
Abstract
Background and Aims:
There is a lack of research on metastatic renal pelvis cell carcinoma in the current literature. In this study, we aimed to detect distant metastatic patterns in renal pelvis cell carcinoma, and illustrated the affection of different metastatic sites, surgery to primary site and chemotherapy on prognosis outcomes in patients with diverse conditions.
Methods:
We collected data between 2010 and 2015 from the Surveillance, Epidemiology and End Results database. Kaplan–Meier analysis with log-rank test was used for survival comparisons. Multivariate Cox regression model was employed to analyze the effect of distant metastatic sites on overall survival (OS) and cancer-specific survival (CSS).
Results:
A total of 424 patients were included in the analysis, the median follow-up time was 5 months (interquartile range (IQR): 2-12) and 391 deaths (92.2%) in all patients were recorded. Among them, 192 (45.3%), 153 (36.1%), 137 (32.3%) and 127 (30.0%) patients were diagnosed with lung, bone, liver and brain metastases, respectively, while only 12 (2.8%) patients had brain metastases. The bi-organ, tri-organ and tetra-organ metastatic pattern was found in 135 (31.8%), 32 (7.5%) and 11 (2.6%) patients, respectively. The multivariate Cox analyses showed that distant lymph nodes (DL) metastases was not an independent prognostic factor for both OS and CSS (OS: Hazard ratios (HR) = 1.1, 95% CI = 0.8-1.4, P = 0.622; CSS: HR = 1.0, 95% CI = 0.8-1.3, P = 0.906). Besides, there was no significant difference of survival in patients with T3-T4 stage (OS: HR = 0.8, 95% CI = 0.5–1.2, P = 0.296; CSS: HR = 0.8, 95% CI = 0.5–1.2, P = 0.224), N2-3 stage (OS: HR = 0.8, 95% CI = 0.5–1.3, P = 0.351; CSS: HR = 0.7, 95% CI = 0.4–1.2, P = 0.259) and multi-organ metastases (OS: HR = 0.8, 95% CI = 0.5–1.3, P = 0.359; CSS: HR = 0.7, 95% CI = 0.4–1.2, P = 0.179) between surgery to primary site group and no-surgery to primary site group.
Conclusion:
we described the metastatic patterns of mRPCC and the prognosis outcomes of DL metastases, surgery to primary site and chemotherapy. Our findings provide more information for clinical therapeutic intervention and translational study designs.
Keywords
Introduction
Upper-tract urothelial carcinoma (UTUC), containing both renal pelvis and ureter tumors, is a rare genitourinary malignant tumor, responsible for almost 5% of all urothelial cancers. 1 However, with the diversification of diagnosis methods and improvement of overall survival rate in the last 5 decades, patient groups with UTUC have continually increased, especially for renal pelvis cell carcinoma (RPCC). 2 -4 The rate of patients with localized RPCC is in decline, 5 and patients with distant metastases appear to have a worse prognosis. Thus, it is beneficial to research the distant metastatic patterns to improve diagnosis and therapy of patients with metastatic RPCC (mRPCC).
Neoplasm metastasis undergoes a complex course that includes the migration of cancer cells from the original site, metastasis throughout the entire body, and then accommodation to a new microenvironment at distant sites. 6 The progression of tumor cells is considered as a cross-correlation between seeds (cancer cells) and soil (microenvironment of the host organ). 7 At present, some researchers have suggested 3 steps of invasion-metastasis: epithelial-mesenchymal transition, angiogenesis, and immune evasion. In addition, certain host organs may be more amenable to the survival and proliferation of specific tumors, because of the more suitable microenvironment. 8 By clarifying the preference of metastatic sits in mRPCC patients, we can better understand this “seed and soil” interaction.
The patient treatment plan for mUTUC is still limited to chemotherapy, and surgery to the primary site (pSUR), etc. However, there is a lack of research on the efficacy of pSUR within the existing literature, and is limited to the application of surgery to the current guidelines. 9,10 There have been 2 reports that have suggested a survival benefit after chemotherapy in the setting of surgically and non-surgically treated mUTUC. 11,12 However, most of the above reports are limited to UTUC or mUTUC, without considering the influence of 2 different cancer sites. There is currently a lack of research focused solely upon RPCC or ureter cell carcinoma (TCC), although there are still controversies about the prognosis of the 2 types of UTUC. 13 -15 Based on the limited nature of the report, in which the benefit of surgery and chemotherapy in patients with mRPCC was described, it is beneficial to postulate a formal, confirmatory study in this era of pursuing evidence-based medicine.
