
Abstract
Introduction
Glioblastoma multiforme (GBM) has a very poor prognosis with a median survival time of 14 to 15 months,1,2 using standard therapy with concurrent postoperative radiotherapy and oral chemotherapy for 6 weeks, followed by maintenance chemotherapy. Recently, the novel approach of tumor treating fields (TTFields) utilized after completion of radiotherapy has been demonstrated to improve survival outcomes in a randomized trial. 3 For patients not enrolled in clinical studies, the current clinical treatment paradigm is to first complete 6 weeks of radiation therapy, followed with TTFields therapy concurrent with maintenance Temozolomide (TMZ). Preclinical data suggest that using TTFields concurrently with radiotherapy treatment may further improve outcome. 4 We have previously determined that with the TTFields arrays in place but powered off, radiation dosimetry is appropriate 5 and that it is possible to accurately target a head phantom by using a cone-beam CT for alignment.6,7 In this work, a dedicated robotic radiosurgery system is used to assess idealized accuracy and stability of radiation targeting through the arrays while TTFields are being delivered. The role of radiosurgery for GBM has previously been reviewed 8 and is not the topic of this paper, but the accuracy of radiation delivered through TTFields is best measured by stereotactic systems because of their improved accuracy.
TTFields acts as an antimitotic treatment method that works by delivering electric fields in the frequency range of 100 to 300 kHz via ceramic transducer arrays placed directly on the skin. 9 Cell line studies have shown that TTFields may interfere with the assembly of spindle microtubules in lung adenocarcinoma cells while inducing cellular multinucleation and chromosome segregation. 10 Similar phenomena were observed in vivo in F-98 glioma cells. 10 In ovarian A2780 cells, TTFields was shown to induce apoptosis in actively dividing tumor cells. 10 TTFields is also currently being investigated as a therapy for treating several extracranial indications such as mesothelioma (NCT02397928) which has completed, 11 lung (NCT02973789), 12 pancreas (NCT03377491), 13 hepatocellular (NCT03606590), 14 and ovarian cancer (NCT03940196). 15
A randomized phase 3 clinical trial EF-14 showed that TTFields with maintenance TMZ therapy resulted in improvement in progression-free survival and overall survival in newly diagnosed GBM patients. In the patient group treated with TMZ plus TTFields, median progression-free survival was 6.7 months (95% CI 6.1-8.1) compared to 4 months (95% CI 3.8-4.4) in patients treated with TMZ alone with a 40-month median follow-up period. 3 This study also showed that there were no clinically significant differences in side effects in both groups. A study by Ballo et al 16 examined the effect of field strength 17 in a simulation-based study of 340 patients from the EF-14 study by combining factors of power density and compliance into a single measure of dose. These researchers showed a correlation between TTFields dose density (product of average power density in the tumor and device usage) and overall patient survival. Patients with dose density >0.770 mW/cm3 had a longer progression-free survival of 8.5 months compared to 6.7 months in patients with dose density <0.770 mW/cm3. Patients with both power density >1.15 mW/cm3 and device usage >75% had a median overall survival increase of 4 months over patients with power density <1.15 mW/cm3 and device usage <75%. 16
The combined treatment of TTFields, radiotherapy and TMZ following tumor resection was found to be safe and well-tolerated. 18 In the study of Li et al, 19 the presence of TTFields electrodes demonstrated only a very minor impact on the radiotherapy dose delivered to the target site, but large differences at the skin surface. When the ceramic electrodes were left in place but powered off during radiation treatment, 80% of patients developed local dermatological complications graded as CTCAE grade 1 to 2, but no grade 3 or higher toxicities were encountered. 20 Recommendations on scalp saving measures were advised.5,19,20
Concurrent TTFields therapy with radiation is defined as both therapies delivered during the same period of time but not given simultaneously. To differentiate from prior studies on concurrent therapy, we define “simultaneous” as delivering both therapies at the same time, with the TTFields device powered on while the radiation beam is on. Karanam et al 4 have hinted at potential synergisms of TTFields and simultaneous radiation therapy, and simultaneous therapies would be one of several options to enable patients to receive TTFields several weeks sooner than in the current clinical paradigm.18,19,21 However, before the 2 therapies could be delivered simultaneously, it is necessary to determine if either therapy interferes with the accuracy of the other.
