
Abstract
Introduction
Among women, breast cancer is the most commonly diagnosed cancer worldwide: the last edition of the Chinese cancers statistic released in 2019 by the Chinese National Cancer Center, 1 reported breast cancer as the first for incidence with 304,000 new cases diagnosed in 2015 representing 17.05% of the female incidence; the ranking in the United States, based on modelled projections, estimated 276,480 breast cancers for the female population by 2020, representing 30% of the total number of female cancers occurred this year. 2 The standard of care includes conservative surgery or mastectomy as appropriate, followed by adjuvant radiotherapy. Adjuvant radiotherapy for breast cancer improves locoregional control and overall survival rates, however, it is unavoidable to irradiate the surrounding healthy tissues mainly, the heart, lungs, and contralateral breast with a significant number of non-cancer-related deaths. 3 Increased risk of fatal cardiac events, pneumonitis, as well as of a second primary cancer of the breast has been largely reported.4,5 Given the occurrence of this disease even at a young age and the increased life expectancy, it is essential to limit long-term complications as much as possible. Currently, for women who must undergo radiotherapy to the left breast, all the various techniques available are examined to limit the dose to the heart. Efforts are being made to move the heart away from the radiation field through prone positioning of the patient, coordination of the respiratory cycle, using advanced technologies such as intensity-modulated radiotherapy, the use of proton beams, accelerated partial irradiation on smaller volumes, and intraoperative radiotherapy. Shah et al 6 provided an updated review of these contemporary techniques for avoiding cardiac protection showing that, although promising from a dosimetric perspective, there are limited data on late cardiac events due to the difficulties of long-term follow-up. Several studies pointed on the fact that the motion of the thorax can have a crucial impact on heart dose in left-sided breast cancer patients; 7 Quirk et al 8 analyzed chest wall respiratory motion using an external surrogate that could potentially be considered closer to reality for the early breast cancer patient population because the trajectory of the tumor will be more faithful to the trajectory of the external surrogate; they recorded a significantly lower maximum chest amplitude during normal breathing than during deep breathing.
Breath hold (BH) in left breast treatment increases the distance between the target and the heart allowing to minimize irradiation of nearby organs at risk while maintaining an adequate target dose coverage9–11 and has become the gold standard in clinical practice in many institutions.12–14 Patients who can tolerate deep inspiration BH (DIBH) may yield a benefit from it as reported by Conroy et al 15 who focused their investigation on cardiac positioning instead of cardiac dose evaluation while irradiating left-sided breast tumor in voluntary DIBH.
Breast cancer treatment has historically been performed with 2 opposing non-divergent isocentric tangent fields, using 6 MV photon energies, with the addition of beam modifiers to homogenize the dose within the target;16,17 recently tangential field-in-field (TFiF) technique, also referred to as forward intensity-modulated radiation therapy is used as an alternative. Several groups have compared the dosimetry in free breathing (FB) versus BH for the left breast treatment; many studies performed the comparison using a single cohort of patients scanned twice, once in FB and again in BH;18–20 while other studies12,21 considered different clinical datasets for both FB and BH, focusing on specific dosimetric parameters of the heart and lung, mainly the mean dose to the heart and lung and 1 or 2 significant points of the dose-volume histogram as also reported by the meta-analysis published in 2020. 22
This study compares the dosimetry of the planning target volume (PTV), the heart, the left and right lung, and the right breast for a large clinical series of left-sided breast cancer patients treated with forward intensity modulated radiation therapy with different delivery modalities (FB or BH). In addition to the mean and maximum dose, different dosimetric cut-off points along the dose volume histogram (DVH) of the heart and ipsilateral lung were analyzed, as well as the mean and maximum dose to the right breast and contralateral lung, enriching with valuable data to the existing FB and BH statistics; moreover, the possible correlation between physical parameters such as target size, left lung volume with heart and left lung dosimetric parameters, were investigated for both delivery techniques.
Materials and Methods
BH for post-operative left-sided breast cancer patients became part of the standard radiotherapy treatment offered by our department from April 2019, nevertheless, its use remains at the discretion of the physician treating the patient. At the beginning of the year 2020, a 3-dimensional (3D) surface tracking system has been introduced in the daily clinical routine of breast treatment, and this has renewed the interest in the use of the BH technique due to the simplicity and rapidity of monitoring the correct setup of the patient during the positioning and delivery phase.
