
Abstract
Keywords
Introduction
Prophylactic cranial irradiation (PCI), which eliminates micrometastases in the brain and brainstem via whole-brain radiotherapy (WBRT), is the standard treatment for preventing brain metastases;1,2 however, an early retrospective study on small cell lung cancer showed that 12.5% of patients had memory loss, ataxia, and body weakness after WBRT. 3 Other investigations related to the radiation therapy oncology group (RTOG) 0212 trial revealed that chronic neurotoxicity occurred in 62% of patients receiving PCI.4,5 Damage to bilateral hippocampal tissues (BHT) will inevitably affect patients' advanced neural activities, such as emotions, learning, and memory, and decrease the quality of life (QOL). Preclinical models have demonstrated that hippocampal radiation leads to the loss of hippocampal spatial learning and memory-dependent functions. 6 In the NRG CC001 trial, hippocampal avoidance during WBRT (HA-WBRT) improved neurocognitive function and QOL compared with WBRT. 7 Therefore, the BHT must be spared during WBRT.
According to Gondi et al, 8 intensity-modulated radiotherapy (IMRT) can be used to design BHT-sparing PCI plans. Jiang et al 9 compared the dosimetry characteristics of helical tomotherapy (HT), co-planar dual Arcs volumetric-modulated arc therapy (VMAT-2 ARC), and fixed-beam IMRT in PCI therapy and found that HT provided a better target dose homogeneity index (HI) (HI = 0.39, P < .05), followed by VMAT-2 ARC (HI = 0.57, P < .05). However, there are very few clinical data on the relationship between the dose the hippocampus is exposed to and its dysfunction. Gondi et al 8 reported that exposing 40% of the BHT to >7.3 Gy was associated with an impairment in delayed recall (P = .043). Therefore, it is believed that a reduced BHT irradiation dose would lead to a decrease in the risk of neurocognitive dysfunction. However, excessive hippocampal dose reduction could result in unacceptably large low-dose areas and unconformable dose distribution in the PCI planning target volume (PTV). Therefore, dose distribution guidelines focusing on hippocampal sparing could provide reference to physicians when choosing between optimized radiotherapy strategies based on both target coverage and hippocampal sparing.
This study aimed to explore the capabilities and characteristics of HT and VMAT-2 ARC in sparing the hippocampus, establish guidelines on dose variation to the PTV, and propose a balance between hippocampal sparing, and conformity, homogeneous dose to the PTV.
Materials and Methods
Hippocampus and Inner ear Delineation
Sixteen patients who underwent PCI were enrolled in this study. The BHT were contoured on T1-weighted magnetic resonance imaging axial sequences fused with contrast-enhanced computed tomography images according to RTOG guidelines. Ghia et al 10 demonstrated that only 3.3% of metastases are located in the perihippocampus within 5 mm, and no metastases lie within the hippocampus. BHT + 5 mm 3-dimensional extensions were therefore defined as hippocampal avoidance regions (HAR).
The middle ear and bilateral main structures of the inner parts of the ears, including vestibular organs and cochlea, were delineated at a window width of 3000 to 4500 and window level of 400 to 800.( 11 )
Prescription Dose and Planning Scheme
Whole-brain tissue was defined as the clinical target volume (CTV). The PTV was defined as CTV minus the HAR. For each patient, HT and VMAT-2 ARC treatment plans were designed using a prescription dose of 30 Gy/10 fractions. For each patient, the initial plan was drawn in accordance with the conventional PCI planning method, which only met the PTV and OAR dose constraints without BHT dose limitation. When the PTV dose met the clinical prescription requirements, the dose-volume constraints of BHT and their corresponding weights were increased gradually to decrease the dose to BHT. During the plan optimization process, the dosimetry parameters of BHT, HAR, PTV, and OARs, including Dmean_BHT, D98%_BHT, D2%_BHT, D98%_PTV, D50%_PTV, D2%_PTV, and the conformal index (CI) and HI of PTV, Dmean-inner-ear, Dmean-parotid, Dmax-lens, Dmax-optic nerve, and Dmax- brainstem were statistically recorded whenever the mean dose to BHT decreased by 4 Gy. The dosimetry parameters listed above, as well as the dose delivery duration variation, were plotted following the BHT dose-decrease steps.
