
Abstract
Keywords
Introduction
Hepatocellular carcinoma (HCC) is one of the deadliest diseases, ranking as the sixth most common cancer and the fourth leading cause of tumor-related death. 1 The mortality rates have increased over recent decades in many countries, especially in China, which accounts for over half of new cases and deaths worldwide. 2 Recently, some improvements are achieved owing to the progress of the treatments, such as surgical resection, liver transplantation, and transarterial chemoembolization. 3 However, the 5-year cause-specific survival rate of HCC remains less than 20% for all stages combined diagnosed, at a low level in human cancers. 4 The main reasons for the poor outcome include difficulties in early diagnosis, rapid progression of advanced liver cancer, and deficiency in practical prognostic assessment. 5 Thus, risk stratification is critical to improving overall survival (OS), particularly in high-risk HCC patients.
Platelet (PLT) characteristics are important inflammatory parameters, and platelets are also associated with the development, invasion, metastasis, and recurrence of cancer. 6 Some platelet-based measures such as platelet count, mean platelet volume (MPV), platelet distribution width (PDW), and platelet-to-lymphocyte ratio (PLR) were significantly associated with the prognosis of HCC patients,7,8 although their roles in predicting survival outcomes are still controversial. Taking platelet count as an example, some studies demonstrated that thrombocytopenia was strongly associated with improved survival, 9 while others showed that preoperative thrombocytopenia was a negative predictor of OS. 10 Besides, some new hematologic markers combining liver function and platelet function have been paid considerable attention. Gamma-glutamyl transpeptidase-to-platelet ratio (GPR) and alkaline phosphatase-to-platelet ratio (APPR) could be auxiliary diagnostic indicators to improve early detection of HCC. 11
In the study, the prognostic significance of these platelet-related indices was systematically evaluated for predicting the survival of HCC patients after surgical resection.
Methods
Study Population and Study Design
A total of 337 HCC patients with hepatectomy were recruited consecutively in the cohort study from May 2013 to January 2014. HCC patients with diabetes were not included in this cohort because diabetes is associated with poor OS and disease-free survival per se, and it has a significant impact on platelet counts and platelet-based parameters. 12 Patients were included if meeting all the following criteria: (1) pathological diagnosis of HCC without distant metastasis; (2) complete clinical, pathological and surgical data; and (3) no previous anticancer treatment with chemotherapy and radiofrequency ablation before surgery; Simultaneously, patients were excluded if not meeting any of the above criteria from analyses to account for bias. Ultimately, 279 patients (median age 51, range:19-81years) were included and analyzed in the retrospective study. The Medical Ethics Committee of our institute approved this study. The written informed consent following the Declaration of Helsinki was provided to all patients and we have de-identified all patient details. The reporting of this study conforms to STROBE guidelines. 13
Follow-up
All the participants were followed-up by outpatient visits. The routine reexaminations included liver function, alpha-fetoprotein (AFP), abdominal ultrasound, and enhanced computed tomography (CT) or magnetic resonance imaging (MRI). Overall survival (OS) was defined as the months from the date of surgery to the time of death or last follow-up. The follow-up was ended in September 2017 for this cohort.
Data Acquisition and Definitions
The clinical features, including age, hepatitis, cirrhosis, antiviral therapy, tumor size, tumor markers (such as AFP, CEA, and CA199), tumor numbers, microvascular invasion, etc., were obtained from the medical records of the patients.
Hematologic and liver function parameters, including platelet count, lymphocyte count, serum gamma-glutamyl transpeptidase (GGT), alkaline phosphatase (ALP), and albumin levels were obtained within three days before surgery. The data from these parameters were used to calculate platelet-related indices: platelet to lymphocytes ratio (PLR), GGT to platelet ratio (GPR), and ALP to platelet ratio (APPR). Also, The prognostic nutritional index (PNI) was calculated with the formula: serum albumin level (g/L) + 5 × total lymphocyte count (10 9 /L), as previously reported. 14 Coagulation markers, prothrombin time (PT), activated partial thromboplastin time (APTT), thrombin time (TT), and fibrinogen (FIB) were also analyzed in the cohort.
