
Abstract
Background:
The aim of our study was to develop a nomogram model to predict overall survival (OS) and cancer-specific survival (CSS) in patients with gastric signet ring cell carcinoma (GSRC).
Methods:
GSRC patients from 2004 to 2015 were collected from the Surveillance, Epidemiology, and End Results (SEER) database and randomly assigned to the training and validation sets. Multivariate Cox regression analyses screened for OS and CSS independent risk factors and nomograms were constructed.
Results:
A total of 7,149 eligible GSRC patients were identified, including 4,766 in the training set and 2,383 in the validation set. Multivariate Cox regression analysis showed that gender, marital status, race, AJCC stage, TNM stage, surgery and chemotherapy were independent risk factors for both OS and CSS. Based on the results of the multivariate Cox regression analysis, prognostic nomograms were constructed for OS and CSS. In the training set, the C-index was 0.754 (95% CI = 0.746-0.762) for the OS nomogram and 0.762 (95% CI: 0.753-0.771) for the CSS nomogram. In the internal validation, the C-index for the OS nomogram was 0.758 (95% CI: 0.746-0.770), while the C-index for the CSS nomogram was 0.762 (95% CI: 0.749-0.775). Compared with TNM stage and SEER stage, the nomogram had better predictive ability. In addition, the calibration curves also showed good consistency between the predicted and actual 3-year and 5-year OS and CSS.
Conclusion:
The nomogram can effectively predict OS and CSS in patients with GSRC, which may help clinicians to personalize prognostic assessments and clinical decisions.
Introduction
Gastric cancer is the sixth most common malignant tumor worldwide, and its fatality rate ranks second in the world. 1 It is a malignant tumor that seriously threatens the health of people in China, and its morbidity and mortality are both ranked second in China. 2 According to the classification established by the Japanese Gastric Cancer Society, gastric cancer can be classified into adenocarcinoma, mucinous adenocarcinoma, signet ring cell carcinoma and other types. 3 Although the incidence and mortality of gastric cancer have decreased with the widespread eradication of Helicobacter pylori and the early diagnosis of gastric cancer, the incidence of gastric signet ring cell carcinoma (GSRC) has significantly increased and the prognosis is poor. 4,5
GSRC belongs to primary gastric cancer, which is a highly malignant tumor, accounting for 3.4%-39% of gastric cancer. 6,7 GSRC has its unique clinicopathological features, which mainly originate from undifferentiated stem cells with active proliferation of glandular neck in the lamina propria of gastric mucosa. 8 GSRC is one of the types of gastric cancer with poor tissue differentiation, which has the characteristics of low differentiation, high invasiveness and poor prognosis. 9 Studies have shown that age, TNM stage, epidermal growth factor receptor (EGFR), surgical methods, perineural invasion (PI), and lymph node metastasis status are independent risk factors for the prognosis of GSRC. 10,11
The nomogram is simplified by multivariate regression analysis to incorporate a large number of prognostic factors into a single short numerical estimation model to predict the possibility of events. 12 The nomogram allows clinicians to more visually assess the health status of an individual patient and provide personalized treatment to the patient. 13 Currently, the nomograms are commonly used for the prognosis (e.g., overall survival (OS), progression-free survival (PFS), or cancer-specific survival (CSS) of cancer patients. 14
Currently, the nomogram has been widely used in the prognostic assessment of gastric cancer patients. Han et al 15 retrospectively analyzed 7,954 gastric cancer patients who underwent D2 gastrectomy and constructed a nomogram that could predict 5-year and 10-year OS. Hirabayashi et al 16 included 39,859 patients who underwent gastric cancer surgery at multicenter in Japan from 2001 to 2003, and constructed a postoperative serosa-negative advanced gastric cancer (AGC) with a 5-year OS nomogram.
The nomogram has been constructed in GSRC and have been validated as valid and correct. 17,18 However, the population selection of the above studies were relatively limited. In this context, we used the Surveillance, Epidemiology, and End Results (SEER) database to analyze the clinicopathological features and prognostic factors of OS and CSS in patients with GSRC, and developed and verified 3-year and 5-year OS and CSS prognostic nomograms of patients with GSRC.