Dosimetric Evaluation
According to the dose-volume histogram (DVH) of the formula proposed by Paddick
12
:
The formula most commonly used to calculate HI is as follows
13
:

Statistical Analysis
Origin 2018 software (OriginLab) was used to draw line charts to present the trend in the PTV and OARs dose variation in sparing BHT. Statistical analyses of the results obtained from the 2 planning schemes were performed using SPSS software (IBM Corp.). A nonparametric analysis of the Willis rank test was used to determine differences, which were considered significant at P ≤ .05.
Results
Hippocampus Contouring
The characteristics of the 16 patients are presented in Table 1. The hippocampus, HARs, and whole brain volumes were 5.02 ± 1.21 cm3 (3-7.7 cm3), 33.79 ± 6.97 cm3 (13-44.4 cm3), and 1580.69 ± 179.12 cm3 (1295.6-1890.9 cm3), respectively. The HA and HAR volumes accounted for 0.32 ± 0.08% (0.20-0.47) and 2.18 ± 0.47% (1.57-2.72), respectively, of the whole brain volume.
Characteristics of 16 Patients with PCI.

Abbreviations: PCI, prophylactic cranial irradiation; CTV, clinical target volume; HT, helical tomotherapy; VMAT, volumetric-modulated arc therapy.
Comparing Dose Variation Trends in PTV
The dosimetric evaluation for the OARs is shown in Table 2. Both HT and VMAT-2 ARC spared the hippocampus, and all plans met the dose constraints of the clinician as indicated. Figure 1 presents the HT and VMAT-2 ARC plans when the hippocampal dose was unconstrained and limited to 12 Gy.

The dose distribution of TOMO and VMAT plans. (a) The TOMO and VMAT plans when the BHT dose was limited BHT to 28 Gy and (b) both the 2 plans limited BHT to 12 Gy.
Average Dosimeteric Evaluation for OARs According to the 2 Planning Modalities.

Each value was calculated from the date for all 16 patients, and show the corresponding dose volume parameter when the average hippocampal dose is limited to 28 Gy, 24 Gy, … etc.
Abbreviations: HT, helical tomotherapy; VMAT, volumetric-modulated arc therapy; Dmax, maximum dose; Dmean, average dose; Dmin, minimum dose.
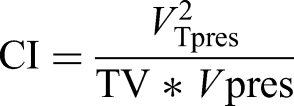
For the brain PTV (PTV_brain), HT provided a lower average D2%_PTV (P = .02), a higher average D98%_PTV (P = .22), and the best CI (P = .02) and HI (P = .05). The plots including Dmean_PTV, D2%_PTV, D98%_PTV, CI_PTV, HI_PTV, PTV_V30Gy, and treatment duration are shown in Figure 2.
The variation trends in HARs, D98%_PTV, D50%_PTV, D2%_PTV in (a), the variation trends in target coverage percentages of CI, HI, (PTV_V30Gy), and plan delivery in (b) during the BHT sparing process.
During the reduction of the dose to the BHT, the Dmean_PTV and D2%_PTV variations in both treatment plan modalities were stable, and there were variations in D98%_PTV across 3 different regions in the HT plan: the plateau region (>20 Gy), gradient region (∼20 to ∼12 Gy), and falling region (<12 Gy). The VMAT-2 ARC plan, like the HT plan, also had 3 different regions with thresholds of 16 Gy and 11 Gy. There was almost no impact on PTV dosimetry factors at a Dmean_BHT not lower than 12 Gy (not lower than 11 Gy for VMAT-2 ARC). The decrease in the dose to the hippocampus led to a linear and slight decrease in the CI with HT; however, for VMAT-2 ARC, the CI was severely impaired at a Dmean_BHT lower than 11 Gy and failed to register at a Dmean_BHT below 10 Gy. For both treatment plan modalities, the HI was severely decreased in the falling region.
