
Abstract
Introduction
Breast cancer is one of the most prevalent malignant carcinomas among women, and the incidence and mortality rates have been increasing.1,2 Additionally, approximately 50% of all women diagnosed with breast cancer experience metastatic disease, and the most common metastatic sites are the liver, lung, bone, and brain.3,4 Liver metastases occur in approximately 50% of all metastatic breast cancer patients, and 5 to 12% of patients develop liver metastases as the primary site of breast cancer recurrence. 5 Systemic treatment including the chemotherapeutic agents or endocrine therapy is still the standard treatment in patients with breast cancer liver metastasis (BCLM). 6 Capecitabine also improved 5-year disease-free survival as maintenance therapy in breast cancer who received standard adjuvant treatment. 7 Although some progress has been made in systemic therapies, the clinical outcomes for patients with BCLM are still poor and affect patients’ long-term survival.8-10 Therefore, improving the prognosis of BCLM patients remains a major challenge.
Previous studies have suggested that the combination of a hepatic arterial infusion pump and systematic chemotherapy was helpful for patients with colorectal liver metastases (CRLM) to achieve a high local response and prolong survival.11-14 Moreover, it was reported that HAI gemcitabine and FUDR were effective in prolonging survival time and improving the DCR of intrahepatic lesions for NPC patients with liver metastasis and were connected with a relatively low rate of toxicity. 15 The purpose of this study was to explore the benefits and risks of HAI chemotherapy in patients with breast cancer liver metastasis.
Materials and Methods
Patient Selection
In this retrospective study, the diagnoses of all patients with BCLM were based on conventional clinical, radiographic and histopathology or cytological criteria. Between Jan 2012 and Dec 2019, we treated 19 consecutively eligible patients with breast carcinoma liver-predominant metastases. Before the initial treatment, all patients aged over 18 years had an Eastern Cooperative Oncology Group (ECOG) performance status (PS) of 0 to 2, adequate bone marrow reserve and organ function, and normal electrocardiogram. Furthermore, none of the subjects enrolled in this study suffered from other cancers. The treatment protocol was discussed and determined by a multidisciplinary treatment (MDT) team in our hospital and was approved by the ethics committee of our hospital. Written informed consent was obtained in accordance with the principles of the Declaration of Helsinki and Good Clinical Practice Guidelines.
Implantation of the HAI Catheter System
The infusion catheter and injection port (Celsite, B. Braun, Chasseneuil, France) were implanted as previously described.12,15,16 The main steps of this procedure include the following: (a) The anatomy of the hepatic artery and indication for HAI therapy were evaluated by computed tomography angiography before the operation; (b) the Seldinger technique was used to obtain access to the right femoral artery under the guide of digital subtract angiography (DSA); (c) angiography of the celiac trunk and superior mesenteric artery was performed to reveal the anatomy of the hepatic artery; (d) the gastro-duodenal artery (GDA), right gastric artery, and, if necessary, left gastric artery or dorsal pancreatic artery were embolized using metallic coils (Tornade, Cook, Bloomington, IL, USA) to prevent gastrointestinal mucosa injury caused by chemotherapy drugs; (e) the infusion catheter with side holes was placed into the GDA using the same coils as mentioned above or was inserted into the peripheral branch of the hepatic artery, and the position of the side hole was sited at the common hepatic artery. Therefore, the chemotherapeutic agents infused the entire liver from the side hole; (f) the proximal end of the infusion catheter was connected to an injection port, and the device was implanted into a subcutaneous pocket in the right inner thigh. After the administration of chemotherapeutic agents, the implanted port and indwelling catheter system were flushed and filled with 2 mL of heparin solution (1000 IU/mL).