In this study, we used data from the American Surveillance, Epidemiology, and End Results (SEER) program to detect distant metastatic patterns in RPCC, and illustrated the effects upon different metastatic sites, and surgery and chemotherapy on prognosis outcomes in patients with diverse conditions. We supposed that mRPCC presents with a special metastatic frequency and patients with different metastatic sites will have different prognosis outcomes. Additionally, both pSUR and chemotherapy could improve prognostic outcome in different cohorts of mRPCC patients. We present the following article in accordance with the STROBE reporting checklist.
Methods
Our data were obtained from the National Cancer Institute’s SEER program through SEER*Stat software V.8.3.5, which covers approximately 34.6% of the U.S. population (https:// seer. cancer. gov/, accession numbers 13693-Nov2015 and lh8N79l2). In this study, we selected patients diagnosed with RPCC between 2010 and 2015. Patient information includes age, race, gender, marital status, laterality, grade, cancer tumor node metastasis (TNM) staging according to the criteria from the American Joint Committee on Cancer (AJCC) seventh versions, therapies (primary surgery, metastatic surgery, radiotherapy and chemotherapy), cause of death and survival in months. Our exclusion criteria included (1) not first primary malignancy; (2) unknown information; (3) M0 stage of the cancer. The specific selecting process has been included as Supplemental Figure 1.
Statistical Analyses
Descriptive statistics were used to summarize the clinical characteristics of patients. Continuous variables were expressed as means ± standard deviation (SD) and were compared using a Student’s t test, while categorical parameters among different groups features were compared using a Pearson’s chi-square test or Fisher’s exact test. We used a Venn diagram to clarify the distribution of distant metastatic sites. Survival curves were plotted using the Kaplan-Meier method and the log-rank test was conducted. Univariate and multivariate cox regression models were performed in order to determine the hazard ratios (HRs) with 95% confidence intervals (CIs) for overall survival (OS) and cancer-specific survival (CSS). Among them, variables that were introduced to the basic model or were eliminated from the complete model and that had an impact on the regression coefficient of X > 10%, were included in multivariate Cox regression models. Subgroup analysis via multivariate Cox models were conducted to discovery the different effects within populations with different conditions. All statistical tests were 2-sided, and the significance level was P < 0.05. Data were analyzed using the statistical package R (the R foundation; http://www.r-project.org;version3.4.3).
Ethics Statement
The permission from the National Cancer Institute USA was granted to get the SEER data for research purposes only (reference number: 21111-Nov2018). All the data from the SEER database were de-identified, and the extracted data did not require informed consent.
Results
Patient Characteristics and Metastatic Patterns
A total of 424 patients were included in the analysis. The demographics, tumor characteristics and therapies status are presented in Supplemental Table 1. Tumor characteristics, therapies status and follow-up information were missing from 259 patients (7.81%), and our analysis showed that these data met the “missing at random” hypothesis. By comparison to the non-lung-metastatic group, the lung-metastatic group was inclined to have a higher incidence of TCC histologic type, and a higher rate of primary surgery and radiotherapy. By comparison to the non-bone-metastatic group, the bone-metastatic group was inclined to have a lower rate of radiotherapy. By comparison to the non-liver-metastatic group, the liver-metastatic group was inclined to have a higher rate of radiotherapy. By comparison to the non-brain-metastatic group, the brain-metastatic group was inclined to have a lower incidence of metastatic surgery, and a higher rate of unmarried patients. By comparison to the non-DL-metastatic group, the DL-metastatic group was inclined to have a higher N stage.
We used a Venn diagram (Figure 1) to further clarify metastatic sites distribution. This distribution showed that 192 patients (45.3%) were diagnosed with lung metastases, 153 patients (36.1%) had bone metastases, 137 patients (32.3%) had liver metastases, 127 patients (30.0%) had DL metastases, and only 12 patients (2.8%) had brain metastases. A bi-organ, tri-organ or tetra-organ metastatic pattern was found in 135 (31.8%), 32 (7.5%) and 11 (2.6%) patients, respectively. There were significant differences between all co-metastatic patterns (

Venn diagram of the distribution of distant metastatic sites in the overall cohort. DL, distant lymph node.