Comparing Dose Variation Trends in OARs
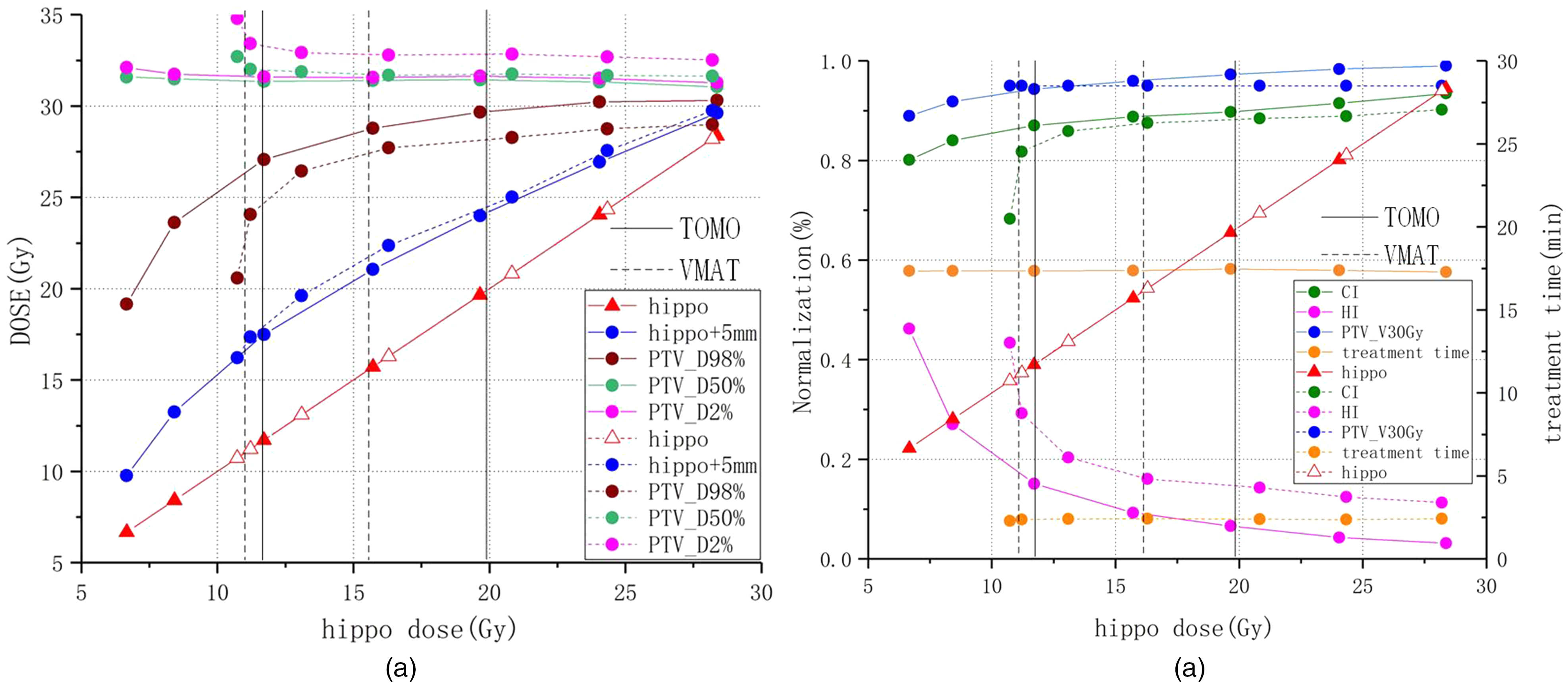
All plans met the RTOG 0933 protocol dose restriction criteria for sparing BHT. The dose variation to each OAR during the BHT dose decrease is shown in Figure 3. The Dmean-BHT(P = .03), D98%-BHT(P = .01), D2%-BHT(P = .01), Dmean-inner ear (P = .02), Dmean-parotid gland (P = .02), Dmax-Lens (P = .02), and Dmax-brainstem (P = .02) were lower in HT than in VMAT-2 ARC, but there was no significant difference in Dmax-optic nerve (left, P = .87; right, P = .39) between the 2 plans. When BHT were restricted to 8 Gy, D40%mean-BHT = 7.64 ± 0.41 Gy (>7.3 Gy) in HT, while D40%mean-BHT = 10.96 ± 0.38 Gy (>7.3 Gy) in VMAT-2 ARC, and the variation tendency of D40%mean-BHT is shown in Table 2. HT protected OARs better than VMAT-2 ARC. A decrease in the dose to the BHT resulted in an almost linear decrease in the doses to the HAR and D98%-BHT, but the doses to OARs did not change significantly when using HT. For VMAT-2 ARC, there were variations in the doses to OARs in 3 different regions: the plateau region (>16 Gy), slow-growth region (∼16 to ∼11 Gy), and sharp increase region (<11 Gy). However, in the optic nerves, the dose dropped when the dose to the hippocampus was <11 Gy.