This retrospective study included 155 early-stage left breast carcinoma patients consecutively admitted to our hospital in 2020 and referred by physicians for whole breast radiation therapy in FB (73 patients), and BH (82 patients). The inclusion in the study was interrupted once reached about half of the cases treated annually in our department.
The research was approved by the Institutional Ethics Committee of Sichuan Cancer Hospital and Research Institute (Approval Number No. SCCHEC-02-2021-026). The patients gave oral consent to the use of data regarding their radiation treatment for research purposes; data were anonymized before use and patient details de-identified. The reporting of this study conforms to STROBE guidelines. 23
Treatment Preparation: Simulation, Contouring, Treatment Planning
The patients were immobilized with a WingStep (IT-V, Innsbruck, Austria) breast board in the supine position. CT scans were acquired with 3 mm slice thickness with a 16-slice Brilliance Big Bore CT scanner (Philips Medical Systems, Cleveland, OH). The CT scans were performed in FB or BH for their use in FB or BH treatment, respectively, following the indication of the referring physician. Patients to be treated in BH were previously instructed by the doctor on how to hold their breath and were invited to practice at home. On the day of the CT scan, the procedure was repeated to them, and after a few attempts, the technician assessed whether the patient could hold her breath for more than 25 s and whether she could reproduce a stable BH position, according to an internal protocol of our department, described in detail in a previous publication. 24
Imaging datasets were imported to MIM Version 7.0.5 (MIM Software Inc.) for contouring. Target volume and organs at risk were outlined by experienced radiation oncologists of the breast department. Clinical target volume (CTV) of the residual breast included all mammary tissues as visualized on the CT scans; the contouring was aided by a copper wire placed along the palpated breast tissue during simulation. The PTV was generated as an isotropic expansion of the CTV with a 3 mm margin in all directions; the first 5 mm inside the body external contour were excluded both from the CTV and from the PTV; the organs at risk (OARs) delineations were performed according to the breast cancer atlas for the radiation therapy planning consensus definitions. 25
CT images and radiotherapy structures were imported to Pinnacle 3TM Version 9.10 (Philips Medical Systems) treatment planning system. All plans were based on TFiF technique with a 6 MV photon beam energy of an Elekta Infinity (Elekta) LINAC. TFiF consisted of 2 opposing tangential fields with gantry angle between 300° and 315° for the medial beam and 120° and 135° for the lateral beam, each including 3 to 5 subsegments. Patients were treated with a prescribed dose (Dp) of 50 Gy in 25 fractions, 1 fraction per day. The plan was optimized to achieve a minimum of 95% of the PTV covered by 95% isodose line and a mean dose (
Surface Guided Treatment
At the LINAC, the patient's surface (limited to the chest area) was acquired by a 3D real-time surface tracking system, AlignRT (Vision RT, Ltd). The real-time surface position was compared with the surface acquired at the planning CT (reference surface) for the patient positioning and during the beam delivery. AlignRT reports the real-time deltas for 3 translational and 3 rotational directions, and through the automatic gating function, the accelerator stops irradiating if the 2 surfaces deviate beyond the defined tolerance thresholds. The thresholds set up in our department for breast treatments are ±3 mm in the translational directions and ±3° in the rotational directions. This procedure is used for both FB and BH treatments. During BH treatments, patients have a visual tool helping them to maintain the breath within the tolerance level guiding them through inspiratory inconsistency. 27
Data Analysis
DVH endpoints were used to compare the dosimetry of the FB and BH left-sided breast radiotherapy treatments; for the PTV, the volume,
Results
Patient and tumors characteristics of the FB and BH groups are shown in Table 1. The 2 groups present no significant differences in age and body mass index (BMI) (P = .654, P = .703, respectively), neither in the tumor grading and pathological tumor node metastasis stage (P = .452, P = .543, respectively). Furthermore, from the frequency analysis, 153 out of 155 of the patients included in this study had a BMI in a standard range (18.5-24.9) kg/m2 as defined by WHO (World Health Organization), and 80% of the patients had a left breast volume of less than 837 and 778 cm3 for the BH and FB groups, respectively. The target and OARs DVH representative dosimetric parameters for FB and BH groups were reported in Tables 2 and 3, respectively. The BH percentage difference was calculated as (BH−FB)/FB in percentage.
