than 29.6%, 21%, and 13.6% of the CF group, and there was no grade 4 in each group. In-hospital patients with myelosuppression were treated with leukocyte-raising drugs in time, and it was controlled at Grade 0 to 1 out of hospital. Significant differences were observed between HF-SIB and CF for myelosuppression (P = .00) (Table 5). In other words, the HF-SIB group showed lower blood toxicity. Further analysis of the factors affecting blood toxicity of the HF-SIB group found that chemotherapy was a crucial factor (P = .045) (Table 6).
Myelosuppression of HF-SIB Group and CF Group.

Chemotherapy for Myelosuppression of HF-SIB Group.

This study evaluated the cosmetic outcomes of all patients at 6 months and 2 years after RT according to the Harris criterion. The 2 groups had no statistical difference in the excellent and good rate (x26 months = 0.254, x22 years = 0.451). And analysis found that chemotherapy (P = .732), and breast volume (P = .397) were not associated with cosmetic outcomes.
We found that the incidence of acute skin reactions was 74.4% in the supine position, which was higher than the 65.4% in the prone position. At the same time, the results showed that the excellent and good rate in the prone position 2 years after radiotherapy was equivalent to that in the supine position (93.4% vs 89.5%).
The incidence of grade 0 to 1 and grade 2 to 3 radiation pneumonia of the HF-SIB group was6.2% and 3.8%, while that of the CF group was 98.8% and 1.2%, respectively. There was no statistical difference in radiation pneumonia between the 2 groups.
Discussion
During the COVID-19 pandemic, the HF-SIB RT in our study reduced the exposure time of patients in the hospital by half compared with CF RT. This greatly reduces the harm caused by patients who fail to receive timely oncology treatments due to fear of contracting COVID-19. 11 Furthermore, many clinical studies have confirmed that normal breast tissue does not increase tissue damage under the same equivalent biological dose irradiation and the recommended fraction dose was > 2 Gy. In the past 20 years, more than 2000 female patients participated several HF versus CF trials: START-A trial, 12 START-B trial, 13 RMH/GOC trial, 14 and ONTARIO trial. 15 The long-term results of these trials showed that the 2 treatment groups have similar curative outcomes for 10 years and the local regional recurrence rate, which largely confirmed the safety and effectiveness of the 13 to 16 fractions in 3 to 4 weeks.
Van Parijs et al 16 recently reported the feasibility study of HF-SIB in 70 patients with stage I to II breast cancer. The above studies confirmed that HF-SIB was not significantly inferior to CF in terms of survival benefit and treatment effect. However, the ASTRO meeting in 2018 recommended that the tumor bed boost should base on the clinical indications (stage/histology, age, grade, margins, ER/PR/HER2-neu status, and dose fractionation for WBI) and were independent of WBI which might be due to the lack of large multicenter randomized clinical studies that demonstrate the advantages of HF-SIB. Our study explored the incidence and influencing factors of adverse reactions between HF-SIB and CF, which indicated the incidence of myelosuppression was lower in the HF-SIB group, but others were similar.
At present, the supine position is still the most commonly used position, which allows the breast, chest wall and lymph nodes to be irradiated. However, we could not guarantee the absolute repeatability of patients’ positioning between the CT and the treatment table or between each fraction of irradiation, especially for patients with large pendulous breasts. Therefore, Lakosi et al 17 put forward that prone position improved the reproduction of position and target area to reduce the movements of respiration related surgical clip and chest wall. In recent years, many trials claimed that the cardioprotective effects of the prone position of large breasts after BCS were equivalent to or even better than that of the supine position.18,19 Moreover, a higher risk (relative risk = 2.59) of secondary lung malignancies was predicted for supine breast irradiation when compared with prone breast irradiation no matter in CF or HF. The statistics of our study were similar to the results of the above study: acute skin toxicity rates were lower with the Prone position compared to the Supine position (64.4% vs 74.4%). Although this study did not conduct a dosimetric analysis of OARs and the number of cases was limited in terms of the different adverse reactions, the advantages of the prone position could be reflected. All in all, whether it is short-term or long-term toxicity, the treatment effects of prone position were not inferior to that of the supine position, or even better.
