
Abstract
Introduction
Whole-brain radiotherapy (WBRT) is a treatment modality frequently used for multiple cerebral metastases and is often performed for prophylactic cranial irradiation (PCI) of small-cell lung cancer. In the past, WBRT was performed in a bilateral two-portal manner involving radiotherapy of the whole brain, including the skull, skull base, and aural region.
Radiation-related hippocampal injury plays a major role in the development of cognitive dysfunction. The findings of the RTOG0933 study, performed by the Radiation Therapy Oncology Group (RTOG), were promising, showing that hippocampus-sparing whole-brain radiotherapy (HS-WBRT) was effective in reducing cognitive dysfunction.1,2 In addition, a comparative study of HS-WBRT + memantine and the usual treatment (WBRT + memantine) showed that HS-WBRT was superior.3,4 HS-WBRT is considered to be superior to the usual radiotherapy in terms of neurocognitive and quality-of-life outcomes, and HS-WBRT should be accepted as the new standard therapy for patients undergoing WBRT that have a favorable performance status. 5 In addition, three-phase III studies of PCI are currently in progress: NKI/AVL (ClinicalTrials.gov identifier: NCT01780675), NRG CC003 (ClinicalTrials.gov identifier: NCT02635009), and PREMIER-TRIAL (ClinicalTrials.gov identifier: NCT02397733). 6
HS-WBRT requires intensity-modulated radiotherapy (IMRT), and several studies have reported that tomotherapy was superior to other IMRT methods in terms of dose distribution.7-9 However, it was reported that volumetric-modulated arc therapy (VMAT) had an advantage in terms of irradiation time compared with tomotherapy, which takes more than 20 min while VMAT takes only a couple of minutes.7,8,10-13 Miura reported that tilting during tomotherapy shortened the irradiation time, and this reduction was only approximately 10%.13
Two methods have been proposed for shortening the irradiation time during tomotherapy: (1) reducing the modulation factor (MF) and (2) increasing the jaw width from 1 cm to 2.5 or 5 cm. In the case of complex treatment plans, it has been proposed that the responsible provider should start from a high MF, achieve a favorable conformal plan, and then reduce the MF until the dose quality is at a level that is not clinically tolerable.14,15 Van Gestel et al and Meyer et al18 examined the changes of the MF, jaw width, and pitch in oropharyngeal cancer and extremity sarcoma treatment plans, respectively.16-18
Ryczkowski et al19 reported a phantom test that showed that the MF affected the treatment plan quality and performance time. The resulting treatment plan showed no statistically significant difference from the initial treatment plan when the MF in the initial treatment plan was within the 6.0 to 1.8 range. In addition, the MF range from 6.0 to 3.0 demonstrated an approximately linear correlation with irradiation time. However, in treatment plans with an MF of 3.0 or lower, the irradiation time no longer decreased. Kerf et al20 reported that if the jaw width was 5 cm and the pitch was 0.2 or less, there were no changes in irradiation time with changes in MF. Therefore, even a marked reduction in MF does not necessarily shorten the irradiation time, and the appropriate selection of MF is clinically relevant for tomotherapy.
The tomotherapy radiation field is divided into 51 projections per gantry rotation. Each projection is further divided into 64 beamlets representing each one of the 64 multileaf collimators binary leaves (ie, the leaf being either open or closed). Inverse-planning optimization for tomotherapy requires the planner to choose an MF that is defined as the leaf-open time (LOT) max/LOTmean. The LOT of each beamlet that intersects a target volume determines the instantaneous radiation dose delivered from it through the projection arc or fraction thereof. IMRT is achieved by varying the LOT of each beamlet with inverse-planning optimization of the treatment plan. LOTmax is the maximum LOT, and LOTmean is the average of all beamlet LOTs.
The present study aimed to investigate whether by changing the MF in HS-WBRT, it is possible to shorten the irradiation time while maintaining the quality of the radiotherapy plan.
Materials and Methods
This was an exploratory study using computed tomography (CT) data from patients with cerebral metastases. An MT2013CF with a carbon-fiber tilting baseplate (CIVCO Radiotherapy) was used as a tilted head and neck fixation device for radiotherapy, and Aquarion LB was used for treatment-planning CT. At the same time, the brain, hippocampus, eye, lens, optic nerve, and chiasm contouring were assessed using T2-weighted and gadolinium-contrast-enhanced, T1-weighted magnetic resonance imaging. The hippocampal zone to be avoided was delineated with a 5-mm margin, and the planning target volume (PTV) was defined as the brain with this 5-mm hippocampal marginal zone excluded. The contour data obtained were combined with CT data using a RayStation (Ray Research Laboratories, Stockholm, Sweden; Table 1).
