
Abstract
Introduction
With the rapid progress and wide application of endoscopic technology, the incidence of early stage esophageal carcinoma (EC) is increasing, and now accounts for up to 40% of esophageal squamous cell carcinoma. 1
As a crucial diagnostic and therapeutic method for early stage EC, endoscopic resection (ER) has the advantages of being able to evaluate pathological parameters, including tumor invasion depth, lymphovascular invasion (LVI) status, and tumor differentiation grade; as well as allows removal of local lesions while achieving organ preservation.
However, tumors with submucosal invasion (pT1b) have a relatively high rate of lymph node (LN) metastasis, ranging from 15% to 42%.2–6 Additionally, several studies have reported a comparatively high LN relapse rate of 25%-30% in patients with pT1b-SM2 (submucosal invasion depth ≥200 μm) disease treated with ER alone.7–9 Eguchi et al 2 reported that the LN metastasis rate of pT1a-M3 (muscularis mucosae invasion) disease with or without LVI was 42% and 10%, respectively. Furthermore, Yamashina et al 9 found that the 5-year cumulative recurrence rate of pT1a-M3 patients with or without LVI treated solely with ER was 47% and 1%, respectively. In addition, a scoring system based on NCDB that identifies patients with early stage EC at risk of LN metastasis also showed that pT1b and LVI were independent risk factors. 10 The aforementioned data indicate that for patients with pT1b or LVI, ER alone is noncurative, and additional treatment is needed.
However, the optimal mode of additional treatment after ER remains unclear. Considering the curative effect of radiotherapy (RT), it is reasonable to speculate that, based on radical local excision of the ER and effective regional treatment of RT, the combination of these two organ preservation treatment modes could hopefully improve survival and ensure quality of life. However, high-level evidence to prove the safety and efficacy of this multimodality therapy is relatively scarce. Herein, we retrospectively analyzed the clinical outcomes of stage I EC patients with high-risk factors who received RT at our institution after ER.
Materials and Methods
From January 2010 to August 2019, patients with EC who received RT or ER at our institution were retrospectively screened. The inclusion criteria were as follows: (1) pathologically proven EC, including squamous cell carcinoma, adenocarcinoma, or adenosquamous cell carcinoma; (2) cT1N0M0 disease based on computed tomography and/or ultrasound examinations before ER; (3) pT1 disease with high-risk factors (submucosal, lymphovascular, or venous invasion) based on endoscopically resected specimens; and (4) ER followed by additional RT. Exclusion criteria were as follows: (1) other pathological types other than those mentioned above, (2) inadequate examinations to confirm clinical stage, (3) positive resection margins after ER, and (4) local-regional or distant metastasis (DM) before RT.
Chest computed tomography (CT) with or without contrast was mandatory to identify mediastinal LN status. Cervical and abdominal CT or ultrasound were needed to exclude positive LNs and DM. Emission computed tomograph (ECT) and brain magnetic resonance imaging were not performed.
Endoscopic mucosal resection and endoscopic submucosal dissection (ESD) were performed at our institution and were permitted in the present study. Additional RT should be administered within 6 months of ER. GTVtb was defined as the esophagus between the upper and lower borders of the ER, and was marked endoscopically with a surrogate. Clinical target volume (CTV) was defined as the LN drainage area of GTVtb plus a 2-5 cm craniocaudal margin with or without elective lymph node irradiation (ENI). Planning target volume (PTV) was defined as CTV plus a 3-dimensional, 5 mm margin. A total dose of 44.0-60.0 Gy in common fractionation based on intensity modulated radiotherapy (IMRT) technology was conducted. Adjuvant chemotherapy can be administered. Platinum and paclitaxel liposome-based chemotherapy regimens can be administered weekly or every three weeks either concurrently or sequentially with RT.
Patient characteristics, treatment details, overall survival (OS), disease-free survival (DFS), cancer-specific survival (CSS), cause of death, local control rate (LCR), regional control rate (RCR), failure pattern, common acute toxicities (based on descriptions in medical records, according to Common Terminology Criteria for Adverse Events, CTCAE 5.0), esophageal stricture, and dysphagia at the last follow-up were analyzed. OS was defined as the duration between diagnosis and any cause of death. DFS was defined as the duration between the diagnosis and any disease recurrence or any cause of death, whichever occurred first. CSS was defined as the duration between the diagnosis of EC and death. Estimates of OS, DFS, and CSS were derived using the Kaplan–Meier method. The subgroups were compared using the log-rank test. Independent prognostic factors were assessed using the Cox proportional hazards model. Differences in the distributions of adverse effects between the subgroups were assessed using Pearson’s chi-squared test or Fisher’s exact test as appropriate. Analysis items with two-sided P values < .05 were considered statistically significant. Data were analyzed using SPSS version 19.0. Survival curves were drawn using GraphPad Prism version 6.0.