Patient and Tumor Characteristics.

Planning Target Volume Dosimetric Parameters in FB and BH.

OARs Dosimetric Parameters Comparison for FB and BH Treatments.

Note: P-values < .05 are highlighted in bold.
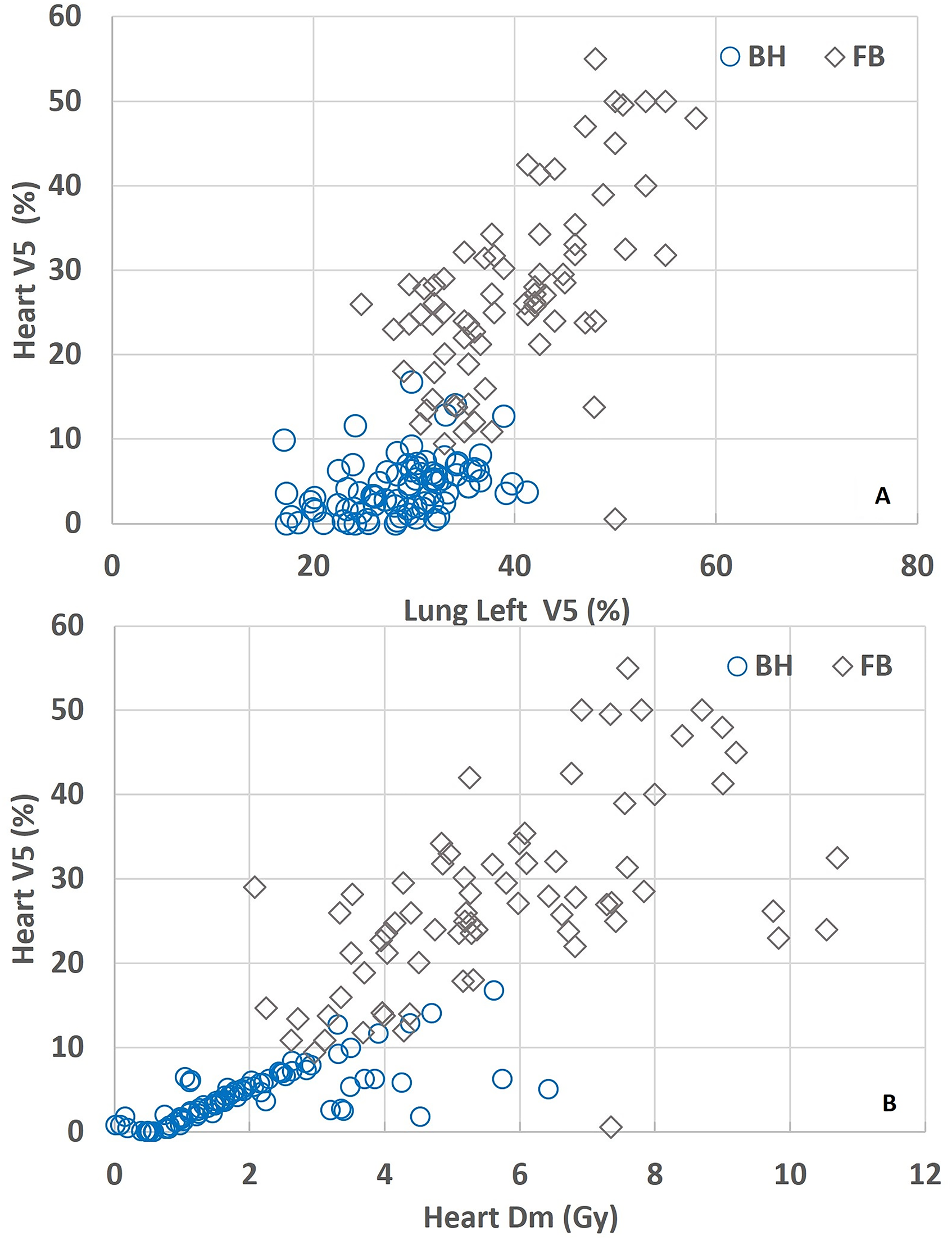
Comparing the dosimetry of the heart, significantly lower values for patients in the BH group were recorded; particularly heart median value
Heart and left lung representative dosimetric parameters for FB and BH treatments.