Structure Volume.

Note: Volume values are in cm3.
Abbreviation: PTV, planning target volume.
Optimization was performed using the TomoTherapy Planning Station (version 5.1.1.6; Accuray Inc.), as shown in Table 2. The prescribed radiation dose was 30 Gy applied in 10 subdivisions and was normalized to the isodose line, including 96% of the PTV. Calculations were made with MF at 3.0, 2.6, 2.2, 1.8, and 1.4. We reviewed whether the dose constraints (Table 3) presented in RTOG0933 were followed and the doses absorbed in the PTV and hippocampus and irradiation time was evaluated.
Optimization Constraints.

Note: D96% = 30 Gy in 10 fractions. (Max and Min constraints: 30 Gy, Importance and penalty: 240).
Jaw width: 1 cm, pitch = 0.200, iterations: 100.
Abbreviation: DVH, dose-volume histogram.
Dose Constraints.

All analyses were performed using BellCurve for Excel (Social Survey Research Information Co., Ltd). The differences among groups were analyzed using one-way analysis of variance and Scheffe post hoc test, and data are presented as mean values with standard deviation.
Results
We confirmed that all of the plans satisfied dose constraints in RTOG 0933 criteria shown in Table 3. The doses in the PTV and hippocampus are shown in Table 4. The dose-volume histogram (DVH) for one subject is shown in Figure 1. Dose conformality was thus maintained in both the PTV and hippocampus over the MF range 3.0 to 1.8, but the dose/MF relationship broke down when the MF was 1.4.
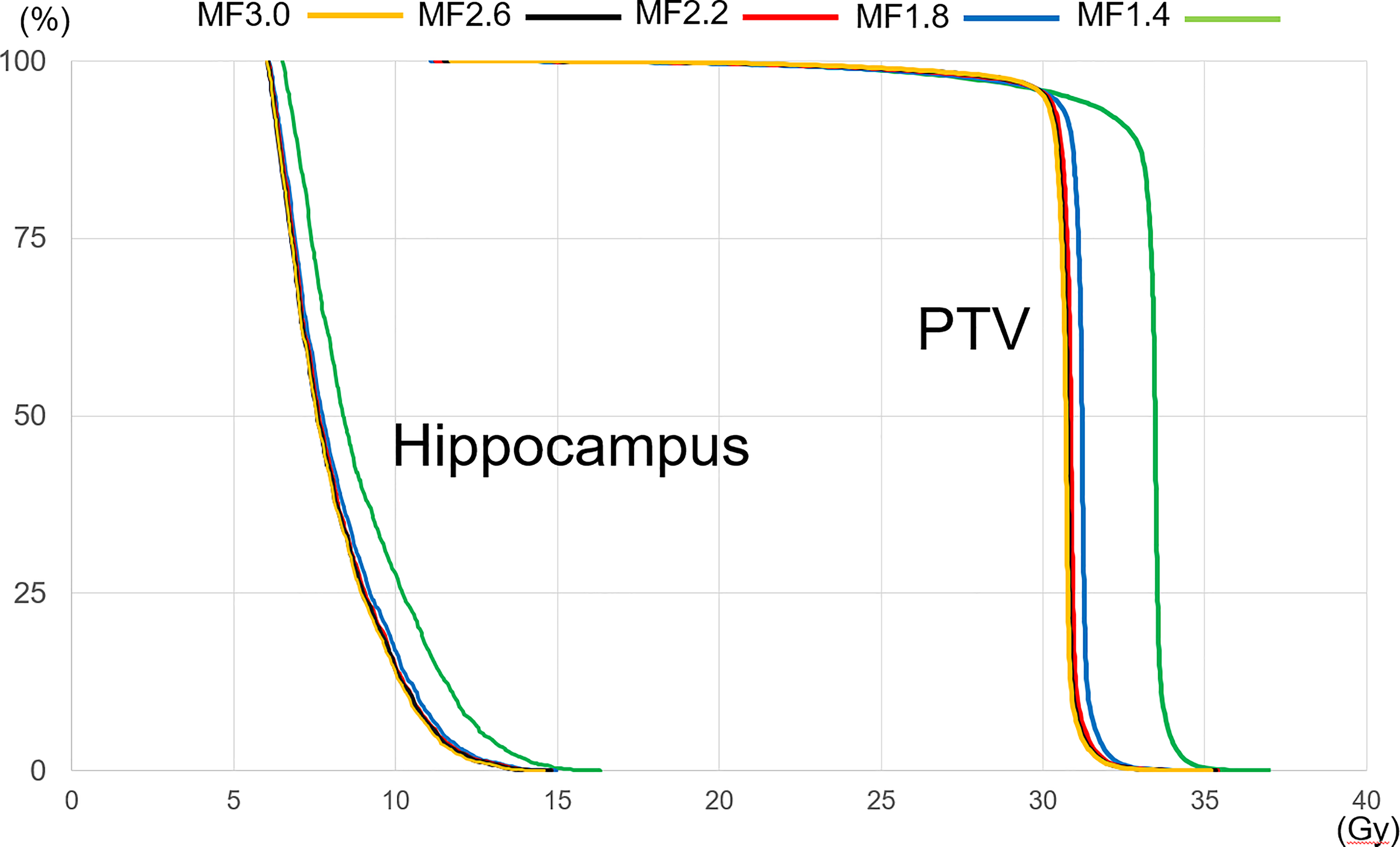
Example of a dose-volume histogram (case 3).
Results of Dose Parameters.
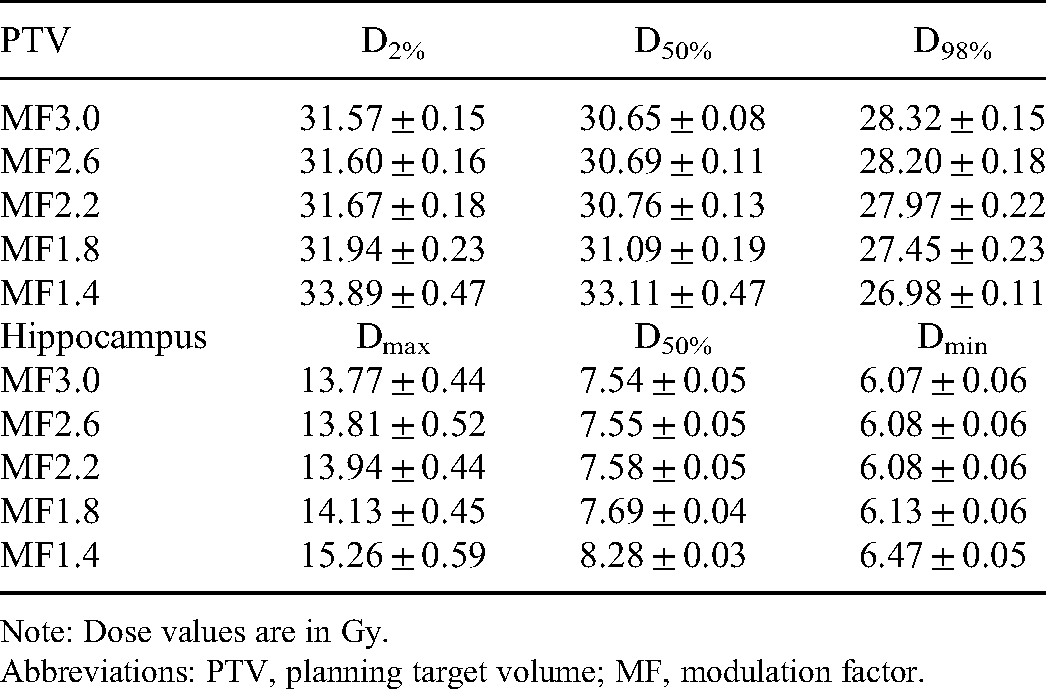
Note: Dose values are in Gy.
Abbreviations: PTV, planning target volume; MF, modulation factor.
In the Scheffe post hoc test, no significant differences were found in any of the six dose parameters in the PTV or hippocampus between when the MF was 3.0, and when it was 2.2 to 2.6. With an MF of 1.8, we found significant differences between the PTV D98% and hippocampus D50%, but not between the other four factors. However, when the MF was 1.4, all six factors showed significant differences from when the MF was 1.8, 2.2, 2.6, or 3.0. Figure 2 shows the irradiation time decreasing lineally from MF 3.0 to MF 1.8, and irradiation time for a plan with MF 1.8 was approximately 60% less than that with MF 3.0.