Results
Patient Characteristics and Treatment Details
In total, 31 patients met the preset criteria and were included in the final analysis. Patient characteristics and treatment details are shown in Table 1. The median age was 62 years (range, 49-78). All patients had either submucosal invasion (83.9%), LVI (48.4%), or venous invasion (3.2%). The median infiltration depth of patients with submucosal invasion was 650 μm (range, 50-1550). Sixteen patients (51.6%) had comorbidities, with high blood pressure (22.6%) being the most common, followed by heart disease (19.4%) and diabetes (16.1%). The entire cohort of patients was diagnosed with a single lesion endoscopically and underwent complete ESD. The median time between the completion of ER and initiation of RT was 2.5 months (range, 1.2-5.8). The median dose of IMRT was 50.0 Gy (range, 44.0-60.0). Only one patient did not complete the prescribed radiation dose due to refusal. Twenty-two patients (71.0%) received ENI based on the tumor location. Six patients (19.4%) underwent concurrent chemoradiotherapy (CCRT). The regimens were paclitaxel liposome combined with platinum administered weekly (66.7%) or every three weeks (33.3%).
Patient characteristics and treatment details.

Muscularis mucosae invasion.
Submucosal invasion depth <200 μm.
Submucosal invasion depth ≥200 μm.
Abbreviation: LVI, lymphovascular invasion.
Survival and Cause of Death
The median follow-up time was 35.5 months (95% confidence interval, 28.1-42.8). The 1-, 3-, and 5-year OS rates were 100.0%, 86.9%, and 68.5%, respectively (Figure 1). The corresponding DFS rates were 100.0%, 85.2%, and 75.8%, respectively (Figure 2). The corresponding CSS rates were 100.0%, 89.8%, and 78.6%, respectively (Figure 3). The median survival times for OS, DFS, and CSS were not reached. No independent prognostic factors were observed for OS, DFS, and CSS. Five patients (16.1%) died, and the causes of death included EC (60.0%), heart failure (20.0%), and unknown reasons (20.0%). The patient who died of heart failure developed atrial fibrillation as a complication before RT and died 14.9 months after the completion of treatment without relapse.

Overall survival curve of the entire study cohort.

Disease-free survival curve of the entire study cohort.

Cancer-specific survival curve of the entire study cohort.
LCR, RCR, and Failure Pattern
By the last follow-up, the LCR of the entire cohort was 100.0%, and the RCR was 93.5%. Three patients (9.7%) experienced relapse, including one with DM and two with DM and regional LN recurrence synchronously. The DM sites included retroperitoneal LN (33.3%) and lungs (66.7%). The regions with LN recurrence were the recurrent laryngeal nerve (50.0%) and left gastric (50.0%) drainage regions. The details of the three patients are shown in Table 2.
Characteristics and outcomes of the patients with recurrence.
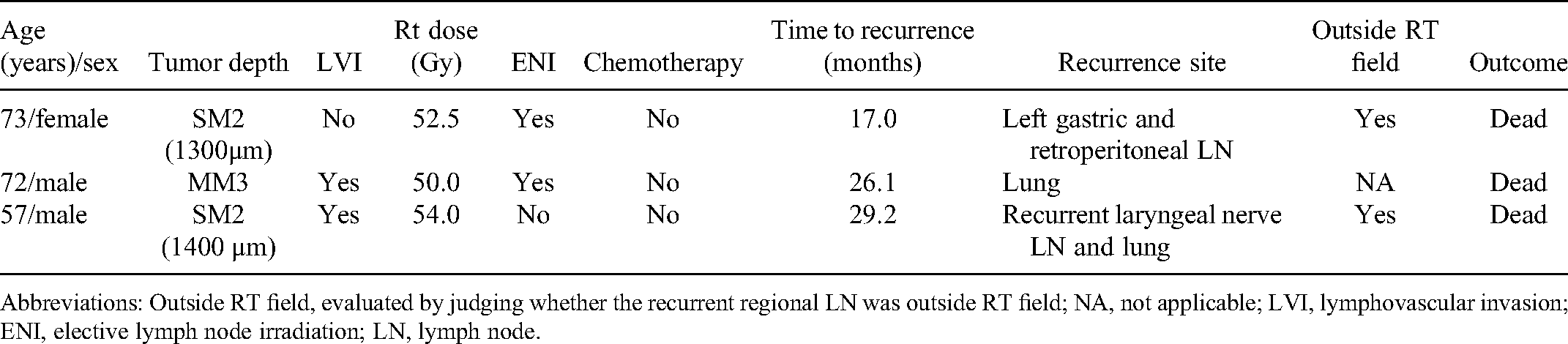
Abbreviations: Outside RT field, evaluated by judging whether the recurrent regional LN was outside RT field; NA, not applicable; LVI, lymphovascular invasion; ENI, elective lymph node irradiation; LN, lymph node.