The purpose of this work is to examine the targeting accuracy of treating central nervous system (CNS) and stereotactic body radiation therapy (SBRT) patients with simultaneous TTFields and radiation therapy on a robotic radiosurgery platform with skull tracking or fiducial tracking. In the Stachelek et al 5 study, radiation dosimetric effects from the TTFields arrays were analyzed by first scanning a head phantom without the arrays, and then comparing radiation treatment plans calculated on the nonTTFields array phantom to those recalculated with the arrays in place. In a similar strategy, the skull tracking tests in the present study use a CT scan of the phantom without the arrays in place as the reference, to compare the potential effects in targeting if the arrays were added in various positions at the time of treatment.
The first concern we address in this work is to determine if the ceramic disks inhibit the ability to accurately target the radiation, especially if skull tracking is used. The ceramic disks are close to the density of bone and therefore are very clearly visible in the stereoscopic x-rays used for localization. This means that before skull tracking with the robotic radiosurgery platform could be used for patients, steps would need to be taken to ensure that excessive target localization errors could be prevented. Therefore, fiducial tracking was used for the actual end-to-end measurement in this study, which would be applicable to the extracranial body sites which are currently being investigated for TTFields.11–15 This is a preliminary phantom study to assess the targeting of patients wearing the electrodes and to examine the effect of the radiation environment on the TTFields generator and the fields in-situ.
Materials and Methods
The methods and results are both separated into 2 parts: (1) a series of skull tracking feasibility tests consisting of imaging only and (2) a fiducial tracking end-to-end measurement.
Skull Tracking Feasibility Tests on Head Phantom
The TTFields arrays are repositioned on a weekly basis for patients, so in order to test localization, the anthropomorphic head phantom 22 was CT scanned without any of the ceramic electrodes in place; 0.625 mm thin slices were used. When the phantom was on the treatment table as in Appendix Figure A1, the arrays were taped in place for ease of repositioning. A series of imaging tests were taken, as in Appendix Figure A2, to assess the potential effects on skull tracking each time the TTFields array position was changed.
The skull tracking treatment plan was CT scanned several months before we obtained the TTFields arrays; we simply used the normal monthly quality assurance skull tracking end-to-end plan for the dedicated robotic stereotactic system. This method completely eliminated any influence of the TTFields arrays on the treatment plan, because the plan was created before the arrays were placed on the phantom. As can be seen in Figure A1, the TTFields system consists of 4 separate arrays, 1 on the posterior, 2 on the sides, and 1 on the superior portion of the head. Initially, only the posterior array was affixed to the head phantom, since the posterior array could not be repositioned without moving the head phantom. The head phantom was then placed on the treatment table and aligned using skull tracking image guidance. For the entirety of all skull tracking tests, the posterior array and head phantom remained in this exact position, while the other 3 arrays were taped on in various positions, and skull tracking images were taken for each position of the 3 movable arrays, to determine any potential effects on the targeting accuracy. No end-to-end targeting measurements were performed with skull tracking, because methods to ensure the prevention of large targeting errors would be needed before it could be considered for patients.
Fiducial Tracking End-to-End Measurement of Ball Cube in Water Phantom
In addition to the skull tracking tests, fiducial tests were also performed because both hypofractionated treatments and TTFields have been used extracranially, since body arrays are also available.11–15 For this test, we wanted to target not only based on fiducials but also to examine the effects of the radiation environment on the TTFields system. This study used a dedicated robotic radiosurgery platform to deliver a typical radiation plan to a phantom that was designed to mimic the clinical situation of a patient with implanted fiducials receiving simultaneous TTFields and radiation therapy. The standard for end-to-end accuracy measurement of robotic radiosurgery is the ball cube phantom 22 as shown in Figure 1, which holds 2 orthogonal sheets of 2.5 × 2.5 inch Gafchromic film. The target in the center of the cube is a 3-cm diameter sphere which is 12% denser than water so it is visible on CT scan and can be delineated as the target, as seen in Figure 2.