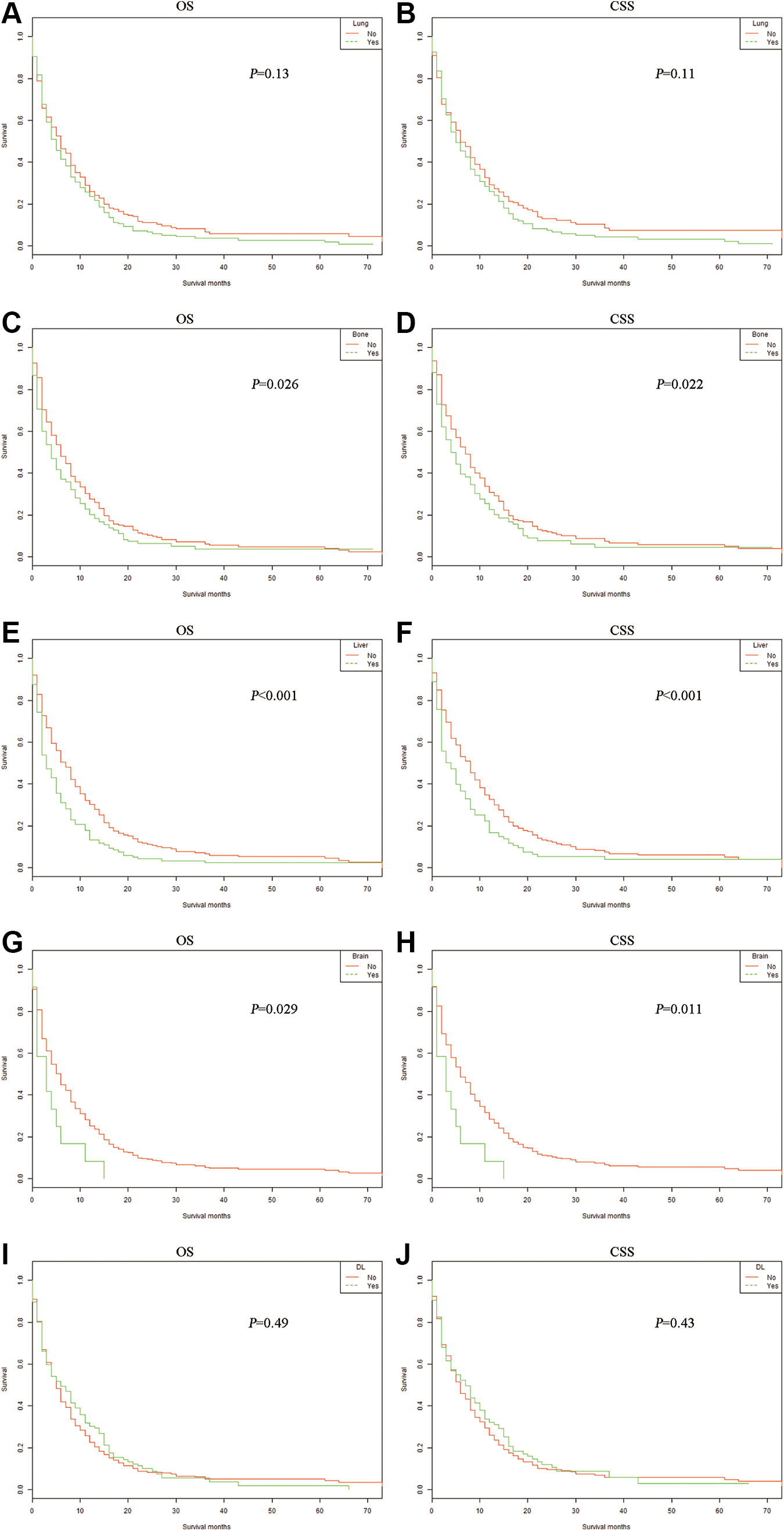
Kaplan–Meier curves of OS and CSS according to whether or not patients had lung (A, B), bone (C, D), liver (E, F), brain (G, H) and DL (I, J) metastases. OS, overall survival; CSS, cancer-specific survival; DL, distant lymph node.