Pearson Correlation Coefficients and P value (in parenthesis) for FB and BH Treatment Parameters.
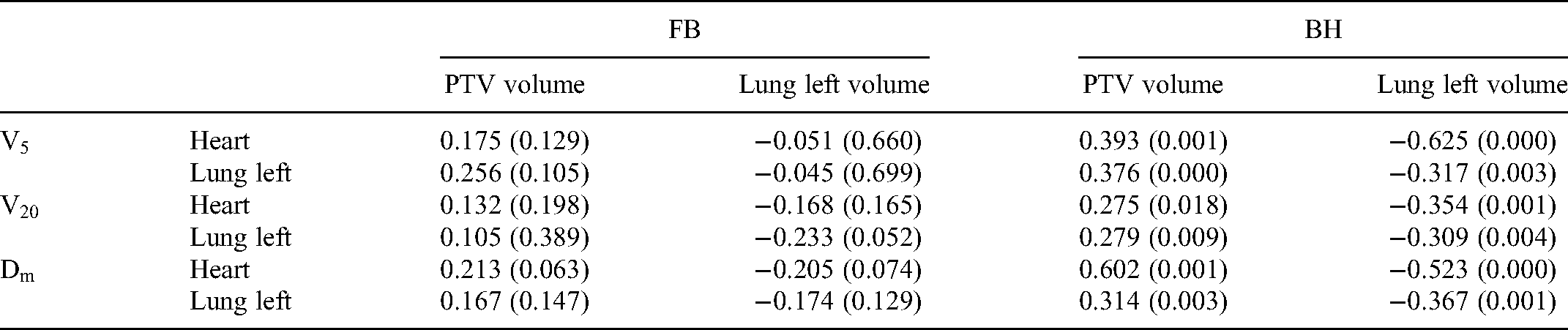
We found that an increase in the volume of the target gives rise to a positive Pearson coefficient indicating a corresponding increase in the value of the dosimetric parameters of both heart and lung in both groups; this increase is only significant for the BH group. Similarly, we can observe that an increase in the volume of the left lung tends to decrease (negative Pearson coefficient) the value of the dosimetric parameters in both groups, but this decrease is again only significant for the BH group; The dosimetry trends of the heart and lung, which are positively correlated in the case of an increased target volume, and negatively correlated in the case of increased left lung volume, are shown in Figures 2 and 3, respectively for the BH group as they are statistically significant.

Correlation between the target volume and the heart representative dosimetric parameters for breath hold treatments.

Correlation between the left lung volume and the heart representative dosimetric parameters for breath hold treatments.
Discussion
In recent years, radiotherapy techniques such as volumetric modulated arc radiation therapy, and TFiF forward intensity-modulated radiation therapy, have been introduced as an alternative to classic opposing tangential fields as a treatment strategy to improve the homogeneity of the target coverage while reducing the doses to OARs; moreover, several studies showed a significant reduction in cardiac exposure in case of left-sided breast treatments by implementing respiratory management methods in radiation delivery, such as voluntary, DIBH, active breath control.9,10,13 In this study, we included radiotherapy treatments of the left side of the breast after conservative surgery, performed with the TFiF technique in a BH or FB setup and using a real-time guided 3D surface monitoring system. The groups of patients treated in BH or FB, were found to be homogeneous in terms of age, body conformation and size of the target to be treated. The radiation doses to cardiac and left lung parameters were significantly reduced with the BH technique; a positive moderate correlation in FB and BH between the target volume and heart
Regarding the mean dose to the heart, its median value in BH is 1.7 Gy and is 3.6 Gy (67.9%, P = .003) lower than its value in FB. A systematic review by Smyth et al 28 in the benefit of cardiac dose sparing including 10 studies showed a statistically significant reduction of the mean dose to the heart with the DIBH technique by up to 3.4 Gy when compared to a free-breathing approach; this decreased value is in line with our results. Quirk et al 29 conducted a retrospective study of a large cohort of left-sided breast cancer patients treated in DIBH and found a median dose to the heart of 1.0 Gy; similarly, Yeung et al 30 analyzed twenty patients undergoing CT simulation in both FB and BH and found a dosimetric benefit from DIBH treatments registering a median dose of 1.1 Gy in BH, values in line with the median dose value we assessed, underlining the importance and effectiveness of using breath control methods. The results of the meta-analysis by Lai et al 22 including 12 observational studies each with total number of cases greater than or equal to 40, reported, as for our research, statistically significant lower heart and left lung doses in BH when compared to FB.