Statistical Analysis
All statistical analyses were performed using SPSS statistics 22 (IBM SPSS, Inc., USA). Continuous data were expressed as mean (SD) or median (interquartile range), and the Student's t-test or the nonparametric Mann–Whitney test were used for statistical analyses. Categorical variables were presented as numbers (n) and proportions (%) of patients. The chi-square tests or Fisher's exact tests were used for statistical analyses. The correlation between the platelet-related parameters and clinical features was assessed using the Pearson's or Spearman's correlation coefficients. Receiver operating characteristic (ROC) analyses were performed to determine the optimal cut-off point for these parameters. Cumulative survival rates were estimated by the Kaplan-Meier method. Univariable and multivariable Cox regression analyses were performed to identify prognostic factors associated with OS. Propensity score matching analysis in a 1:2 ratio was employed to reduce the confounding effect of tumor-related factors affecting prognostic survival. A P-value < .05 was considered statistically significant.
Results
Association of Platelet-Related Measures with Clinical Characteristics
A total of 279 from 337 HCC patients received surgical resection were enrolled in this cohort with the exclusion of 2 patients with previous treatment, 3 with distant metastasis, 32 with lost to follow-up, and 21 with missing preoperative hematologic parameters data. The baseline clinical characteristics of patients were summarized in Table 1. A total of 225 patients (80.6%) had viral hepatitis, and 259 (92.8%) developed cirrhosis. Increased AFP levels (≥100 μg/L) were observed in 131 patients (47.0%), and the mean diameter of the greatest tumor was 7.6 cm.