Impact of Metastatic Sites on Survival Outcomes
In our research, the median follow-up time was 5 months (interquartile range (IQR): 2-12), and for which 391 deaths (92.2%) for all patients were recorded. The OS and CSS were compared according to different metastatic sites. For patients with bone, liver and brain metastases, Kaplan–Meier analyses showed worse outcomes both for OS and CSS (Figure 2), compared to patients without the corresponding sites of metastases: with vs without bone metastases: P = 0.026 for OS and P = 0.022 for CSS; with vs without liver metastases: P < 0.001 for both OS and CSS; with vs without brain metastases: P = 0.029 for OS and P = 0.011 for CSS. For patients with lung and DL metastases, Kaplan–Meier analyses did not show different outcomes for OS or CSS, compared to patients without the corresponding sites of metastases: with vs without lung metastases: P = 0.13 for OS and P = 0.11 for CSS; with vs without DL metastases: P = 0.49 for OS and P = 0.43 for CSS. Multivariate Cox analyses (Table 1) showed that only DL metastases was not an independent prognostic factor for both OS and CSS (OS: HR = 1.1, 95% CI = 0.8-1.4, P = 0.622; CSS: HR = 1.0, 95% CI = 0.8-1.3, P = 0.906). In order to determine the impact of DL metastases upon survival in different patients, we conducted further sub-group analyses, and found that patients with DL metastases was not associated with worse OS or CSS in different cohorts (Figure 3).
Multivariate Cox Regression Analysis of Prognostic Factors Influencing Survival Outcomes in Overall Patient Cohort.

Abbreviations: OS, overall survival; CSS, cancer-specific survival; DL, distant lymph node.
Note: ‡Including American Indian/AK Native, and Asian/Pacific Islander.
* Cancer TNM stage according to criteria from the American Joint Committee on Cancer (AJCC) 7th versions.

The forest plot for HR comparing overall survival and cancer-specific survival between the group with DL metastases (A) and group without distant lymph node metastases (B) according to different variables. HR, Hazard ratio.
Our results revealed that patients with single-organ and bi-organ metastasis had significantly better outcomes for both OS (single-organ metastases vs more than 2 organs metastases: HR = 1.9, 95% CI = 1.3–2.7, P < 0.001; bi-organ metastases vs more than 2 organs metastases: HR = 1.6, 95% CI = 1.1–2.3, P = 0.011) and CSS (single-organ metastases vs more than 2 organs metastases: HR = 1.9, 95% CI = 1.3–2.7, P < 0.001; bi-organ metastases vs more than 2 organs metastases: HR = 1.6, 95% CI = 1.1–2.4, P = 0.009), than patients with more than 2 metastatic organs (Figure 4). There were no differences for prognosis of patients diagnosed with single-organ metastases and 2-organ metastases for both OS and CSS (OS: HR = 1.2, 95% CI = 1.0–1.5, P = 0.117; CSS: HR = 1.1, 95% CI = 0.9–1.4, P = 0.268). The results of further multivariate Cox analyses were confirmed for the above results (

Kaplan–Meier curves of OS (A) and CSS (B) according to the number of metastatic sites. OS, overall survival; CSS, cancer-specific survival. #More-site means more than 2 sites (including 3 and 4 metastatic sites) in this figure.
The survival outcomes of patients with single-site metastasis were also analyzed, and patients with DL-only metastases had a better prognosis compared to patients with liver-only (DL-only vs liver-only: OS: HR = 0.6, 95% CI = 0.4–1.0, P = 0.033; CSS: HR = 0.6, 95% CI = 0.4–1.0, P = 0.033) as shown in the Kaplan–Meier analyses (Figure 5). However, patients with DL-only metastases had a better prognosis compared to patients with bone-only, liver-only or lung-only metastases (bone-only vs DL-only: OS: HR = 1.9, 95% CI = 1.2–3.3, P = 0.012; CSS: HR = 2.0, 95% CI = 1.2–3.4, P = 0.012; liver-only vs DL-only: OS: HR = 1.7, 95% CI = 1.0–2.9, P = 0.049; CSS: HR = 1.8, 95% CI = 1.0–3.1, P = 0.046; lung-only vs DL-only: OS: HR = 1.7, 95% CI = 1.0–2.7, P = 0.036; CSS: HR = 1.7, 95% CI = 1.0–2.8, P = 0.038) as shown using multivariate Cox analyses (Table 2). Due to the very small number of patients with brain-only metastases (4 patients), this data was not included in the comparison.