Materials and Methods
Patients Selection
The Surveillance, Epidemiology and final results (SEER) Database is an open public database that was launched in 1973. 19 It comes from population registries of 18 sites and covers about 28% of the population of the United States. 20 SEER database can provide clinical information of cancer patients, such as gender, age, year of diagnosis, race, tumor primary site, tumor size, tumor grade, tumor stage, pathological type, survival time and cause of death. In this study, SEER*Stat software (version 8.3.6, SEER 18 Regs Custom Data (with additional treatment fields), Nov 2018 Sub (1975-2016 varying) database) (https://seer.cancer.gov/seerstat/) was used.
In the present study, according to the International Classification of Diseases for Oncology (ICD-O), patients with gastric cancer with pathological type code (8490/3: signet ring cell carcinoma) at the primary site of stomach between 2004 and 2015 were included. A total of 12,825 GSRC patients were included in the study. Subsequently, we excluded multiple tumors (n = 2,613), unknown survival time (n = 21), unknown American Joint Committee on Cancer (AJCC) stage (n = 1,013), and unknown TNM stage (n = 2,029). In the end, 7,149 patients were included in the final study.
Clinical Variables
We extracted the gender, age, marital status, race, origin, tumor grade, Tumor-Node-Metastasis (TNM) stage, SEER stage, treatment (surgery, radiotherapy and chemotherapy), survival time, survival status and cause of death of GSRC patients from the SEER database. The end points of the study were OS and CSS. OS was defined as the time from diagnosis to death or last follow-up visit, CSS was defined as the time from diagnosis to death due to GSRC or the last follow-up.
Ethical Statement
The contents of this article are data mining from the Surveillance, Epidemiology and End Results (SEER) database. The SEER database is open and shared. The data released from the SEER database did not require informed patient consent because cancer is a reportable disease in every state in the US.
Statistical Analyses
In this study, the best cut-off value of age (<62 years, 62-80 years and >80 years) (Figure S1) was determined by X-tile software (version 3.6.1, Yale University School of Medicine, US). All patients were randomly divided into training set and validation set according to the proportion of 2:1 using R software. Univariate and multivariate Cox regression analysis was used to analyze the risk factors related to OS and CSS in patients with GSRC, and the hazard ratio (HR) and 95% confidence interval (CI) were calculated. Variables with P-value < 0.05 in the univariate Cox proportional risk model were further analyzed in the multivariate Cox proportional risk model. Based on the results of multivariate Cox regression analysis, the independent risk factors of OS and CSS were included, and the prognostic nomograms of 3-year, and 5-year OS and CSS were established. Receiver operating characteristic (ROC) curve and decision curve analysis (DCA) curve were used to analyze the sensitivity and specificity of the nomogram, TNM stage and SEER stage, and determined the area under the curve (AUC). 21 In addition, the performance of the nomogram was evaluated by the C-index and the calibration curve (1000 bootstrap resamples). All of the above analyses were performed using SPSS software (version 24.0, Chicago, USA) and R software (version 3.6.2). All tests were two-sided. P-value < 0.05 (2-sided) was considered statistically significant.
Results
Demographic and Clinical Characteristics
A total of 7,149 GSRC patients were enrolled in the study, of which 4,766 (66.7%) were assigned to the training set and 2,383 (33.3%) were included in the validation set. Table 1 shows the demographic and clinical characteristics of GSRC patients in the entire cohort, training set, and validation set. Among all patients, male patients were slightly higher than female patients (52.6% vs 47.4%). Most of the patients were younger (<62 years, 50.2%), married (58.5%), white (69.3%), Non-Spanish-Hispanic-Latino (NSHL) (775.4%). The majority of tumors were grade III (79.7%), AJCC stage IV (42.1%), T1-2 stage (60.1%), N0 stage (44.4%) and M0 stage (67.1%). In addition, more than half of the patients received surgery (58.7%) and chemotherapy (58.9%).
Clinical and Demographic Characteristics of Patients With Gastric Signet Ring Cell Carcinoma (GSRC).