Comparison of Clinical Characteristics of Patients Stratified by the Level of Different in Platelet-Related Measures.
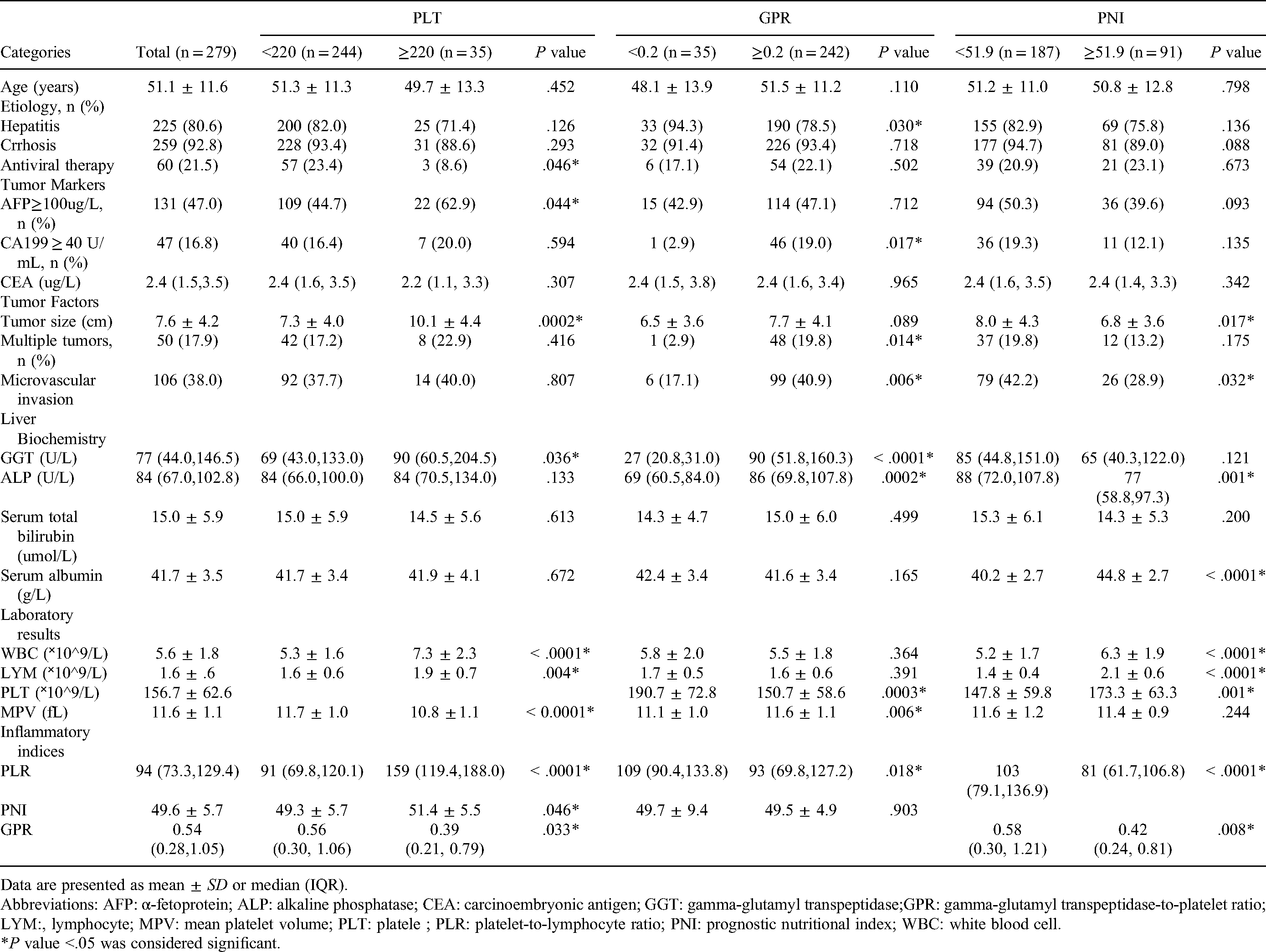
Data are presented as mean ± SD or median (IQR).
Abbreviations: AFP: α-fetoprotein; ALP: alkaline phosphatase; CEA: carcinoembryonic antigen; GGT: gamma-glutamyl transpeptidase;GPR: gamma-glutamyl transpeptidase-to-platelet ratio; LYM:, lymphocyte; MPV: mean platelet volume; PLT: platele ; PLR: platelet-to-lymphocyte ratio; PNI: prognostic nutritional index; WBC: white blood cell.
*P value <.05 was considered significant.
Patients were divided into two groups, the low-PLT and high-PLT group to observe the association of platelet count with the clinicopathologic features. The cut-off point was determined for PLT (220 × 109/L) by the ROC plot. As shown in Tables 1 and 2, a significantly larger diameter of the tumor, more white blood cell (WBC) count, higher PLR and PNI were observed in patients with high-PLT. PLT count was also significantly correlated with WBC count (r = 0.609, P < .0001) and PLR (r = 0.576, P < .0001), and negatively correlated with MPV (r = -0.485, P < .0001) and PDW (r = -0.491, P < .0001).
Correlation of Hematologic Parameters with the Main Characteristics of Patients.
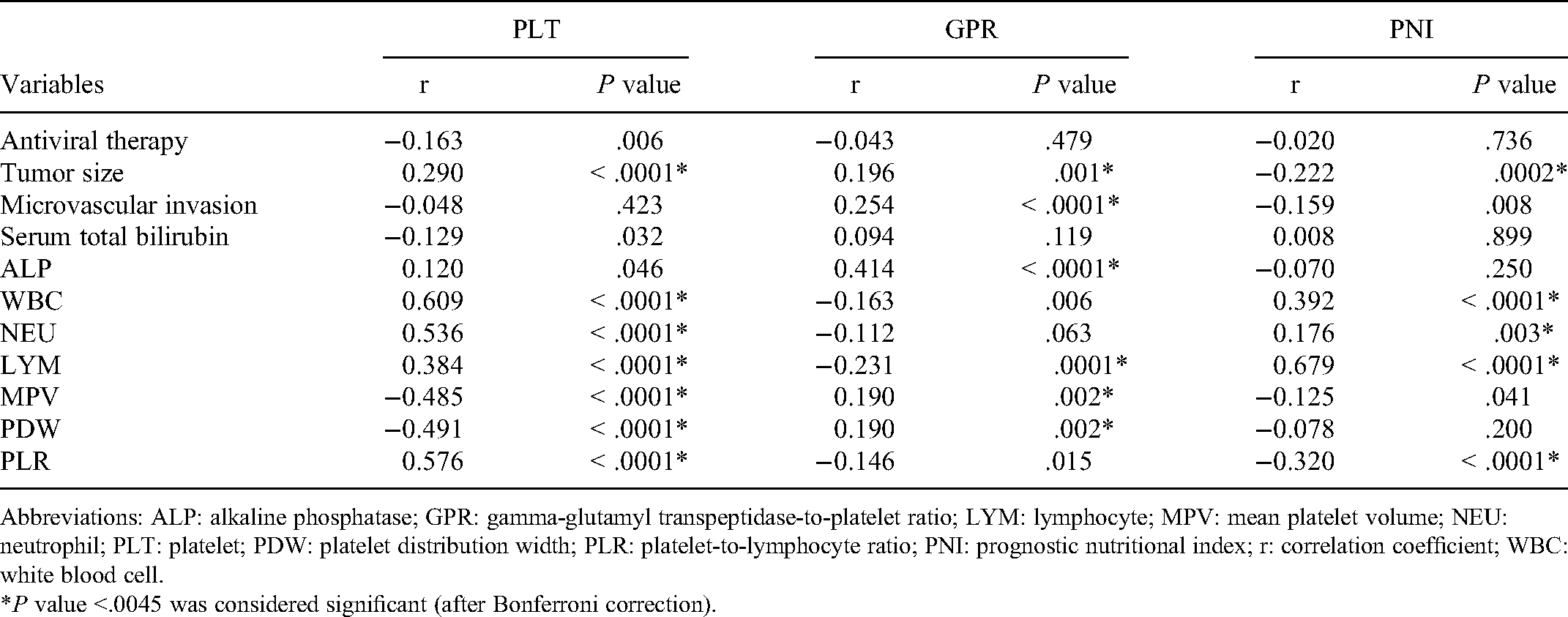
Abbreviations: ALP: alkaline phosphatase; GPR: gamma-glutamyl transpeptidase-to-platelet ratio; LYM: lymphocyte; MPV: mean platelet volume; NEU: neutrophil; PLT: platelet; PDW: platelet distribution width; PLR: platelet-to-lymphocyte ratio; PNI: prognostic nutritional index; r: correlation coefficient; WBC: white blood cell.
*P value <.0045 was considered significant (after Bonferroni correction).