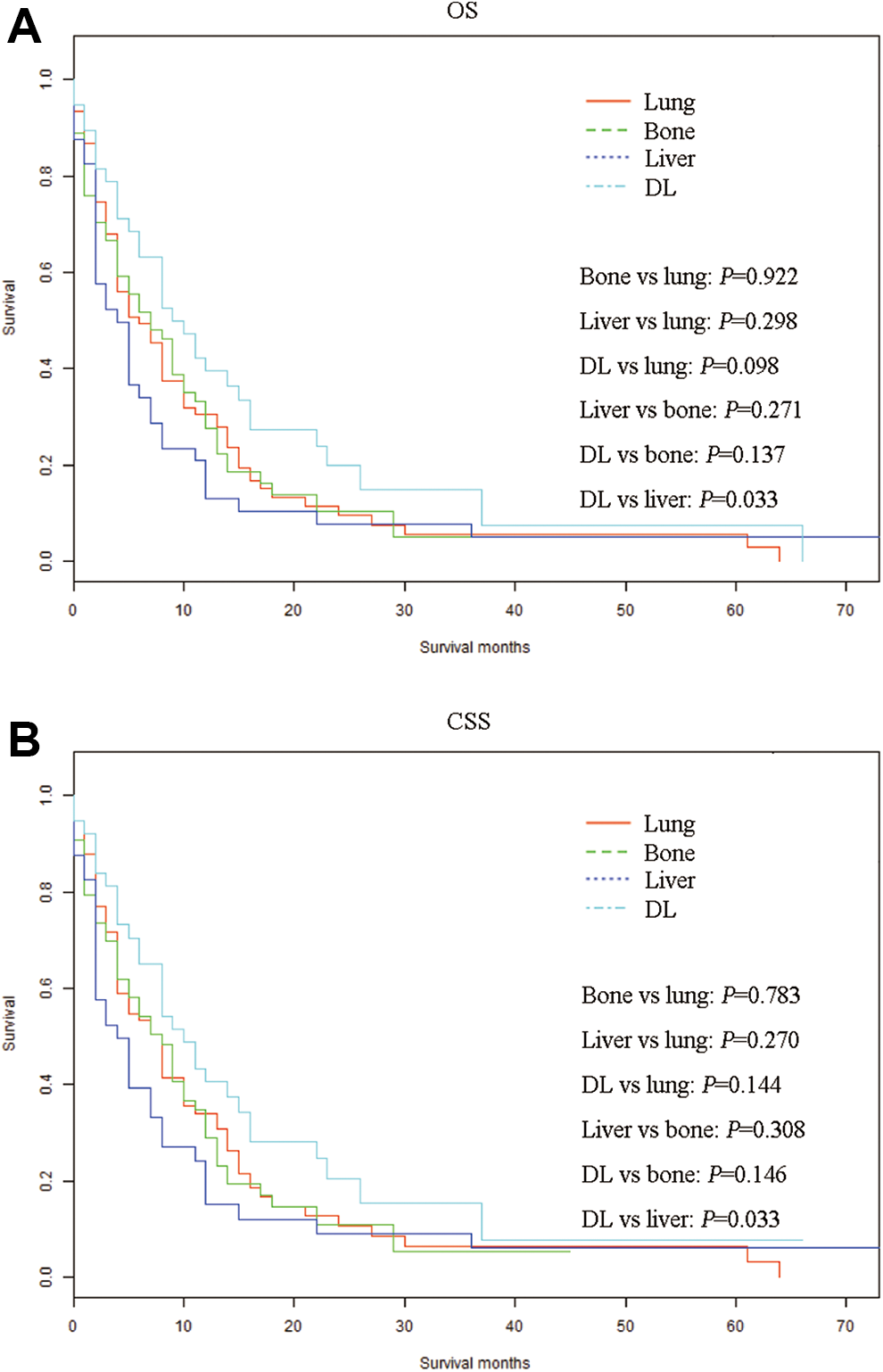
Kaplan–Meier curves of OS (A) and CSS (B) according to the sites of metastases in patients with single metastatic site. OS, overall survival; CSS, cancer-specific survival; DL, distant lymph node.
Multivariate Cox Regression Analysis of Prognostic Factors Influencing Survival Outcomes in Patients With Single Metastatic Site.

Note: ‡Including American Indian/AK Native, and Asian/Pacific Islander.
* Cancer TNM stage according to criteria from the American Joint Committee on Cancer (AJCC) 7th versions.
OS, overall survival; CSS, cancer-specific survival; DL, distant lymph node.