Abbreviations: NSHL, Non-Spanish-Hispanic-Latino; SHL, Spanish-Hispanic-Latino; AJCC, American Joint Committee on Cancer; SEER, Surveillance, Epidemiology, and End Results.
Risk Factors of OS and CSS in Patients With GSRC
To examine factors associated with OS and CSS in patients with GSRC, we conducted univariate and multivariate Cox regression analysis in the training set. Univariate Cox regression analysis showed that age, marital status, race, grade, AJCC stage, TNM stage, SEER stage, surgery, radiotherapy and chemotherapy were associated with OS (All P < 0.05) (Table 2). After incorporating the above factors into the multivariate Cox regression analysis, we found that age, marital status, race, AJCC stage, TNM stage, SEER stage, surgery and chemotherapy were independent risk factors for OS. Similarly, we found that age, marital status, race, AJCC stage, TNM stage, surgery, radiotherapy and chemotherapy were independent risk factors for CSS (Table 3).
Univariate and Multivariate Analysis of Overall Survival (OS) Rates in Training Set.

Abbreviations: OS, Overall survival; HR, hazard ratio; CI, confidence intervals; NSHL, Non-Spanish-Hispanic-Latino; SHL, Spanish-Hispanic-Latino; AJCC, American Joint Committee on Cancer; SEER, Surveillance, Epidemiology, and End Results.
a Model was adjusted by age, marital status, race, grade, AJCC stage, T stage, N stage, M stage, SEER stage, surgery, radiotherapy and chemotherapy.
Univariate and Multivariate Analysis of Cancer-Specific Survival (CSS) Rates in Training Set.

Abbreviations: CSS, Cancer-specific survival; HR, hazard ratio; CI, confidence intervals; NSHL, Non-Spanish-Hispanic-Latino; SHL, Spanish-Hispanic-Latino; AJCC, American Joint Committee on Cancer; SEER, Surveillance, Epidemiology, and End Results.
a Model was adjusted by gender, age, marital status, race, origin, grade, AJCC stage, T stage, N stage, M stage, SEER stage, surgery, radiotherapy and chemotherapy.
Construction Nomograms
Based on the above multivariate Cox regression analysis results, we constructed OS nomogram (Figure 1A) based on age, marital status, race, AJCC stage, TNM stage, SEER stage, surgery and chemotherapy, and CSS nomogram (Figure 1B) based on age, marital status, race, AJCC stage, TNM stage, surgery, radiotherapy and chemotherapy. We found that surgery made the largest contribution to survival outcomes in the OS nomogram, whereas AJCC stage made the largest contribution in the CSS nomogram.

Nomogram predicting 3-, and 5-year OS and CSS rate of GSRC patients. A, OS rate; B, CSS rate. OS indicates overall survival; CSS, cancer-specific survival; GSRC, gastric signet ring cell carcinoma.
Nomogram Validation
We validate the OS and CSS nomograms in both the training set and the validation set. In the training set, the C-index of the OS nomogram was 0.754 (95%CI: 0.746-0.762) and the C-index for the CSS nomogram was 0.762 (95%CI: 0.753-0.771). In the validation set, the C-index for the OS nomogram was 0.758 (95%CI: 0.746-0.770) and for the CSS nomogram was 0.762 (95%CI: 0.749-0.775). Regardless of the training set and validation set, the C-index of OS and CSS nomograms were significantly higher than those of TNM stage and SEER stage (Table 4). In addition, we calibrated the 3-year and 5-year OS and CSS nomograms for the training set and the validation set, and found that the nomograms were very close to the ideal curve (Figure 2 and Figure S2).
Comparison of C-Indexes Between the Nomogram, TNM Stage and SEER Stage in Gastric Signet Ring Cell Carcinoma (GSRC) Patients.

Abbreviations: HR, hazard ratio; CI, confidence interval; SEER, Surveillance, Epidemiology, and End Results.