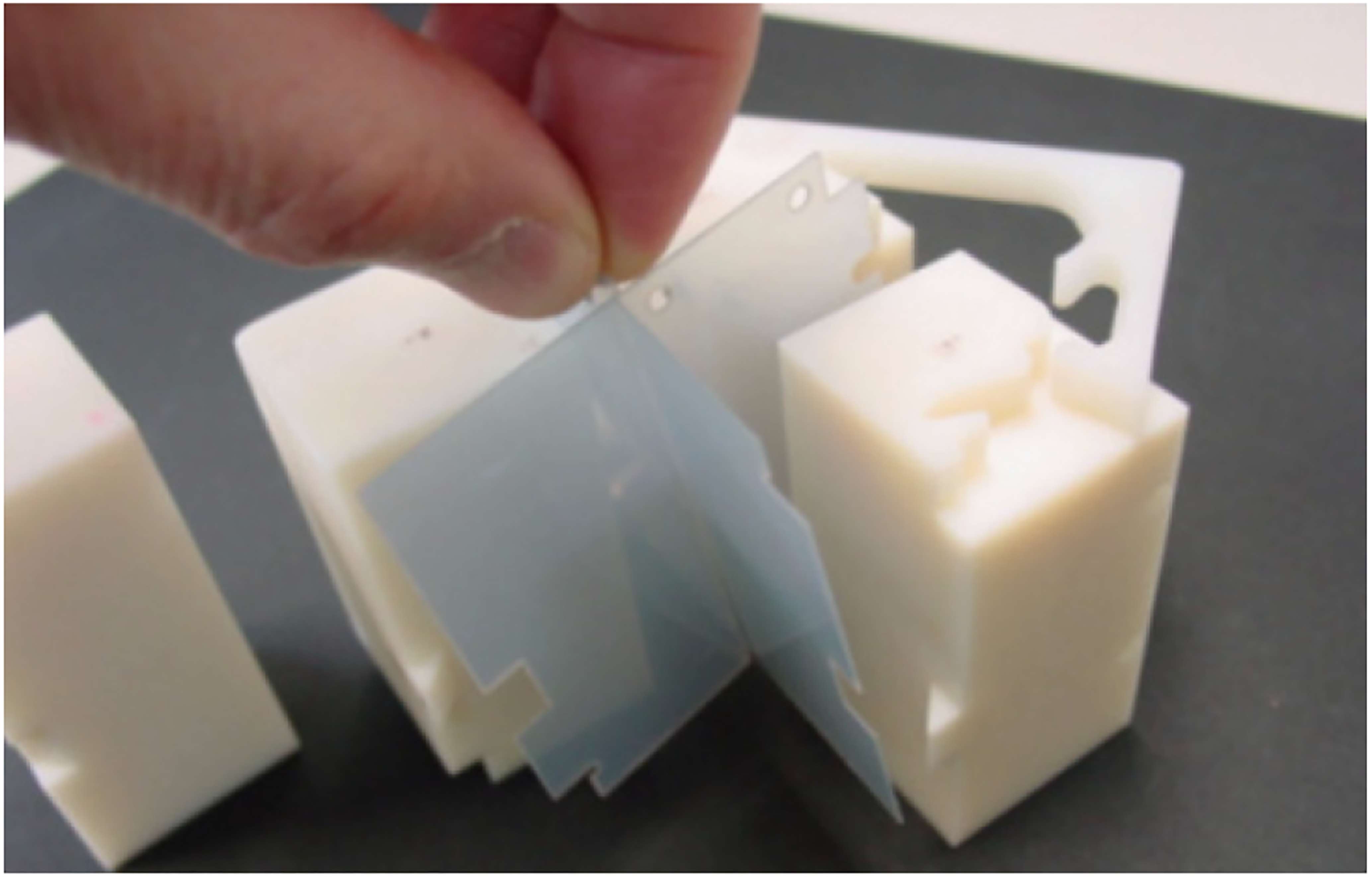
End-to-end targeting tests using the Accuray anthropomorphic phantom, showing insertion of 2 perpendicular pieces of film.

Treatment planning system view of tumor treating fields (TTFields) arrays surrounding the saline water bath with the ball cube phantom inside. In the upper portion of the figure (A) and (B) are 2 oblique images of the phantom with the ceramic electrodes clearly visible. The fiducials used for alignment are identified by the purple target marks. On the bottom of the figure, axial, sagittal, and coronal views have the isodose lines superimposed on the cube phantom in the water bath.
It is worth noting that the TTFields generator measures the “skin temperature” and will shut the generator off and sound an alarm if the temperature drops much below that of normal human skin (33 °C), as a safety mechanism in case the array comes loose from a patient. In addition, the generator checks the impedance, also alarming and shutting the generator off if the impedance is not in the normal range. In contrast to the skull tracking tests that used an existing treatment plan for the fiducial tracking test, the phantom was scanned, planned, and irradiated within an hour to ensure the water temperature remained within the allowable range to avoid these alarms.