Most studies used sequential boost after hyperfractionated RT, but few simultaneous boosts. Among the simultaneous boost studies, most similarly concluded that the HF-SIB group has a lower incidence of skin toxicity and satisfactory cosmetic outcomes.8,20-22 The 2-year results of our trial concluded that no impact had been seen so far in skin toxicity or cosmetic outcomes between the HF-SIB group and the CF group. Therefore, HF-SIB not only provided a higher dose/distillate on the basis of simultaneous tumor bed boost, but also did not increase acute skin toxicity. A study with a median follow-up time of 45 months also confirmed that HF-SIB RT had very low late skin toxicity: only grade 1 skin toxicity was recorded. 23
In our study, we demonstrated that chemotherapy aggravated myelosuppression (P = .000). The National Comprehensive Cancer Network (NCCN) guidelines also considered receiving RT and chemotherapy as risk factors for neutropenic fever.24,25 In terms of skin toxicity and cosmetic outcomes, De Santis et al 26 found that chemotherapy impacted late fibrosis at univariate analysis (P = .04). Analogously, Kouloulias et al 27 analyzed 116 patients treated with HF RT, of which 33 underwent adjuvant chemotherapy, which found chemotherapy aggravated the development of skin toxicity but without critical difference at univariate analysis. Our study also reached the same conclusion: adjuvant chemotherapy had no significant effect on acute skin toxicity (P = .609), late skin toxicity (P = .758), and cosmetic outcomes (P = .538).
According to reports, large volume breasts were related to the occurrence of acute reactions. The dates displayed that the maximum dose of large volume breasts was 7% higher than the prescribed dose, which resulted in dose inhomogeneity. In univariate analyses, larger breast volumes were frequently associated with the development of acute skin toxicities (P = 0004) and in the multivariate analysis, larger breast target volume had a significant influence on higher grade skin toxicity (P = .003). 28 The same results were confirmed in another study, which observed the acute skin toxicity of intensity-modulated radiation therapy (IMRT) and CF RT. Stepwise logistic regression analysis showed that breast size (P < .0001) was significant predictor of moist desquamation. Specifically, small and large breast sizes might have lower desquamation with IMRT than medium sizes. 29 However, there is no consensus on breast sizes at present: different studies had different standards for dividing breast volume. In the present study, the breast size of the HF-SIB group was divided into 3 grades ranging from 180 to 1011 cc. Spearman rank correlation analysis did not get similar positive results: it had nothing to do with skin toxicity and cosmetic outcomes. However, the breast volume of the enrolled group was mainly concentrated in less than 800 cc (82%), and there were only 19 cases (18%) of large breasts. The sample size of large breasts was small, which was prone to errors.
This study also had some limitations. First, although there was no significant difference in baseline characteristics of patients between groups, selection bias in our population is inevitable due to the nature of retrospective studies. Second, there were a limited sample size and a short follow-up period in both groups. In future studies, prospective randomized trial with a larger sample size of patients and a longer follow-up period is needed to obtain more evidence and support for data on this page.
Conclusion
The results of this trial help determine the real impact of HF-SIB for breast cancer patients after BCS, but we need to extend follow-up time and expand the sample size before long-term outcomes are obtained. Meanwhile, the use of HF-SIB RT to breast cancer patients after BCS may be considered to be a valuable choice and should be recommended to suitable candidates during the COVID-19 epidemic.
Footnotes
Abbreviations
Ethics Statement
The study was approved by the Shandong First Medical University Affiliated Cancer Hospital Ethics Committee (the committee's reference number: SDTHEC2021009003). Informed consent was exempted by the board due to the retrospective nature of this research. All methods were performed in accordance with the relevant guidelines and regulations. Patient records were anonymized and de-identified before analysis of the data.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China (81773232); the Academic Promotion Program of Shandong First Medical University (Shandong Academy of Medical Sciences)(2020RC002); and the Project of Young Taishan Scholars (Tsqn201909187); the Wu Jieping Medical Foundation (320.6750.2021-01-11).