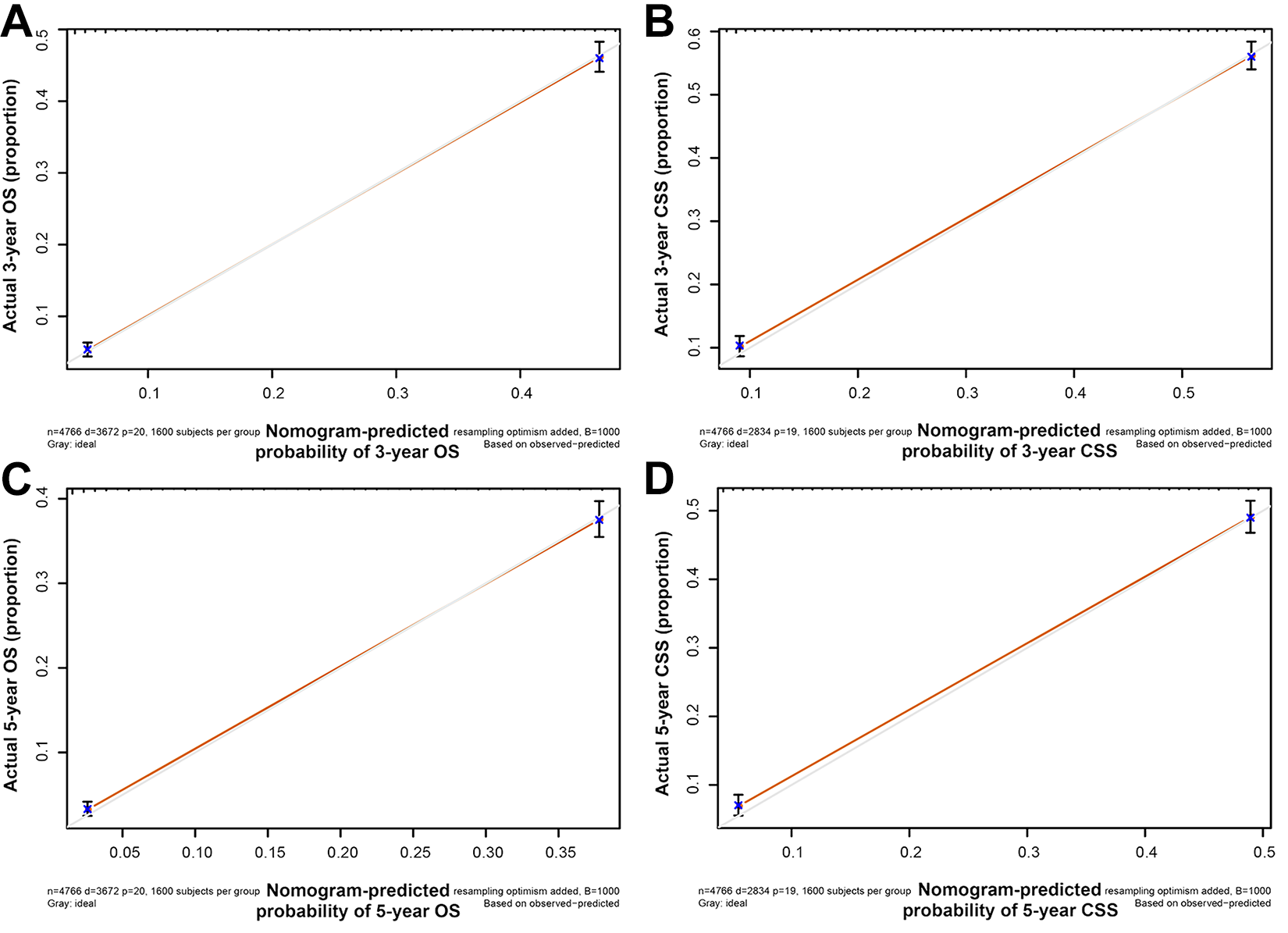
Calibration plot of the nomogram for predicting 3-, and 5-year OS and CSS in training cohort. A, 3-Year OS; B, 3-year CSS; C, 5-year OS; D, 5-year CSS. OS indicates overall survival; CSS, cancer-specific survival.