The variation trends in D98%_hippo and D2%_hippo in (a), Dmean-BHT, Dmean-inner−ear, Dmean-parotid, Dmax-lens, Dmax-optic nerve, and Dmax-brainstem in (b) during the hippocampus sparing process.
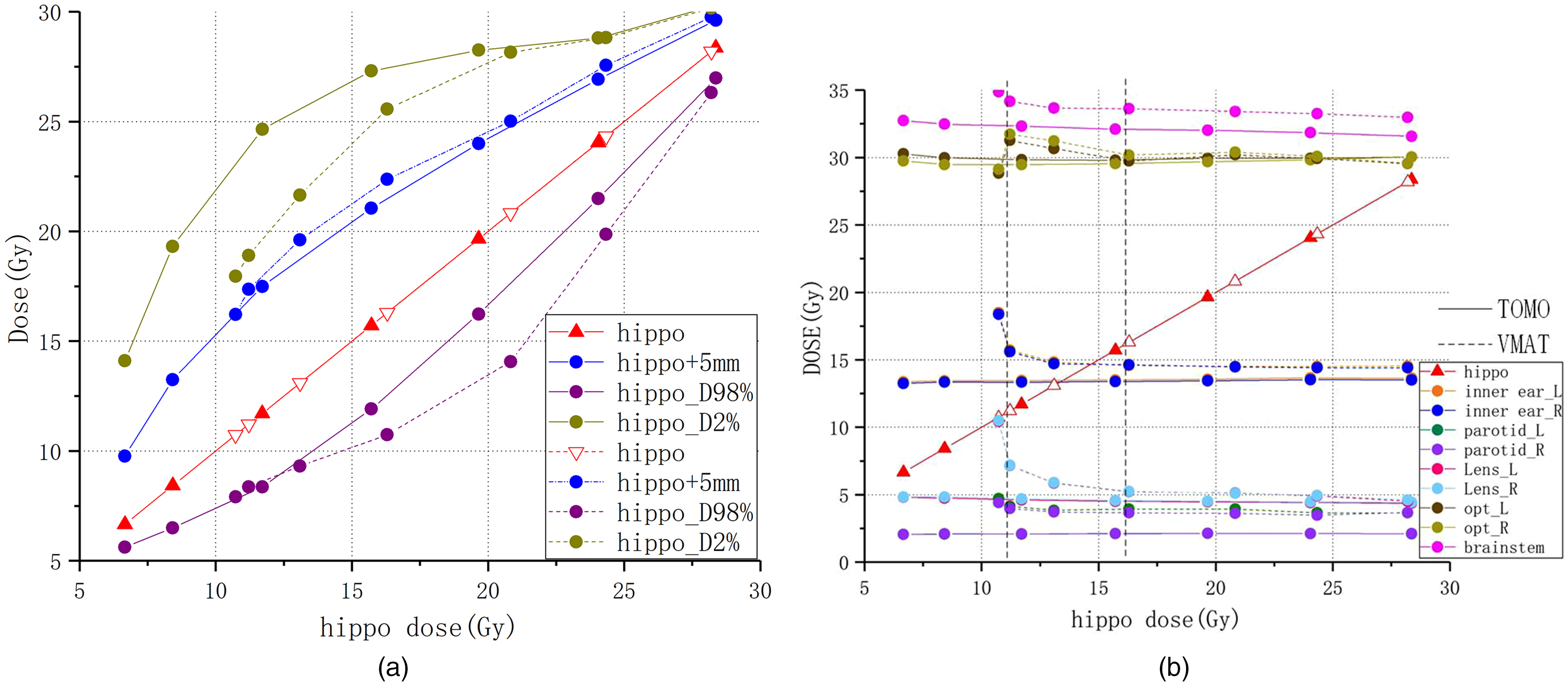
Given that HT provided better PTV coverage, a series of transversal dose distributions on the HT treatment planning system (TPS) was proposed, as shown in Figure 4, for the visual presentation of the PTV coverage variation at different observation points.