Treatments
All patients received a 3-week cycle of oral capecitabin (1000 mg/m2/day, twice daily for 14 days) and HAI therapy, which was performed on days 1 and 8: gemcitabine 1 g/m2 for 30 min. At the same time, a blended solution including FUDR (0.15 mg/kg/day), dexamethasone (DXM) (1 mg/m2/day), low molecular heparin (3200 U) and 250 mL of saline was started using the infusion pump (Accufuser, Woo Young Medical Co., Ltd, Korea), which connected to the port-catheter system on day 1 and was continuous for 14 days. Drug toxicity was assessed, and dose adjustment was made according to the National Cancer Institute-Common Terminology Criteria for Adverse Events (NCI-CTCAE) version 3.0. If there were serious technical catheter-related problems, intrahepatic disease progression, severe toxicity occurred or patient refusal, HAI therapy was stopped. Patients with epigastric pain prompted workup using upper gastrointestinal endoscopy. If an ulcer or gastroduodenitis was observed, HAI therapy was stopped for 1 month to allow for recovery, and the dose of FUDR and DXM was reduced in subsequent therapies.
Disease Assessment
The therapeutic efficacy was assessed every two HAI cycles or when necessary by computed tomography scan. The response to treatment was evaluated in accordance with response evaluation criteria in the solid tumors committee: complete remission (CR), partial remission (PR), stable disease (SD), and progressive disease (PD). The primary endpoint of the study was the overall response rate (ORR), which was defined as the sum of CR and PR rates. Overall survival (OS) was defined as the time from the date of catheter implantation to the date of death or the date of the last follow-up. Median survival time (mOS) was defined as the time from the date of catheter implantation to the date when 50% of individuals were alive.
Statistical Analysis
All statistical analyses were performed using SPSS 13.0 software (SPSS Inc., USA). Fisher's exact test was used for rate comparison between two groups. The survival curve was estimated using the Kaplan-Meier method. Survival curves were compared using the log-rank test. A P value less than .05 was considered statistically significant.
Results
Patient Characteristics
Nineteen patients (all females) with unresectable BCLM were enrolled in this study. The characteristics of the patients are listed in Table 1. The average age was 55.58 years old (range 33 to 76). All of them scored 0 to 2 on the ECOG score standard. The pathological types of all 19 patients were recorded, including 17 (89.5%) invasive ductal carcinomas and 2 (10.5%) invasive lobular carcinomas. Of the 19 patients, 13 (68.4%) were estrogen receptor positive (ER+), 10 (52.6%) were progesterone receptor positive (PR+), and only 4 (21.1%) were human epidermal growth factor receptor 2 positive (HER-2+). The status of hepatic metastases, including synchronous hepatic metastases at the initial diagnosis of breast carcinoma and disease progression to hepatic metastases, was evaluated by the proportion of hepatic involvement, lobular involvement, number of hepatic lesions, existence of extrahepatic metastases, and baseline level of albumin.
Characteristics of patients.

Tumor Response and Survival
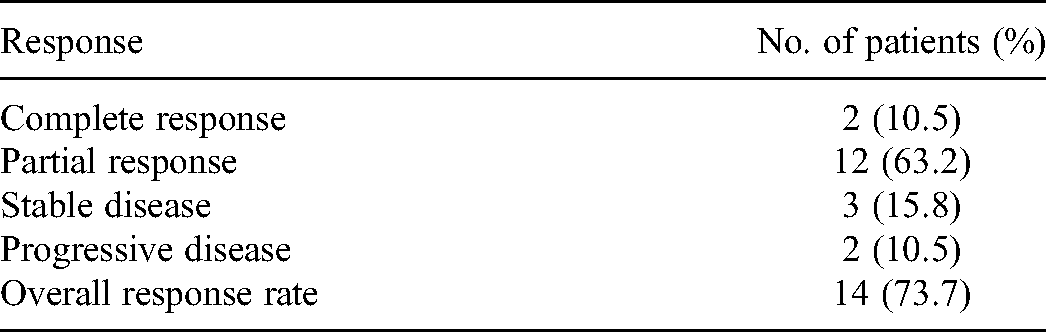
As shown in Table 2, 2 patients (10.5%) had CR, 12 patients (63.2%) achieved PR, and 3 patients (15.8%) achieved SD. The overall response rate (ORR) of intrahepatic lesions was 73.3%. Additionally, we found that young patients (age < 55 years) had a higher ORR than the older (100% vs 44.4%, P = .011, Table 3). The median follow-up was 28 months (range 2 to 40 months). At the last follow-up, 3 patients were alive. The median overall survival (mOS) was 13.1 months (Figure 1). Kaplan–Meier survival curves demonstrated that the mOS was not significantly different between patients with < 9 intrahepatic lesions and those with ≥ 9 lesions (Figure 2) (13.7 months vs 10.9 months, P = .225). The mOS was 14.3 and 10.6 months for patients without extrahepatic metastases and with extrahepatic metastases, respectively (P = .016), which is statistically significant (Figure 3). Encouragingly, 2 patients received the opportunity for percutaneous radiofrequency ablation for liver metastasis after treatment.