We performed ROC curves analyses for OS and CSS at 3-year and 5-year, respectively, and found that there was a high AUC in the training set and validation set (Figure 3). In addition, we performed DCA curve analysis and ROC curve analysis on the nomogram (Table S1), TNM stage and SEER stage, respectively (Figures 4 and 5), and found that the nomogram performance of OS and CSS was significantly better than that of TNM stage and SEER stage, regardless of the training set and validation set.
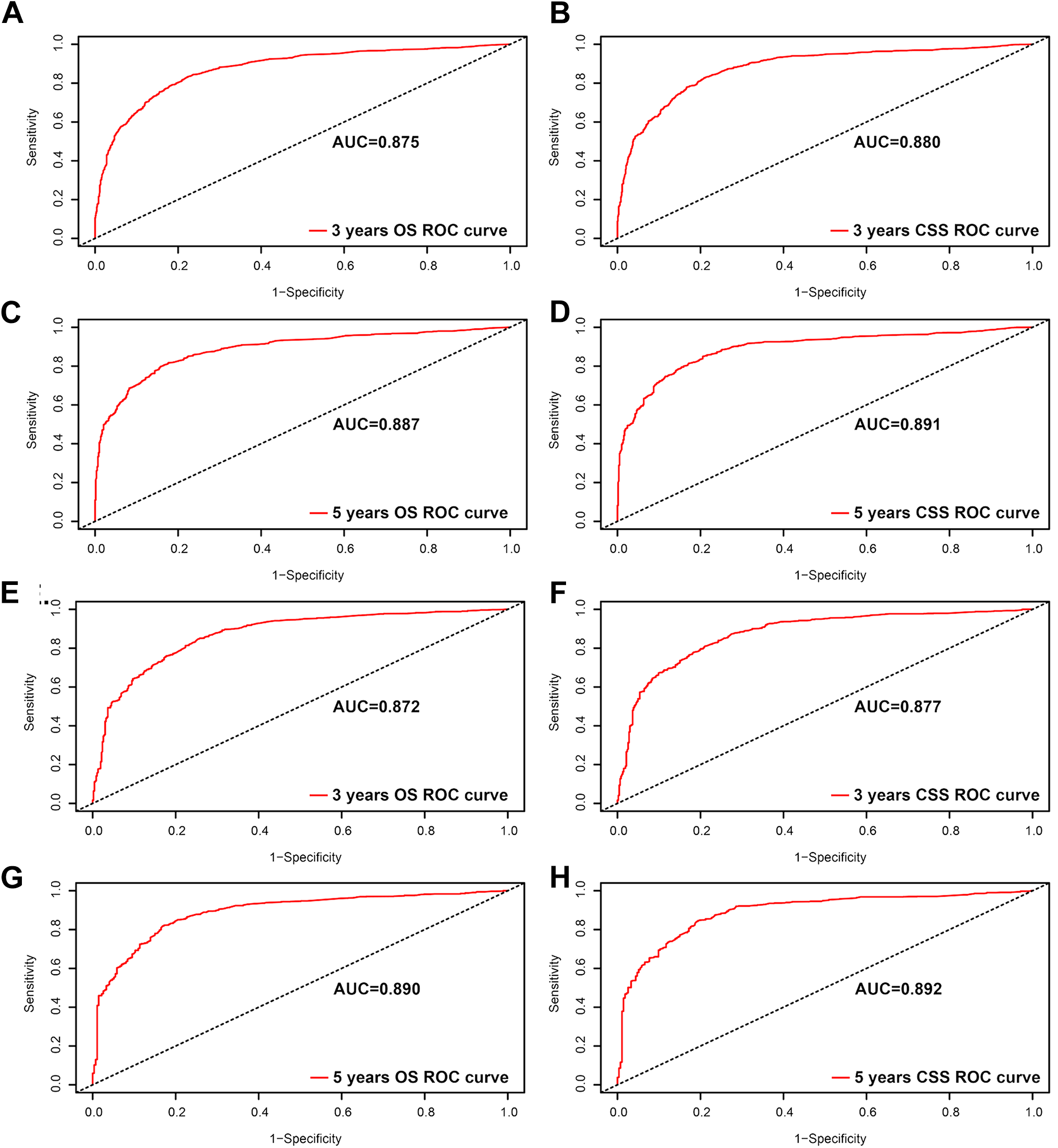
ROC curves for the nomogram. A, The ROC curve of nomogram with 3-year OS in training set; B, the ROC curve of nomogram with 3-year CSS in training set; C, the ROC curve of nomogram with 5-year OS in training set; D, the ROC curve of nomogram with 5-year CSS in training set; E, the ROC curve of nomogram with 3-year OS in validation set; F, the ROC curve of nomogram with 3-year CSS in validation set; G, the ROC curve of nomogram with 5-year OS in validation set; H, the ROC curve of nomogram with 5-year CSS in validation set. ROC indicates receiver operating characteristic; OS, overall survival; CSS, cancer-specific survival.