Patients were also divided into two groups based on the GPR value (cut-off value is 0.2) by the ROC plot. The low-GPR (<0.2) group had a higher rate of hepatitis virus infection, higher PLT count, and higher PLR compared to those of the high-GPR (≥0.2) group. Also, GPR was significantly and positively correlated with ALP (r = 0.414, P < .0001).
Patients were further divided into two groups by PNI with a cut-off value of 51.9 through the ROC plot. A total of 187 patients were categorized as low-PNI (<51.9) and the remaining patients as high-PNI (≥51.9). The low-PNI patients showed larger tumor size, higher ALP, and higher PLR, but lower serum albumin, WBC count, and PLT count. In addition, PNI was significantly correlated with WBC count (r = 0.392, P < .0001), lymphocyte count (r = 0.679, P < .0001), and PLR (r = -0.320, P < .0001).
Identification of Preoperative Factors for Predicting the Survival of HCC Patients with Surgery
The median overall survival of all patients was 46.0 months, and 71.7% of patients remained alive during the follow-up period. The association between preoperative factors and overall survival was analyzed in Table 3. Univariable analysis showed that the following preoperative factors were significantly negatively correlated with OS: age≥58 years (P = .023), hepatitis (P = .039), PLT≥220 × 109/L (P = .001), PDW<12.8% (P = .049), PLR≥116 (P = 0.016), PNI<51.9 (P = .026), GPR<0.2 (P = .014), and APPR<0.55 (P = .042). Multivariable analysis by adjusting for all the confounding factors indicated that these factors significantly impacted OS during the follow-up period, they are: age≥58 years (HR, 2.227, 95% CI, 1.347-3.850, P = .002), PLT≥220 × 109/L (HR, 2.274; 95% CI, 1.061-4.876; P = .035), PNI≥51.9 (HR, 0.503; 95% CI, 0.265-0.954; P = .035), and GPR≥0.2 (HR, 0.432; 95% CI, 0.204-0.912; P = .028). Other platelet-related indices, such as PDW, PLR, and APPR, were not associated with OS (Table 3).