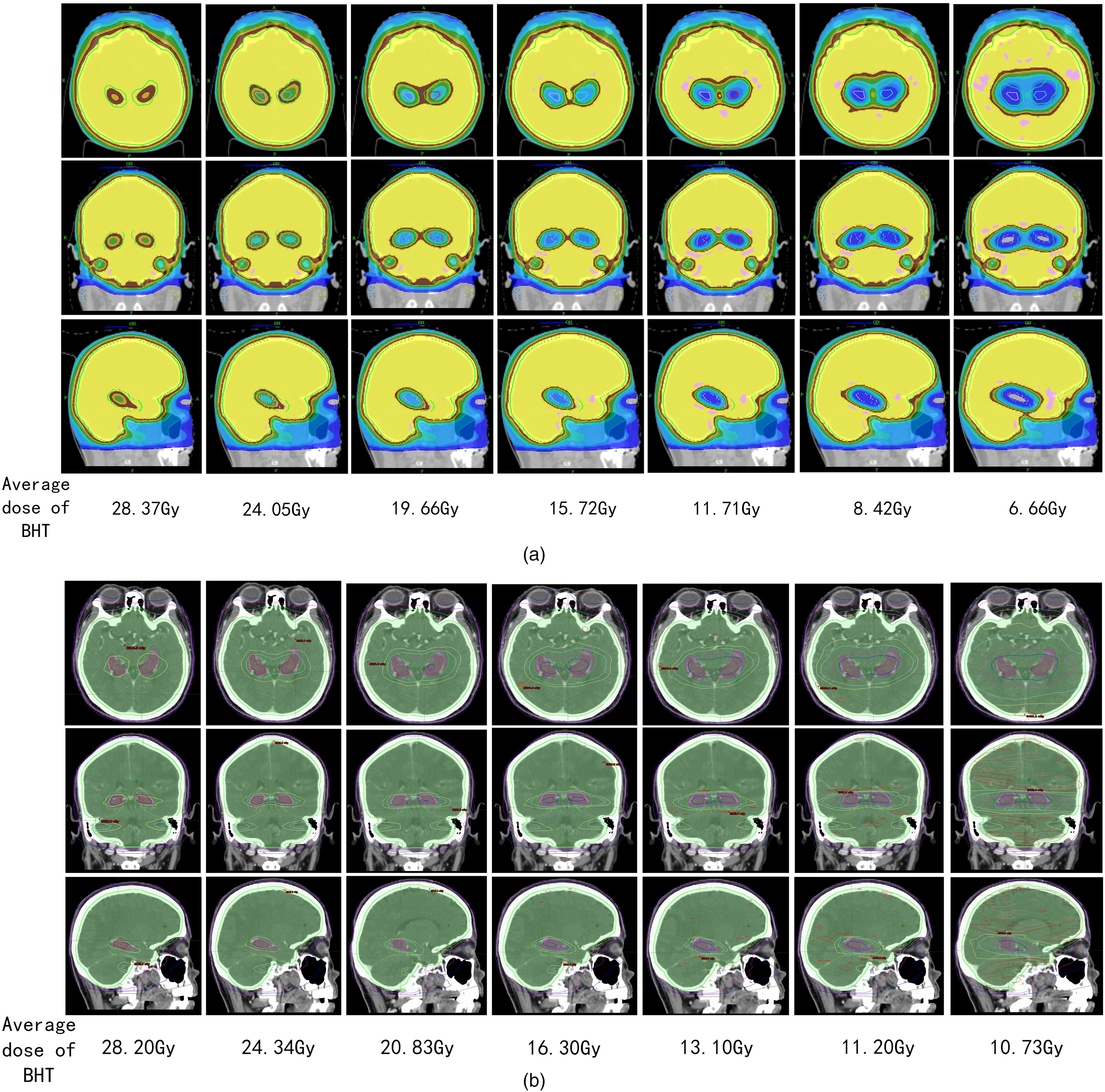
The dose distribution of TOMO and VMAT plans. A series of transversal dose distributions on the HT treatment planning system (TPS) (a) and VMAT TPS (b) at different observation points. All data were derived from the same cross-section of different plans for the same patient.