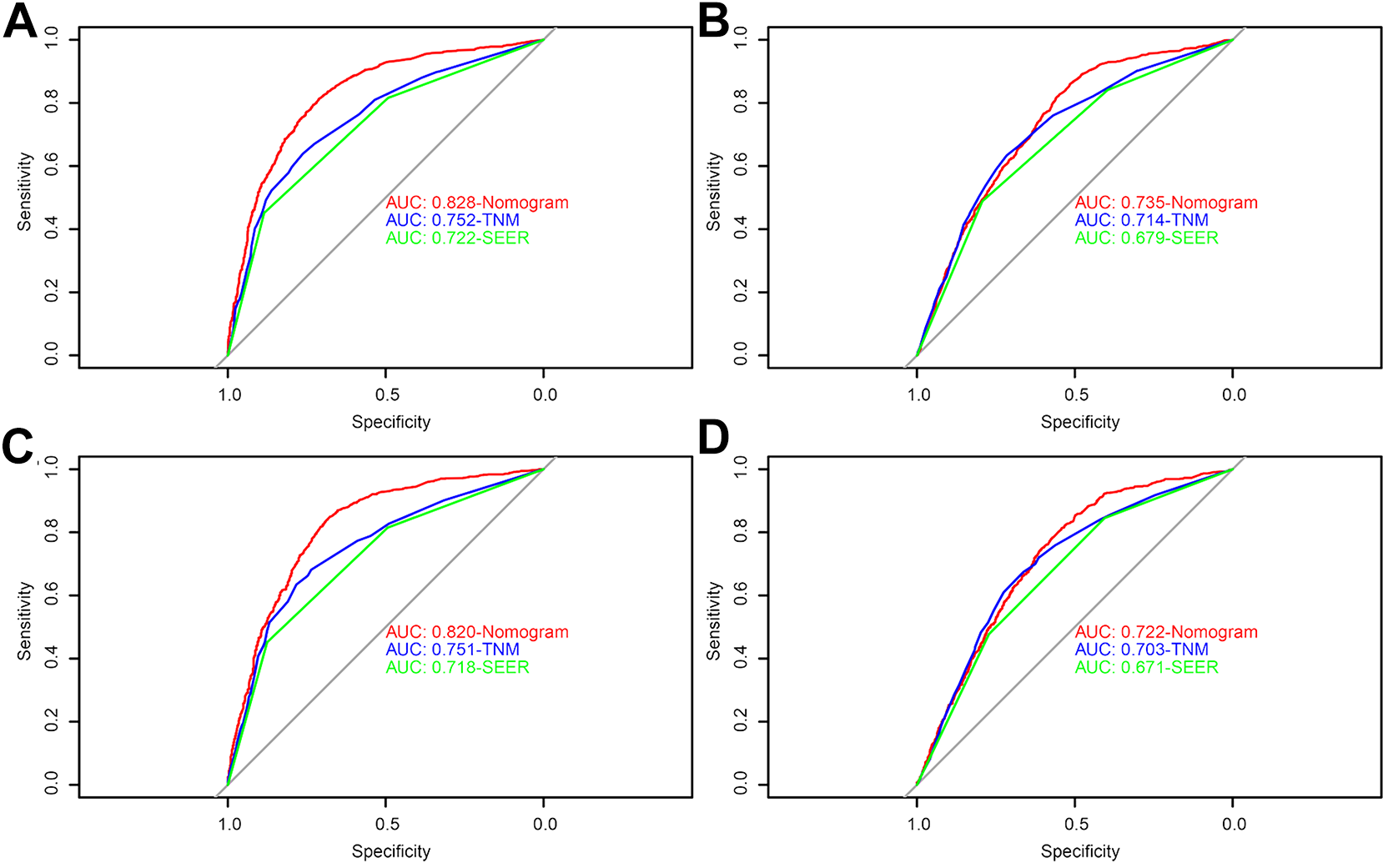
ROC curve for the nomogram, TNM stage and SEER stage. A, The OS ROC curve of nomogram, TNM stage and SEER stage in training set; B, the CSS ROC curve of nomogram, TNM stage and SEER stage in training set; C, the OS ROC curve of nomogram, TNM stage and SEER stage in validation set; D, the CSS ROC curve of nomogram, TNM stage and SEER stage in validation set. ROC indicates receiver operating characteristic; OS, overall survival; CSS, cancer-specific survival; SEER, Surveillance, Epidemiology, and End Results.