Common Acute Toxicities, Esophageal Stricture, and Dysphagia at the Last Follow-Up
Common acute toxicities included esophagitis (Grade 1-2, 67.7%; grade 3, 12.9%), radiation pneumonitis (grade 1, 48.4%), leucopenia (Grade 1-2, 54.8%), and thrombocytopenia (Grade 1-2, 12.9%). No Grade 4-5 acute toxicities were observed. Fifteen (48.4%) patients were diagnosed with esophageal strictures endoscopically before RT, and seven (46.7%) of them underwent subsequent endoscopic balloon dilation. All seven patients (22.6%) with lesions involving ≥3/4 of the circumference were diagnosed with esophageal strictures. At the last follow-up, 28 patients (90.5%) were able to eat a regular diet, one (3.2%) could eat a soft diet, one (3.2%) needed a semifluid diet, and only one (3.2%) had to eat fluid. Dysphagia grades at the last follow-up of the 15 patients diagnosed with esophageal stricture were led to a giving of a regular diet in 80.0%, soft in 6.7%, semifluid in 6.7%, and a fluid diet in 6.7%. No statistically significant difference in dysphagia was observed between patients diagnosed with and without esophageal strictures (P = .315).
Discussion
The present study demonstrated that ER combined with RT was safe and effective for patients with stage I EC with submucosal invasion or LVI, with their swallowing function preserved. Thus, this treatment mode should be fully considered for patients with inoperable disease or for those wanting to preserve organ function.
Currently, chemoradiotherapy (CRT) or surgery is recommended by the Japan Esophageal Society for early stage EC patients with pT1b disease or LVI after ER. 11 Our data showed that ER combined with RT yielded an estimated 5-year OS of 68.5%, which was comparable to that of patients treated with surgery, ranging from 67% to 84%.12,13 Shimizu and colleagues conducted a prospective study in which superficial EC patients were enrolled to receive either ER followed by CRT or surgery. The results showed that the 5-year OS and CSS were similar between the groups (100% vs 88%, P = .21; 100% vs 91%, P = .34). 14 The JCOG 0508 trial reported a 3-year OS of 90.7% in early stage EC patients with LVI or pT1b, which reached its primary endpoint that the ER plus CRT arm could achieve better OS than the historically reported OS of surgery. 15 Binhao et al retrospectively compared the survival of superficial EC treated with ER plus RT or surgery based on data from seven institutions. They also found that there were no differences in 3-year OS and DFS between the groups (100% vs 84%, P = .18; 73% vs 76%, P = .39). 16 In addition, the reported local-regional recurrence rate, 5-year DFS, and CSS for early stage EC treated with CRT were 19%-26%, 34%-59%, and 54%-78% respectively,17–19 which were inferior to our results. Similarly, Yoshimizu et al 19 also reported that the 5-year relapse-free survival of the ER plus CRT group significantly improved compared to that of the definitive CRT group (85.1% vs 59.2%, P < .05). Taken together, the survival of ER followed by RT has the potential to be equivalent to that of surgery and better than that of definitive CRT.
CRT is a treatment option recommended by the Japan Esophageal Society for early stage EC patients with positive LVI after ER. 11 Several studies have shown that LVI is associated with an increased risk of LN metastasis in pT1a patients.2,9 A scoring system based on NCDB also showed that LVI was an independent risk factor for LN metastasis (odds ratio = 3.39, range 2.17-5.29). 10 In the JCOG 0508 trial, 14 pT1a patients with positive LVI were enrolled in the selective CRT group. In our study, pT1a accounted for 16.1% (5/31) of the patients, and all of them had LVI. 15 Among them, only one patient experienced a relapse. Moreover, two patients were diagnosed with esophageal strictures, and only one required balloon dilation. All five pT1a patients could eat a regular diet at the last follow-up. Therefore, we believe that additional radiotherapy after ER is necessary, effective, and safe for pT1a with LVI.