To achieve this, first, the TTFields arrays were affixed to the inside edges of the phantom as in Figure 2, then the container was filled with warm water, at approximately 38 °C, and a small amount of salt was added initially. The ceramic TTFields disks were then connected to the TTFields generator, and as the water was stirred, salt was slowly added until the impedance across each pair of TTFields arrays through the saline bath was approximately 100 Ω and the TTFields software showed the maximal current of 2000 mA, peak-to-peak (amplitude of 1000 mA) in all arrays. A plastic red 16-ounce cup (part number P16RCT, Solo Cup Company) was used as a platform to position the cube in the middle of the phantom. The cup was trimmed shorter in order to customize the height of the ball cube in the center of the saline bath, and the cup was left in the same position throughout the entire procedure. The ball cube phantom was then submerged in the water tank, and pieces of solid water were placed on the top of the cube to keep the cube submerged. 1 The entire assembly was taken to the CT scanner for the planning scan.

Delivery of simultaneous tumor treating fields (TTFields) during radiation on the robotic radiosurgery platform using fiducial tracking. (A) Saline bath with ball cube phantom on the treatment table with the TTFields arrays powered on. (B) Live tracking views on the robotic radiosurgery system console.
The CT was acquired using 0.625 mm slice thickness and subsequently imported to the Precision treatment planning system, where the target was delineated. The ball cube phantom has embedded gold fiducials, and in the planning process these fiducials are identified so that the delivery system tracks these for targeting (Figure 2). A treatment plan was developed using a 3 cm fixed cone, optimized to conform to the target per our standard end-to-end test procedures. 22 Delivery of the treatment by a CyberKnife S7 is shown in Figure 3; the plan consisting of 58 isocentric beams with 6 Megavoltage flattening filter-free photons took less than 20 minutes to irradiate. During the treatment (end-to-end test), the TTFields electrodes were in place and powered on while the radiation was simultaneously being delivered. The orthogonal films were removed from the phantom, scanned, and analyzed with the vendor-supplied end-to-end software to assess the accuracy of the alignment (Figure 4).

The results of the fiducial tracking end-to-end test that was delivered to the ball cube phantom in the saline bath while the tumor treating fields (TTFields) arrays were powered on.
Results
Skull Tracking Feasibility Tests on Head Phantom
A series of stereoscopic x-ray images were taken with the phantom in a fixed known position as shown in Figures A1 to A2, to quickly assess the effects of array position on the targeting accuracy without performing full end-to-end tests. Since the posterior TTFields array could not be moved without moving the phantom, it was left in place throughout all of these tests. Table A1 shows the reference position of the phantom, which was determined by averaging 5 stereoscopic images with only the posterior array in place.
The phantom was left in this same position throughout the remaining tests, therefore any subsequent measurement in excess of 0.1 mm or 0.1° may be considered as a targeting error. At the end of the series of measurements, another ideal set of images like this were taken, verifying that the phantom was not inadvertently moved by more than 0.1 mm or 0.1°.
In the next series of tests, the anterior array was added. In each of the 3 positions of the anterior array, 2 sets of stereoscopic images were taken and compared to each other, as may be seen in Table A2. The phantom and the posterior TTFields array remained in the same position as when the tests in Table A1 were performed. Ideally, the Brightness and Gradient metrics for both images A and B should all be 1.00. In Table A1, it may be seen that the Brightness was only 1% less than ideal when the posterior TTFields array was in place, but that the Gradient was 2% to 4% lower than ideal. In Table A2, with both the anterior and posterior array in the image, the Brightness was 4% to 5% lower than ideal and the Gradient was about 25% lower. The shifts and rotations in Table A2 are quite similar to those in Table A1, but the large difference in Brightness and Gradient may indicate that the tracking algorithm is beginning to have difficulty.
Tables A3 and A4 show results of the final skull tracking tests, in which the full TTFields arrays were placed on the phantom, with the phantom still remaining in the same reference position as in the other tests. The last column in Table A4 has a 3D Euclidean distance approaching half a millimeter from the median reference position of Table A1, from imaging alone without an end-to-end test, which is sufficiently large to indicate the need for further investigation before skull tracking would be used on patients.