Kaplan-Meier analysis of overall survival (the mOS was 13.1 months).

Survival curves were analyzed by the Kaplan–Meier method and log-rank test. The median overall survival was 13.7 months in the patients with < 9 intrahepatic lesions and 10.9 months in those with ≥ 9 lesions (P = .225).

Survival curves were analyzed by the Kaplan–Meier method and log-rank test. Patients with extrahepatic metastases had a significantly poorer median survival time than those without extrahepatic metastases (10.6 months vs 14.3 months, respectively). P = .016).
Tumor response.
Associations between overall response rate (ORR) and clinical variables.

*Fisher's exact test was used
n.d, Not done
Side Effects and Adverse Events
The major adverse events include hematological and hepatic dysfunction, gastrointestinal reactions, fatigue, allergy and fever. See Table 4. None of the patients had grade 4 toxicity. The most common grade 3 toxicities included leucopenia in 2 of 19 patients (10.6%), neutropenia in 1 of 19 patients (5.3%) and diarrhea in 1 of 19 patients (5.3%). The other treatment-related toxicities were mild and reversible.
Adverse effects.

Discussion
The liver in patients with breast cancer is the third most frequent site of such metastases after the lungs and bones. 17 When liver metastatic disease is diagnosed, treatment is generally palliative and usually consists of systemic therapies only. Systemic treatment such as chemotherapy, endocrine therapy-based on hormone status, and biological therapy is complex. The chemotherapeutic agents including the 5-fluoroouracil-based or anthracycline-based regimens, such as cyclophosphamide, doxorubicin, and capecitabin are widespread. Other drugs such as docetaxel and gemcitabine are also actively considered. 18 Currently, systemic therapies have improved, but the median survival rates range between 3 and 16 months,19,20 which provides the impetus for us to explore new therapeutic strategies. The occurrence of liver metastases is expected to determine the survival time of patients with metastatic breast cancer. Thus, preventing the progression of liver metastases often determines the success or failure of treatment. HAI chemotherapy has been widely accepted in the treatment of colorectal cancer liver metastasis patients.11-13 In addition, HAI chemotherapy has also been suggested to be helpful for patients with NPC liver metastasis, but a few patients had extrahepatic progression during the trial treatment. 15 In this study, we administered HAI gemcitabine plus FUDR combined with systemic chemotherapy for 19 patients with BCLM. The overall response rate (ORR) of intrahepatic lesions was 73.7%. The median overall survival (mOS) was 13.1 months. Additionally, Kaplan–Meier survival curves showed that patients without extrahepatic metastases had a longer survival time than patients with extrahepatic metastases. These findings indicate that HAI chemotherapy seems to be an effective treatment for liver metastases for certain different tumors in a palliative situation. However, HAI therapy alone cannot suppress extrahepatic progression of tumors due to the concentration of chemotherapy drugs in liver lesions. Therefore, we treated patients with HAI combined with systemic chemotherapy.
HJ Stemmler et al confirmed that the regimen of gemcitabine plus capecitabine was more beneficial in effectiveness and safety for patients with metastatic breast cancer. 21 In addition, Katrin Eichler et al revealed that TACE with gemcitabine appears to be a safe and effective treatment for patients with liver metastases from breast cancer in a palliative situation and revealed that the progression-free survival was 3.3 months and the median survival time was 10.2 months. They observed a response rate of 7% (complete and partial remission) in 39% of patients with stable disease and in 54% of patients with a progressive disease. 22 In our study, HAI gemcitabine plus FUDR combined with capecitabine was chosen because the patient was in relatively poor physical condition due to extensive liver metastases. Our results indicated that the overall response rate (ORR) of intrahepatic lesions was 73.7%, and the median overall survival (mOS) was 13.1 months. Fortunately, 2 patients received the opportunity of percutaneous radiofrequency ablation for liver metastasis. It seems that patients in our study probably have more survival benefit. Moreover, we found that young patients (age < 55 years) had a higher ORR than the older, which could be attributed to the better physical status of young patients and good tolerance to chemotherapy.