Comparing Treatment Duration
For the same prescription dose, HT (17.36 ± 0.05 min) and VMAT-2 ARC (2.38 ± 0.04 min) yielded distinct delivery durations for each fraction. Furthermore, as Figure 2b and the standard deviation show, during the reduction in the dose to BHT, treatment with the same technique had a similar delivery duration at each observation point. The average delivery duration of HT was almost 7.7 times longer than that of VMAT-2 ARC.
Discussion
It is believed that the dose to BHT should be as low as possible in PCI radiotherapy to mitigate the risk of irradiation-induced toxicity. However, the dose to the BHT and PTV coverage were directly associated. This study proposes dose distribution variation guidelines to promote hippocampal sparing when using HT, which could provide reference to physicians choosing between optimized HT plans based on both target coverage and hippocampal sparing.
The Importance of Sparing the Hippocampus
The emergence of new treatment technologies and drugs (including immunity and targeting) has enabled the continuous prolongation of the median overall survival of patients with brain metastases up to 35.5 months, particularly in those with oligometastatic tumors. 14 The hippocampus is located at the center of the brain,( 15 ) and is responsible for memory and cognitive functions. 16 No WBRT radiotherapy technique can completely avoid irradiation of the BHT. However, patients expect to survive longer and with high QOL after treatment. Therefore, protecting the hippocampus during treatment is of great significance. Conformal sparing of BHT would ultimately reduce the occurrence of neurological dysfunction without affecting treatment effects.16,17 Given that HA-WBRT reduces the radiation dose to BHT, it could lessen neurocognitive sequelae, but that would occur at the cost of a slightly reduced efficacy. 18
Hippocampus and HAR Delineation
The hippocampus is derived from neural stem cells, and its memory function is associated with pyramidal cells and granular cells located in the dentate gyrus of the hippocampus. 19 New hippocampal granulosa cells are produced by mitotically active neural stem cells and migrate from the subgranular region of the dentate gyrus to the granular cell layer.20,21 Monje et al 22 showed that radiation side effects are caused by inflammation around neural stem cells. In Monje's established mouse model experiment, the author observed that a single fraction dose of 10 Gy reduced the proliferation of neural stem cells by 62% and hippocampal neurogenesis by 97%. 23 However, instead of complete hippocampal formation, we focused on the dentate gyrus granulosa subregion. Since the gray matter predominated in the hippocampus, T1 hyposignals on the inner side of the temporal horn were mainly delineated.