Of the three patients with relapse in our study, one patient had DM, while two had DM and regional LN recurrence synchronously, with no local recurrence observed. The most common modes of failure were regional LN and DM, and none of the patients received chemotherapy. Similarly, two retrospective studies also reported that LN recurrence and DM were the main failure patterns for superficial EC treated with ESD plus RT or CRT.20,21 Furthermore, Uchinami et al found that CRT showed a trend for better CSS than RT for patients with clinical T1N0M0 EC invading the muscularis mucosa or submucosa. 18 Thus, CRT other than RT alone may be a more reasonable additional treatment mode in terms of the failure pattern and more effective regional therapeutic effects of CRT. Regarding the characteristics of the three patients with relapse, two were diagnosed with SM2 disease or LVI, which hinted that RT alone might not be enough to cure cases with very high-risk factors. Similar results were observed in the JCOG 0508 trial, in which 11 patients experienced regional LN failure as the first site, and SM2 disease and LVI both accounted for 72.7% (8/11). 22 In addition, another retrospective study also observed that all four early stage EC patients who were treated with ER plus CRT and died of EC were diagnosed with ultra-deep submucosal invasion depth and LVI. 23 Therefore, a higher RT dose combined with chemotherapy or even surgery should be considered in this cohort of patients.
In our study, 46.7% of the patients diagnosed with esophageal strictures received subsequent endoscopic balloon dilation, and 86.7% (13/15) of them could eat a regular soft diet at the last follow-up. No statistically significant difference in dysphagia status at the last follow-up was observed between patients diagnosed with and without esophageal strictures (P = .315). Additional RT was safely applied in patients with esophageal strictures, and swallowing function was well-preserved based on effective endoscopic dilation. Furthermore, Hisano et al 21 reported a similar incidence of esophageal strictures in patients with mucosal defects involving ≥3/4 of the esophageal circumference after ESD in the RT and non-RT groups (33.3% vs 50.0%). Thus, esophageal strictures caused by ER may not be a contraindication to additional RT. According to the results of the JCOG 0502 trial, 57 (27.0%) of 211 clinical N0 patients had pathologic LN metastasis. 24 In other words, LN metastasis may be present in approximately 30% of patients with clinical T1N0 ESCC. Thus, the clinical diagnosis of T1N0 may not be sufficiently accurate. Nevertheless, in the JCOG 9708 trial, 87.5% (63/72) of patients with clinical stage I esophaheal squamous cell carcinoma (ESCC) achieved complete response after CRT, and the 4-year survival rate was 80.5%, which was comparable to that of surgery or ER. 25 Furthermore, in the JCOG 0508 trial, the 3-year OS rate was 90.7% in clinical stage I ESCC patients treated with additional CRT after ER. 15 In our study, a higher proportion of patients had SM2 (77.4%) or LVI (48.4%) than in the JCOG 0508 trial, which meant that more patients might have clinical occult LN metastasis in our cohort. However, the RCR was up to 93.5%, and the OS rates were comparable to those of surgery. Hence, even for ESCC patients with clinical occult LN metastasis, additional RT after ER is effective.
The present study had several limitations. First, this was a retrospective, single-center study. Second, the sample size was relatively small. Third, there was no control group to compare the effectiveness of ER plus RT and surgery. At present, a multicenter, prospective study (NCT number masked for peer review) has already been initiated by our institution, which could hopefully further validate the use of ER plus RT as a treatment modality.
Conclusions
In patients with stage I EC, additional RT following ER was safe and effective, with swallowing function well-preserved. Nevertheless, prospective studies are needed to verify these results.
Footnotes
Acknowledgments
We thank the support from CAMS Innovation Fund for Medical Sciences and all the patients, doctors, nurses, technicians participating in this study.
Ethical Approval
Ethical approval to report this case series was obtained from National Cancer Center/Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, National GCP Center for Anticancer Drugs, The Independent Ethics Committee, approval number 21/015-2686, date of approval May 18, 2021.
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects..
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by National Key R&D Program of China (2017YFC1311000), the CAMS Innovation Fund for Medical Sciences (CIFMS) (grant number 2020-I2M-C&T-B-074) and Beijing Hope Run Special Fund of Cancer Foundation of China.