DCA curve for the nomogram, TNM stage and SEER stage. A, The OS DCA curve of nomogram, TNM stage and SEER stage in training set; B, the CSS DCA curve of nomogram, TNM stage and SEER stage in training set; C, the OS DCA curve of nomogram, TNM stage and SEER stage in validation set; D, the CSS DCA curve of nomogram, TNM stage and SEER stage in validation set. DCA indicates decision curve analysis; OS, overall survival; CSS, cancer-specific survival; SEER, Surveillance, Epidemiology, and End Results.
Discussion
The incidence of GSRC has been increasing in recent years, despite a decrease in the incidence of gastric cancer. 5,22 Therefore, it is necessary to further investigate the predictors that may affect the long-term survival of GSRC patients and it is important to develop valuable models to predict the prognosis of GSRC patients. In the present study, we performed univariate and multivariate Cox regression analysis based on large clinical data to identify independent risk factors for prognosis of OS and CSS in GSRC patients. Depend on the results of multivariate Cox regression analysis, we first established a prognostic nomogram of OS and CSS in GSRC patients and validated it internally. In addition, we also found that the predictive ability of the nomogram was more accurate than that of TNM stage and SEER stage by examining the C-index, ROC curves and DCA curves. And the predictive ability of the nomogram basically consistent with the actual results. In addition, the C-index and AUC of both the OS and CSS nomograms are greater than 0.7, indicating that the nomograms had sufficient discrimination ability.
Currently, TNM stage is commonly used to predict the prognosis status of cancer patients, but because it only includes tumor size, lymph node status and metastasis, it is unclear how other variables such as age, sex, race, marital status, tumor grade and treatment modality affect patient prognosis. 23 Therefore, nomograms were constructed to incorporate various factors to consider the prognosis of the patients. Many studies have shown that nomograms are more accurate than conventional TNM stage in predicting the cancer patient survival. 24,25 Consequently, the combination of TNM stage and other prognosis-related factors can better predict the prognosis of GSRC patients.
Recently, many studies have developed nomograms that include various prognostic factors to predict the prognosis of different gastrointestinal tumors. Based on the SEER database, Yu and Zhang 26 developed and validated a prognostic nomogram for predicting OS and CSS in patients with early-onset gastric cancer, which can promoted the clinical prognosis assessment and personalized treatment of early-onset gastric cancer. Hu et al 27 found that the nomogram combined with liver fibrosis score was more effective than the TNM staging system and clinicopathological nomogram in predicting hepatic-specific disease-free survival (DFS) and recurrence-free survival (RFS). In addition, Xie et al 28 found that the nomogram was superior to the traditional TNM staging in predicting individual disease-specific survival (DSS) in patients with non-metastatic esophageal cancer after preoperative radiotherapy.