When Ghia et al 10 enrolled 272 patients with confirmed brain metastases, 3.3% (n = 9) of the metastatic tumors were located within 5 mm of the hippocampus, while 86.4% were located more than 15 mm from the hippocampus (n = 235). Therefore, the hippocampus + 5 mm regions were regarded as the HAR. The volume of the BHT was larger compared to the contours defined by Gondi et al 16 In this study, 16 patients with PCI were enrolled in comparison with 5 patients with simultaneous integrated boost (SIB) in Gondi et al.'s study. Although the volume was larger than Gondi et al, the HAR occupying 2.18% of the whole brain volume which similar to 2.1% in study of Gondi et al; and the volume obtained in this study was close to the results of Bergouignan et al. 24
The Effect of Radiotherapy Technologies
HT is considered an advanced radiotherapy technology with higher intensity modulation capabilities for flexible delivery angles and finer beamlets, and it provides dosimetric advantages by combining a continuously rotating gantry with a binary multileaf collimator. 25 On the one hand, HT delivers fine beams with a transversal area smaller than 1 cm2 from 51 angles, and the design of pneumatic binary multileaf forms more subfields quickly. On the other hand, superiority of HT was evidently a product of “serial isocenter line” type of delivery versus single isocenter point of VMAT type of delivery. Besides, the contour of hippocampal changes greatly between layers, and the dose drop of HT in Y-axis is faster than that of VMAT. Therefore, HT delivers prescription doses with higher conformability and steeper edge gradient to the hippocampus. Compared with conventional VMAT technology, HT has greater target conformity and is better at sparing OARs, resulting in a biologically effective dose escalation. 25 Furthermore, the HT TPS has the option to set a “complete block” to OARs, which would enable the TPS to set no irradiation beams on the path of such OARs in order to avoid BHT irradiation. This maneuver may explain why our HT plans were more homogeneous and conformal while providing lower BHT doses, which is consistent with a previous finding by Jiang et al 9 that both HT and VMAT radiotherapy modalities are acceptable treatment methods with good avoidance of the hippocampus and inner ear, but that HT possesses superior PTV coverage and homogeneity. Kothavade et al 26 compared stereotactic conformal radiotherapy (SCRT), IMRT, and tomotherapy, and found that tomotherapy and linear accelerator (LINAC)-based IMRT yielded significantly better PTV coverage than SCRT. In their research, Gondi et al 16 showed that the mean dose to the BHT (normalized to 2-Gy fractions) reduced by 87% to 0.49 Gy2 using HT and by 81% to 0.73 Gy2 using LINAC-based IMRT. Therefore, HT irradiation technology is the best WBRT option for sparing BHT.
The Interpretation of CI and HI Parameters
CI is an extension of layer-by-layer dose analysis and DVH, and it can objectively measure the conformity between the prescription dose volume and the PTV. In this study, CI closer to 1 indicated that the treatment plan was better optimized. To the best of our knowledge, our study is the first to restrict the dose to BHT using a gradient and then observe the variation in target coverage, dose distribution, and doses to OARs. We found that the CI decreased slowly when using HT, and as the dose to BHT decreased, there was almost no significant impact on PTV conformity. However, when using VMAT-2 ARC, the CI was stable when the dose to BHT was higher than 11 Gy, but dropped rapidly when the dose to BHT was lower than 11 Gy, suggesting that a dose higher than 11 Gy meant that a better target coverage plan could be established, with a slightly worse target conformity, but a dose lower than 11 Gy implied that the target coverage was unsatisfactory, and the treatment plan would not meet clinical requirements.
HI is an index used to analyze and quantify dose homogeneity within the PTV, with lower values indicating greater homogeneity. As shown in Figure 2(b), HI also harbored 3 different regions with BHT sparing: the plateau region, slow-growth region, and sharp increase region, revealing that the homogeneity of dose distribution in the PTV is stable when the dose to BHT is higher than 20 Gy (higher than 16 Gy for VMAT-2 ARC). If the dose to BHT declines to 12 to 20 Gy (11-16 Gy for VMAT-2 ARC), the homogeneity of the dose distribution in the PTV becomes poorer due to the appearance of hot and cold spots. If the dose to BHT declines further to less than 12 Gy (11 Gy for VMAT-2 ARC), the homogeneity further deteriorates, indicating that the TPS may have reached the limit of optimization.
Treatment Time
A drop in the radiation dose to the hippocampus yielded no significant variations in plan delivery durations in both plan modalities, possibly because the planning modulation factor for all HT plans was 0.22 or 0.2, the pitch value was 0.233, and field width was 1.05 cm; these were the factors affected the plan delivery duration and were fixed in all patients; thus, no significant changes were noted. Meanwhile, the monitor unit values of all VMAT-2 ARC plans ranged from 501 to 720, with corresponding plan delivery durations ranging from 138 to 145 s. The average delivery duration for HT was almost 7.7 times longer than that of VMAT-2 ARC, which contributed to the narrower collimation, lower pitch, and smaller field width. 27
In this study, all patients received prophylactic WBRT, and as the BHT dose decreased, there was no significant change in the radiotherapy planning time in either treatment modality. In practice, from prophylactic WBRT to SIB will prolong the radiotherapy planning time, and the more brain metastases, the longer the treatment time, but this trend is not seen in Figure 2(b). The treatment time is variable in patients with WBRT and brain metastasis, and we should also pay attention to the changes in treatment time while sparing the hippocampus.