Irradiation time due to change in modulation factor (error bars: standard deviation).
Statistically significant differences in irradiation time were found between groups when the MF was 3.0, 2.6, 2.2, and 1.8, but no significant difference was found when the MF was 1.8 and 1.4 (P = .9995).
Discussion
HS-WBRT planning requires considerable time. There have been reports of attempts at optimization using autoplanning functions, resulting in successful standardization of plan quality,21,22 but these achievements were based on VMAT. The results of the present study showed that, as exhibited in Table 1, the dose constraint was considered to be effective when using a tilted fixation device with the jaw width of 1 cm and the pitch of 0.200.
MF affects the complexity of IMRT in tomotherapy; the higher the MF, the more conformal and consistent the target dose distribution is achieved. This relationship has the potential to improve sparing of important anatomical structures. In clinical practice, the MF is known to show marked variation between institutions,23 but in numerous previous reports, the MF in relation to HS-WBRT was taken to be 3.0,7,8,13 because the results of the RTOG0933 study were based on a jaw width of 1 cm and an MF of 3.0.24
In the present study, the dose parameters showed no statistically significant changes with MF reduction from 3.0 to 2.2. As shown in the DVH, it was possible to maintain the radiotherapy plan quality over the range within which the doses received by the PTV and hippocampus were not affected, that is, when the MF was reduced to 1.8. Over an MF range from 3.0 to 1.8, statistically significant differences were found only in two of six factors. In contrast, the hippocampal dose was markedly increased when the MF was reduced to 1.4, and the doses received by both the PTV and hippocampus were shown to increase significantly.
Nevertheless, although irradiation time showed a linear decrease over the MF range from 3.0 to 1.8, no difference was found between when the MF was 1.4 to 1.8. Generally speaking, MF has a direct impact on the treatment delivery time. Because the linear accelerator dose rate, couch speed, and gantry period are constant during helical treatment delivery, the total time for “beam-on” delivery is a product of the number of gantry rotations and gantry period. The number of gantry rotations is determined by the pitch and length of the cranial-caudal treatment volume plus jaw width. The gantry period is equal to 51 × LOTmax, unless LOTmax is < 0.235 s, in which case the gantry period minimum is reached at 11.8 s. Therefore, for gantry periods longer than 11.8 s, the irradiation time is obtained using the following formula25:
Irradiation time = 51 × LOTmax × number of active gantry rotations
In the present study, in all subjects, the gantry period was 11.8 s when the MF was 1.4, and it is therefore considered that no shortening of the gantry period occurred. However, when the MF was 1.8, the gantry periods were 12.0 and 11.8 s in four and two subjects, respectively. Accordingly, it is considered that an MF of 1.8 is optimal to shorten the irradiation time.
Nevertheless, in the treatment plan with an MF of 1.8, the irradiation time was approximately 60% of that with an MF of 3.0, but the irradiation time was approximately 13 min. Even with VMAT, there was no comparison of the irradiation times. However, it has been reported that when a simultaneously integrated boost was performed with the cerebral metastases, in addition to HS-WBRT,26 an increase in jaw width from 1 to 2.5 cm resulted in shortening of irradiation time from 21.8 ± 1.8 to 10.2 ± 1.0 min. In this respect, a limitation was that changing the MF shortened the irradiation time. In general, when a treatment plan is prepared with a jaw width of 5 cm, irradiation can be provided in one-third of the time than that with a jaw width of 1 cm, and in half the time with a jaw width of 2.5 cm.27,28 Future studies should consider evaluating performance with jaw widths of 2.5 and 5 cm.
Conclusions
With HS-WBRT in the tilted body position, a jaw width of 1 cm, and an MF of 1.8 a well-balanced combination would be achieved between the favorable conformal plan and irradiation time. With an MF of 1.4, the radiotherapy plan quality deteriorated, and the irradiation time was approximately the same as that with an MF of 1.8. Thus, there is a limit to the degree to which irradiation time can be shortened by changing the MF, and studies relating to jaw width will be required in the future.
Footnotes
Authors’ Note
Our study was approved by the Ethics Committee of Affiliated JCHO Tokyo Shinjuku Medical Center (approval no. R2-14).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.