Most of the published studies show a reduction in the mean dose to the heart and left lung. Our work evaluates in addition to these values, several significant points of the DVH (V5, V10, V20, V30), and Dmax highlighting a significant percentage decrease of these parameters in BH compared to FB, ranging for the heart from a maximum of 100% (V30, P = .003) to a minimum of 27.1% (Dmax, P = .001); similarly, for the ipsilateral lung, from a maximum of 22.4% (V5, P = .003) to a minimum of 1.6% (Dmax, P = .006); in addition, the mean and maximum doses for the breast and contralateral lung are also assessed but show no significant differences between FB and BH.
Considering that Darby calculated a linear increase in excess relative cardiovascular risk of 7.4% per Gy of mean cardiac dose (95% confidence interval, 2.9% to 14.5%; P < .001), these differences in doses can be considered clinically significant. The decrease in the heart dose in BH compared with the FB is maintained at all points of the dose-volume histogram, from high to low doses, particularly the heart volume receiving doses between 5 and 30 Gy is reduced between 80% and 100% in BH. The increase in cardiovascular deaths appears to be mainly due to high-volume irradiation to the heart. 31
In the left-sided breast treatments, frequently, the apex of the heart is close, or even within the radiation field, resulting in a maximum dose exposure of the heart of up to >20 Gy; this is the case of our study for the FB group with a heart
The volume of the left lung registered for patients in the BH group is as expected significantly increased (+79.2%, P = .008) compared with the volume obtained for patients in the FB treatment group. It is well known that the lung is sensitive to ionization radiation and side effect may arise, as acute or subacute pneumonitis and late lung fibrosis; the risk for acute and chronic RT-induced lung morbidity is also influenced by irradiated lung volume.
34
The filling of air in the lung allows the heart to be moved away from the target in favor of lung volume occupying the space left free. This mechanism may reduce the percentage of lung volume receiving given doses. In our research we highlighted that comparing BH and FB groups DVH endpoints, the reduction in the volume of the left lung receiving given doses in BH compared to FB, decreases as the dose increases: Δ
Following this study, patients with small breast volume treated in BH seems to more benefit from the heart and left lung dose reductions. Focusing on heart
Our study had some limitations. A power analysis of the sample size was not performed, and the number of patients used in the 2 cohorts is too small to have any claim to strong statistical significance. Moreover, the results were obtained using the patient data derived from the clinical practice of our department using a defined treatment technique; the research does not have the value of a multi-institutional quality-assurance program, therefore the results cannot be generalized. Moreover, patients included in this study had a BMI in a standard range and left breast small sized. Further investigations with a cohort of patients with a wider range of physical characteristics and using different radiation techniques are desirable. Long term follow-up is needed to establish the clinical differences between FB and BH delivery techniques.
Conclusion
Findings from this observational study suggest that BH technique for left-sided breast treatments may reduce the dose to the heart and left lung compared to FB; increased dosimetric advantages for small-sized breasts, and large left lung volumes may be considered in choosing treatment strategies.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest concerning the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Prof. Li Jie received a grant (N.2021YFG0320) by Sichuan Province Science and Technology Support Program (CN); (![]() ). The funders had no role in study design, data collection and analysis, decision to publish or preparation of the manuscript.
). The funders had no role in study design, data collection and analysis, decision to publish or preparation of the manuscript.
Ethical Approval
The study received the approval of the Sichuan Cancer Hospital Ethics Committee, in accordance with the ICH-GCP principle and related regulation/guidelines (Approval Number No. SCCHEC-02-2021-026, Approval date 28 April 2021). Patients gave verbal consent to the research.