Studies have constructed prognostic nomograms of patients with GSRC, but these studies have limited population selection. Wei et al 18 included the clinical information from 1,030 patients with locally advanced (stage II and stage III) GSRC between 2004 and 2012, and constructed CSS prognostic nomogram based on age, sex, race, marital status, stage, registy, lymph node, location, tumor size, radiotherapy and chemotherapy, and found that patients who received postoperative radiotherapy had a better prognosis than patients who underwent surgery alone. Guo et al 17 collected 256 early-stage GSRC between January 2002 and December 2015, constructed a nomogram predicting lymph node metastasis (LNM) and performed external validation using a database of 1,273 patients from Cancer Institute Ariake Hospital in Tokyo. Lin et al 29 collected patients with gastric adenocarcinoma containing GSRC and constructed a gastric adenocarcinoma-specific survival (GCSS) prognosis nomogram based on age, race, grade, TN stage, pathological type and tumor size, which can provide relatively accurate survival predictions for patients with operable gastric adenocarcinoma (GA) after gastrectomy. In this study, we included all patients only diagnosed with GSRC from 2004 to 2015 and successfully constructed nomogram of OS based on 10 factors: age, marital status, race, AJCC stage, TNM stage, SEER stage, surgery and chemotherapy, CSS nomogram based on age, marital status, race, AJCC stage, TNM stage, surgery, radiotherapy and chemotherapy, and the constructed nomograms were found to have a better prognosis than TNM stage and SEER stage.
Although the currently constructed nomograms show high accuracy in predicting OS and CSS in GSRC patients, the limitations of this study should not be overlooked. First, the SEER database lacks detailed information on surgery, radiotherapy and chemotherapy, such as the specific type of operation, the dose of radiotherapy and the chemotherapy regimen. Second, the physical condition of GSRC patients may also influence their treatment choices. Final, the SEER database is a retrospective study and further prospective studies are needed. Despite some limitations, the results suggest that the prognostic nomogram we constructed is a guiding model that can provide accurate predictions of survival outcomes for GSRC patients.
In conclusion, we have constructed and validated OS and CSS prognostic nomograms for GSRC with a high degree of accuracy compared to TNM stage and SEER stage, which can help clinicians to personalize survival predictions for GSRC patients.
Supplemental Material
Supplemental Material, sj-pdf-1-tct-10.1177_15330338211027912 - A Prognostic Model for Patients With Gastric Signet Ring Cell Carcinoma
Supplemental Material, sj-pdf-1-tct-10.1177_15330338211027912 for A Prognostic Model for Patients With Gastric Signet Ring Cell Carcinoma by Qinping Guo, Yinquan Wang, Jie An, Siben Wang, Xiushan Dong and Haoliang Zhao in Technology in Cancer Research & Treatment
Supplemental Material
Supplemental Material, sj-tif-1-tct-10.1177_15330338211027912 - A Prognostic Model for Patients With Gastric Signet Ring Cell Carcinoma
Supplemental Material, sj-tif-1-tct-10.1177_15330338211027912 for A Prognostic Model for Patients With Gastric Signet Ring Cell Carcinoma by Qinping Guo, Yinquan Wang, Jie An, Siben Wang, Xiushan Dong and Haoliang Zhao in Technology in Cancer Research & Treatment
Supplemental Material
Supplemental Material, sj-tif-2-tct-10.1177_15330338211027912 - A Prognostic Model for Patients With Gastric Signet Ring Cell Carcinoma
Supplemental Material, sj-tif-2-tct-10.1177_15330338211027912 for A Prognostic Model for Patients With Gastric Signet Ring Cell Carcinoma by Qinping Guo, Yinquan Wang, Jie An, Siben Wang, Xiushan Dong and Haoliang Zhao in Technology in Cancer Research & Treatment
Footnotes
Authors’ Note
Qinping Guo and Yinquan Wang contributed equally to this article. Conception and design: QG, XD and HZ. Administrative support: QG, JA, SW and YW. Provision of study materials or patients: QG, JA, SW and YW. Collection and assembly of data: XD and HZ. Data analysis and interpretation: QG, JA, SW and YW. Manuscript writing: QG and YW. Final approval of manuscript: All authors. Our study did not require an ethical board approval because it did not contain human or animal trials.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The work was supported by Applied Basic Research Project of Shanxi Province (Nos. 201901D111404).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.