In the first 2 rows of Table A3, the imaging technique was the same as for all images in Tables A1 and A2, which for Imager A was 109 kV, 100 mA, 100 msec and for Imager B was 106 kV, 100 mA, 100 msec. In the middle 2 rows of Table A3, energy was changed to 100 kV for both imagers, and in the last 2 rows, it was set to 120 kV. Brightness and Gradient varied greatly among the tests in Table A3.
Fiducial Tracking End-to-End Measurement of Ball Cube in Water Phantom
The duration of the entire fiducial tracking radiation treatment was 10 min and 38 s to deliver all 58 isocentric beams with a 3-cm fixed cone. During the treatment saline bath remained within the allowable temperature and impedance range the entire time without any alarms from the TTFields system. Graphs from the TTFields system in Figure 5 shows that there were no discernible effects on TTFields current output recorded in the logfiles when the radiation beam pulsed on and off, with the reported current in both channels remaining within 1998 to 2004 mA (peak-to-peak) throughout the entire irradiation.

Data file from the tumor treating fields (TTFields) system shows that while the radiation beam was pulsed on and off throughout the measurement, the maximum peak-to-peak variation in the current per channel was (2004-1998)/2001 = 0.3%.
The submillimeter end-to-end targeting accuracy specification was met, and the ceramic electrodes did not inhibit the targeting of the dedicated robotic radiosurgery system. Even when delivering radiation through the TTFields arrays simultaneously while the arrays were powered on, a submillimeter targeting result of 0.47 mm was achieved (Figure 4). The ∼200 kHz TTFields signal did not adversely affect the targeting beyond the submillimeter accuracy specification. Based on the film analysis of the end-to-end test the root-mean-square targeting error was 0.47 mm.
Discussion
TTFields is one of the modern treatment options for GBM. The benefit of TTFields therapy following standard chemoradiation for GBM has been demonstrated by randomized clinical trials resulting in significant overall and progression-free survival.3,16 There is speculation that the simultaneous delivery of TTFields and radiation may be synergistic, 4 so the purpose of the present phantom study was to first test targeting effects.
As expected, the overall targeting has not changed. The fiducial tracking result still met the standard targeting specification even with the TTFields electrodes in place and powered on. For skull tracking treatments, more work on the localization needs to be done to find the best method for the targeting system to ignore the electrodes, particularly the potential impact of the large changes to Brightness and Gradient metrics in Tables A1 to A3 would need to be thoroughly explored. The thickness of each ceramic disk is 1 mm, but this does not necessarily represent the maximal induced targeting inaccuracy because they are denser than bone. If the patients were to be scanned with the array in place, there would be a substantial photon starvation artifact (streaking) that would hamper the ability for the tracking algorithm to properly function. A more thorough investigation on the potential effects on the tracking algorithm would be advisable before skull tracking with TTFields arrays is used clinically. In the clinical setting, the electrodes would not be anticipated to be distributed on the patient exactly the same way every day making this targeting more challenging. Furthermore, the TTFields system has certain temperature and impedance requirements that were more feasible to achieve in a nonanthropomorphic phantom which could not be targeted with skull tracking. Therefore, fiducial tracking was used for the end-to-end measurement in this paper, and although potential feasibility of skull tracking was shown, a much more exhaustive series of tests would need to be done before safety for patients could be ensured, which is beyond the scope of this paper.
The submillimeter end-to-end specification of the robotic radiosurgery platform can only be measured explicitly in a phantom, but several studies have shown similar accuracy in more realistic environments.23–26 The targeting test in the present study was a one-time experiment and is not intended to mandate a new quality assurance procedure. Other more detailed tests of TTFields simultaneously with radiation are planned.
For the skull tracking tests, the phantom remained in the same position for all tests; a more thorough future study would be to repeat this for various shifts and rotations, but for initial verification, this was a serviceable method. Since Table A3 showed that Brightness and Gradient varied greatly as a function of imaging technique when the TTFields arrays were present for skull tracking, this would need to be more fully explored with a series of actual end-to-end targeting tests before use on patients, which is beyond the scope of this paper, so a fiducial tracking end-to-end test was used instead.