Theoretically, liver tumors derive most of their blood supply from the hepatic artery as opposed to the portal vein of normal liver tissue. 23 Hepatic artery infusion (HAI) chemotherapy allows most of the chemotherapy drugs to be delivered to liver metastatic lesions and increases local concentrations of a chemotherapeutic agent, thus potentially increasing the cell-kill fraction and reducing systemic toxicity, decreasing the total tumor burden and yielding a survival benefit. FUDR is an antimetabolite derivative of 5-FU, which has been shown to have a short half-life and high liver extraction rate (> 90%).24-26 In the current study, especially for HAI FUDR, the low-dose and continuance infusion may provide a higher drug concentration in the liver and little systemic toxicity. Thus, FUDR is suggested as an ideal chemotherapy drug for HAI and was used in the study.
Some investigators have reported that the complications associated with implantation of catheter and port systems included infection, catheter displacement and thrombosis, and the specific toxicities of HAI FUDR consisted of reactive gastric or duodenal mucosal lesions, chemical hepatitis and biliary sclerosis.27-29 Fortunately, these adverse events did not occur in the current study, probably because of adding DXM into the FUDR solution and using the fixed catheter tip method, in which the main branch vessels from the associated arteries (eg, hepatic artery or GDA) were routinely embolized during the operation. Our patients also had high-quality professional postoperative nursing care. In our study, the major adverse events (hematological, hepatic dysfunction, gastrointestinal reactions, fatigue, allergy and fever) were low and tolerable. None of the patients had grade 4 toxicity. The most common grade 3 toxicities included leucopenia in 2 of 19 patients (10.6%), neutropenia in 1 of 19 patients (5.3%) and diarrhea in 1 of 19 patients (5.3%). This relatively low rate of toxicity improved the quality of life of BCLM patients. This result indicates that HAI gemcitabine plus FUDR for liver metastases in breast carcinoma patients is safe.
Conclusions
Our data show that HAI chemotherapy is useful in preventing the progression of liver metastases and achieving long-term survival of patients with BCLM. Extensive liver metastases can effectively decrease the number and size of tumors, thus allowing patients to undergo percutaneous radiofrequency ablation or surgery for liver metastasis. Encouragingly, 2 patients in this study obtained percutaneous radiofrequency ablation opportunities after treatment and had no intrahepatic recurrence for a long time. Here, we introduced an alternative treatment method for patients with BCLM, which may be considered an option for suitable patients. However, the limitations of this study were that it was a retrospective study with a small sample size and it lacked a control group with matched BCLM status. Additional progressive studies with larger samples and multicenter randomized studies to confirm the efficacy and safety of HAI therapy are necessary.
Supplemental Material
sj-docx-1-tct-10.1177_15330338211051552 - Supplemental material for Hepatic Artery Infusion Pump Combined With Systemic Chemotherapy for Patients With Liver Metastases From Breast Carcinoma
Supplemental material, sj-docx-1-tct-10.1177_15330338211051552 for Hepatic Artery Infusion Pump Combined With Systemic Chemotherapy for Patients With Liver Metastases From Breast Carcinoma by Hong-Bing Shi, Wei-Guang Qiang, Wei-Liang Zhu, Ye Yuan, Jun-Jun Wang, Jie-Min Zhao and Wen-Wei Hu in Technology in Cancer Research & Treatment
Footnotes
Authors’ Note
Wenwei Hu conceived and designed the experiments. Hongbing Shi and Weiliang Zhu performed the experiments. Jiemin Zhao and Ye Yuan analyzed the data. Hongbing Shi, Weiguang Qiang and Junjun Wang wrote the paper. Wenwei Hu edited the manuscript. All authors read and approved the final manuscript. This study was approved by the ethics committee of The Third Affiliated Hospital of Soochow University. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. Written informed consent was obtained from the patients.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the This research project was supported by the Science and Technology Project of Jiangsu Traditional Chinese Medicine (grant number YB2017059).
Supplemental Material
Supplemental material for this article is available online.
Abbreviations
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.