Univariable and Multivariable Analyses of Prognostic Factors Influencing Overall Survival of Patients after Hepatectomy.

Abbreviations: AFP:, α-fetoprotein; APPR: alkaline phosphatase-to-platelet ratio; APTT: activated partial thromboplastin time; CI: confidence interval; CEA: carcinoembryonic antigen; FIB: fibrinogen; GPR: gamma-glutamyl transpeptidase-to-platelet ratio; HR: hazard ratio; LYM: lymphocyte; MPV: mean platelet volume; PLT: platelet; PDW: platelet distribution width; PT: prothrombin time; PLR: platelet-to-lymphocyte ratio; PNI: prognostic nutritional index; TT: thrombin time ; WBC: white blood cell.
*P value <.05 was considered significant.
With the Kaplan–Meier analysis, we further evaluated the role of preoperative platelet-related indices in the OS prediction in the cohort. As shown in Figure 1, the patients with high-PLT, low-GPR, or low-PNI had an unfavorable OS after surgery. Statistical analysis showed a significant difference between the patients stratified by platelet counts (log-rank P = .0004), GPR (log-rank P = .0120), and PNI (log-rank P = .0231), respectively.

Comparison of overall survival (OS) by Kaplan–Meier curve analysis in the cohort. Patients after surgery were stratified based on (A) platelet count (PLT), (B) gamma-glutamyl transpeptidase-to-platelet ratio (GPR), and (C) prognostic nutritional index (PNI).
High-PLT and low-GPR are Critical Survival Factors with Propensity Score Matching Analysis
We analyzed the association of the factors with survival with propensity score matching analysis. The main demographic and clinical features were not significantly associated with OS based on propensity score matching (Tables 4 and 5). However, the high-PLT (log-rank P = .0248) and low-GPR group (log-rank P = .0220) were consistently associated with a more inferior OS (Figure 2).

Comparison of overall survival (OS) by Kaplan–Meier curve analysis in the cohort with propensity score matching analysis. Patients after surgery were stratified based on (A) platelet count (PLT) and (B) gamma-glutamyl transpeptidase-to-platelet ratio (GPR).
Comparison of the Main Clinical Characteristics of Patients Classified by PLT Sfter Propensity Score Matching.

Abbreviations: AFP: α-fetoprotein; ALP: alkaline phosphatase; CEA: carcinoembryonic antigen; GPR: gamma-glutamyl transpeptidase-to-platelet ratio; PNI: prognostic nutritional index.
Comparison of the Main Clinical Characteristics of Patients Classified by GPR After Propensity Score Matching

Abbreviations: AFP: α-fetoprotein; CEA: carcinoembryonic antigen; LYM: lymphocyte; MPV: mean platelet volume; PLT: platelet; PLR: platelet-to-lymphocyte ratio; PNI: prognostic nutritional index; WBC: white blood cell.
Discussion
In this study, we evaluated the predictive value of platelet-related measures for HCC patients’ survival after surgical resection. The preoperative high-PLT, low-GPR, and low-PNI that were significantly associated with more inferior OS might be independent prognostic factors for predicting survival outcomes of HCC patients.