OAR Exposure Analysis
Regarding the sparing of OARs by WBRT, HT and VMAT-2 ARC yielded significant differences in most organs. The doses to BHT, inner ear, parotid gland, lens, and brainstem were lower in HT than in VMAT-2 ARC, but there was no significant difference in the doses to the optic nerves between the 2 modalities. These findings are consistent with the results of Rong et al 27 demonstrating the advantage of HT in sparing the hippocampus and lenses but not optic nerves.
The radiation doses to OARs in the HT plan were stable, but in the VMAT-2 ARC plan, there were variations in doses to OARs across 3 different regions: the plateau region (> 16 Gy), slow-growth region (∼16-11 Gy), and sharp increase region (<11 Gy). However, the dose to the optic nerves dropped when the dose to the hippocampus was less than 11 Gy, possibly because of the higher intensity modulation capability and the faster dose falloff seen in HT. 16 In VMAT, to reduce the dose to the hippocampus, the rays emitted to the hippocampus were reduced, as was the irradiation to the PTV. A portion of the optic nerves is located in the PTV; therefore, the dose to the optic nerves was insufficient, primarily because the modulation capacity of VMAT-2 ARC is relatively poor. Therefore, VMAT TPS optimization was limited in its capacity to reduce the dose to the hippocampus, which meant that the path of the ray was transformed, and more energy was deposited in the peripheral OARs. This outcome would also explain why the OARs failed to meet the clinical limit when the dose to the hippocampus was lower than 11 Gy.
Multicriteria Optimization
Multicriteria optimization (MCO) is a system that provides a real-time assessment of the tradeoff between multiple objectives and designs a theoretical optimal scheme. Ghandour et al 28 compared VMAT and MCO-VMAT in patients with prostate cancer; although there was no significant difference in V95%, D1%, CI, and HI, MCO-VMAT reduced the treatment planning time and improved the treatment efficiency. Zieminski et al 29 demonstrated that MCO-VMAT was the optimal modality for HA-WBRT in terms of PTV coverage, OAR sparing, and delivery efficiency, compared with MCO-IMRT or standard optimization VMAT (STD-VMAT), and achieved a mean BHT dose of ∼9 Gy with VMAT. Zieminski et al 29 used a third nonplanar vertex arc. Despite achieving better CI, the noncoplanar arc was generated extra radiation and damaging the organs in the long axis direction; while considering that HT only perform 360° continuous rotation around the mechanical iso-center, therefore, the same optimized conditions be set and coplanar dual arcs applied to VMAT in this study. The use of multiple arcs has been confirmed to produce optimal plan quality. 30 PTV coverage was 95% in this study, which is higher than in Zieminski et al's study 92.75% (MCO-VMAT) and 87.94% (STD- VMAT), while the maximum dose of 31.9 Gy (106.4% prescription dose) was similar to that of Zieminski et al: 39.66 (106.4% prescription dose with MCO-VMAT) and lower than 41.96 Gy (111.9% prescription dose with standard optimization—VMAT).
Numerous studies have shown that MCO improves plan quality over conventional plan modalities.31–33 Automatic optimization has broad prospects in the future and improves the level of artificial planning.
Limitations
One of the limitations of this investigation was the relatively small sample size. What we achieved was merely a simple technical comparison. Further prospective clinical confirmation trials are needed to obtain more accurate conclusions.
Conclusion
Compared to VMAT-2ARC, HT performed better in sparing the hippocampus and OARs, yielding better target coverage during radiation therapy. However, the use of HT requires a significantly longer treatment duration. Further decreases in the BHT dose than stipulated yield poorer target dose coverage, presenting a ‘3 regions’ stair-stepping characteristic.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This work was supported by the National Natural Science Foundation of China (grant numbers 82172072); the Shandong Provincial Natural Science Foundation (ZR2020LZL001); the Taishan Scholars Program of Shandong Province (Young Taishan Scholars, No. tsqn201909140); the National Key Research and Develop Program of China (grant number 2016YFC0105106).