There are a few concerns that have been raised regarding simultaneous delivery. Radiation dose is imparted by photon interactions that lead to electron cascades in tissue that may be affected by the alternating TTFields. However, each electron cascade is very short-lived relative to the frequency of the TTFields. The mean energy of the ions that ultimately deliver the dose is ∼34 eV but they interact within 10−9 s. So, there is potential for the dose distribution to be blurred but because of the short-lived electrons, this blurring may be difficult to measure with film because the effect is very small. In addition, the blurring effect is further minimized by the delivery method because the dose delivery was achieved with 58 unique beam angles, so the composite dose blurring would be extremely small and therefore difficult to measure.
Another interplay is related to the dose deposition process. By generating ion pairs in the medium, we change the impedance of the medium. But in this experiment, the reported current from the TTFields system remained within 0.3% of a constant 2000 mA (peak-to-peak). If there was an impedance shift during the treatment, the TTFields generator seemed able to adjust adequately. It is worth noting that there was an observed heating of the phantom during the water phantom measurements that appear to be consistent with Joule heating. In a clinical study, 10% to 17% of patients felt a heat sensation, 27 indicating that hyperthermia could potentially be another synergistic effect of the simultaneous therapies,27–30 although this was superficial heating and presumed not to be heating of the deep tissue. This phenomenon is being studied in greater detail in our upcoming work, which will also account for inherent temperature regulation within a patient.
Stachelek et al 5 compared radiation plans without the TTFields arrays to those recalculated with the arrays in place. Likewise, in the present study, a phantom was CT scanned without the arrays and skull tracking was tested with the arrays added. Since the arrays are repositioned on the patient periodically, the goal of both of these studies is to determine if the effects of the arrays can average out, for both treatment planning dosimetry and for the targeting accuracy. Initial treatments for patients may need CT scans without and with the TTFields arrays for direct comparisons on patients, but if phantom testing and patient comparisons can ultimately show that the arrays do not adversely impact the dose distribution or targeting, then it might eventually be possible to account for the TTFields array effects in plans that were CT scanned without the arrays.
For example, the surface dose may be greatly increased directly below each ceramic disc as shown by Li et al 19 but the dose there is usually already low 5 because of skin-sparing effects of high energy photons and because the average human skull thickness is 6.5 mm which provides a transition region from the high dose in the tumor to a lower dose at the skin. Therefore, although there can be a dramatic percentage increase of 130% to 260% 19 at the surface, the absolute dose in those regions may remain low. 5 Considering all these effects, a phantom study of 10 consecutive patients treated for glioblastoma that were recalculated to a cranial phantom found that dose increases for the highest-dose 1 and 20 cc volumes (D1cc and D20cc) of 5 mm thick skin contours were 3.1%, and skin dose for all 10 cases remained below clinical dose tolerance levels. 5 A clinical study of concurrent TTFields and radiation encountered temporary grades 1 to 2 skin erythema, dermatitis, or pruritus in 80% of patients, but no grade 3 toxicity. 20 These effects must be monitored and quantified thoroughly in upcoming clinical trials, and when they are more fully understood, it might be possible to account for them in plans that were CT scanned without the arrays.
Conclusion
A robotic treatment system with real-time automated stereoscopic x-ray fiducial tracking can be used to successfully target radiation in a phantom with the TTFields arrays in place and activated simultaneously while the radiation beam is on. The end-to-end accuracy specification was met, even when delivering radiation through the TTFields arrays simultaneously while the arrays were powered on, with a final targeting result of 0.47 mm. As shown in Figure 5, no discernible effects beyond 0.3% on TTFields output current were observed when the radiation beam pulsed off and on.
Supplemental Material
sj-doc-1-tct-10.1177_15330338211039135 - Supplemental material for Targeting Accuracy Considerations for Simultaneous Tumor Treating Fields Antimitotic Therapy During Robotic Hypofractionated Radiation Therapy
Supplemental material, sj-doc-1-tct-10.1177_15330338211039135 for Targeting Accuracy Considerations for Simultaneous Tumor Treating Fields Antimitotic Therapy During Robotic Hypofractionated Radiation Therapy by Sharmi Biswas, Irina Kapitanova, Sabrina Divekar, Jimm Grimm, Ian J. Butterwick, Daniel Garren, Lawrence R. Kleinberg, Kristin J. Redmond, Michel Lacroix, Anand Mahadevan and Kenneth M. Forster in Technology in Cancer Research & Treatment
Footnotes
Abbreviations
Acknowledgments
The physics measurements were made possible with visionary innovative biomedical support from Ed Bodzio.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Novocure.
Supplemental Material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.