Platelets are primarily regarded as the essential player in hemostasis and thrombosis. As a versatile factor, platelets also play crucial roles in the inflammatory response and contribute to cancer progression. 15 Platelets could promote tumor cells proliferation and invasion by releasing various soluble factors and allow tumor cells to evade immune surveillance by direct interaction with tumor cells. 16 Furthermore, platelets were also related to the increased risk of cancer metastasis. 17 Based on this, we presumed that platelets could be a potential marker for the progression of HCC. Consistent with most clinical research, 9 our study demonstrated that preoperative high-PLT count (PLT≥ 200 × 109/L) was an independent risk factor for poor prognosis in HCC patients. Propensity score matching analysis, which could avoid potential confounding bias, also indicated that high-PLT counts were associated with adverse survival. Our data further showed PLT count is positively associated with tumor size, which is also in line with previous reports. 18
We found that platelets were significantly and positively correlated with leucocytes. In tumor sites, platelets could recruit macrophages and neutrophils through multiple mechanisms, such as secretion of chemokine signals (SDF-1, serotonin, PF-4, and β-TG) and the formation of platelet-leukocyte complexes (interaction between platelet P-selectin and leukocyte PSGL-1). The close correlation between platelets and leucocytes showed that platelets were essential for the generation of tumor-associated leucocytes, stimulating platelet–tumor cell aggregation and tumor metastasis. 19 Therefore, these data suggested the potential role of PLT in the tumor microenvironment of HCC. Together, our data not only indicate the clinical significance of PLT in prognosis but also shed light on antiplatelet therapy as a new therapeutic strategy against HCC. Indeed, recent studies have verified the potential role of antiplatelet therapy with aspirin in reducing risks of carcinogenic disease outcomes. 20
It is not well studied concerning predictive roles of some indices incorporating both blood count and liver function in the survival of HCC patients after hepatic surgery. Our study demonstrated that low-GPR (GPR<0.2) and low-PNI (PNI<51.9) were independent risk factors for predicting poor prognosis of HCC patients. In contrast, the multivariable analysis did not show the significant association of APPR with survival and further study with a bigger cohort needed to clarify its predicatory roles.
Low-GPR was confirmed to be associated with the more inferior OS of patients in our cohort, which is inconsistent with the previous studies. 21 These contradictory data may be explained by the following reasons. First, although the expression of GGT was higher with larger tumors and could promote the development of tumors, 22 patients expressed GGT without a substantial rise, most of whom had liver cirrhosis in the study. It was probably because extensive hepatocyte necrosis, impaired bile, and early-stage of cancer could affect the formation of GGT. Second, high platelet count may play a more important role in our study. Finally, the small sample size, different inclusion criteria, and baseline characteristics of patients, and selection bias may also make a difference.
PNI, as a nutritional and immunological marker, is calculated from two available laboratory parameters (serum albumin level and peripheral lymphocyte count) in routine clinical practice. Our results well supported the prognostic value of PNI in HCC patients. Preoperative low-PNI was associated with poor survival, indicating large tumor size, poor histologic differentiation, and damaged liver function, which is consistent with several previous studies. 23 The predictive role of preoperative low-PNI could be explained by the hypoalbuminemia and lymphocytopenia. Low albumin levels caused by impaired liver function not only significantly correlate with more aggressive tumor parameters, 24 but contribute to the systemic inflammatory response as a harmful acute-phase protein. 25 Lymphocytopenia results in the loss of lymphocytes, which lead to the impairment of host antitumor immunity and further induce cancer relapse and worse prognosis. 26
Besides, old age was not only risk factors of developing HCC but also the predictors significantly associated with decreased survival in our cohort. Elderly patients could have more comorbidities and lower repair capability of the liver to influence postoperative complications that increased risks of the mortality. 27 The study has several limitations. First, the current study was a single-center preliminary study, and multiple centers are required for further validating our conclusions. Second, the study was a retrospective analysis with a limited number of patients, and larger-sample data from prospective studies would be better to explain the value of these platelet-related measures in predicting the survival of HCC patients.
Conclusion
In summary, our study demonstrates that high-PLT, low-GPR, and low-PNI are significantly associated with increased risk of death and more inferior OS in HCC patients after hepatectomy. These parameters, simple and easily obtained in routine blood tests, might be effective predictors for evaluating a favorable prognosis in patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China under Grant (number 81673080); the Shanghai Pujiang Program under Grant (number 2019PJD004); the Jiangsu Commission of Health under Grant (number H2018073); Shanghai Municipal Key Clinical Specialty (Laboratory Medicine, No.shslczdzk03303).
Ethical Approval Statement
The study protocol was approved by the Medical Ethics Committee of Huashan Hospital, Fudan University (approval 2013-098).