Effect of pSUR and chemotherapy on survival outcomes
For the multivariate Cox analyses of the overall cohort (Table 1), we found that pSUR (OS: HR = 0.7, 95% CI = 0.5–1.0, P = 0.032; CSS: HR = 0.7, 95% CI = 0.5–0.9, P = 0.007) and chemotherapy (OS: HR = 0.3, 95% CI = 0.3–0.4, P < 0.001; CSS: HR = 0.3, 95% CI = 0.3–0.4, P < 0.001) improved both OS and CSS. Subgroup analyses were conducted in order to further determine the effect of pSUR and chemotherapy on OS and CSS in different patients. Chemotherapy improved both OS and CSS in all different cohorts (Figure 6); while there was no significant difference in survival for patients with T3-T4 staged cancer (OS: HR = 0.8, 95% CI = 0.5–1.2, P = 0.296; CSS: HR = 0.8, 95% CI = 0.5–1.2, P = 0.224), N2-3 staged cancer (OS: HR = 0.8, 95% CI = 0.5–1.3, P = 0.351; CSS: HR = 0.7, 95% CI = 0.4–1.2, P = 0.259), and for multi-organ metastases (OS: HR = 0.8, 95% CI = 0.5–1.3, P = 0.359; CSS: HR = 0.7, 95% CI = 0.4–1.2, P = 0.179) between the pSUR group and the no pSUR group (Figure 6).

The forest plot for HR comparing overall survival and cancer-specific survival between the group with primary site surgery (A) and group without primary site surgery (B) and between the group with chemotherapy (C) and group without chemotherapy (D) according to different variables. HR, Hazard ratio.
Discussion
Distant metastasis is still an essential issue in RPCC, resulting in poor prognosis. Thus, it is effectual to detect the metastatic patterns of mRPCC and the prognosis outcomes of pSUR and chemotherapy. In the current study, we firstly elaborated the distribution of metastases. Secondly, we researched the impact of metastatic sites upon survival outcomes. Thirdly, the benefit of surgery and chemotherapy for patients with mRPCC was investigated for different cohorts. As far as we know, ours is the first in-depth study that has clarified metastatic patterns and prognosis outcomes for mRPCC. Therefore, we expect that our study results could be instrumental in guiding future translational studies and clinical practices in UTUC.
After analyzing the metastatic frequencies of RPCC, we found that lung was the most common metastatic site, while brain was the least common metastatic lesion in our patient cohort, consistent with the study of Shinagare’s group. 16 In order to better investigate metastases, we divided the patients into single-site, bi-site, tri-site and tetra-site metastatic cohorts. We were surprised to find that almost one-third of the patients in our cohort had 2-site metastases. The results showed that clinicians need to be conscious of the likelihood of combined metastasis at different lesions, and therefore consider and perform precise diagnosis and treatment of multi-organ metastasis.
We further considered the influence of each metastasis site upon prognosis outcomes. This revealed that lung, bone, liver, and brain metastasis could all cause a poor prognosis, while the occurrence of distant lymphatic metastasis had no obvious effect upon survival. We specially conducted a subgroup analysis, and the results further confirmed that no matter what kind of population, DL metastasis would not significantly affect survival. Additionally, for single-site metastatic cohorts, we showed that DL metastasis was also not an independent prognostic factor for metastatic mRPCC. To the best of our knowledge, our findings about DL metastasis in mRPCC have never been presented before. However, a similar finding was reported for metastatic bladder cancer in the publication by Dong et al. 17 Due to the rarity of cases, it is difficult to divide their patients into different cohorts from a single institution for further analysis and discussion. We solved this problem by using a large population of patients, and found that patients with single or 2 metastatic sites seemed to be related with improved survival, compared with those with 3 or 4 metastatic sites using the Kaplan-Meier method, and multivariate Cox regression models. Given that the above findings are all reported for the first time, we hope these results will inform clinical decision making and translational study designs.
Regarding the treatment plan of mRPCC, as a part of mUTUC, the most widely used clinical approach is chemotherapy and pSUR. However, the efficacy of pSUR has not been clearly confirmed, hence why surgery is not recommended in most guidelines. 9,10 Recently, Nazzani et al 18 suggested that irrespective of whether patients have experienced chemotherapy or not, pSUR is beneficial for the prognosis of mUTUC. It is, however, regrettable that this study only focuses on the survival benefit of pSUR in patients with or without chemotherapy, and does not discuss whether surgery can improve prognosis in various subgroups. In our clinical experience, the different stages of tumors often affect the prognosis of patients and thereby the choice of treatment for patients. Therefore, in order to fill this knowledge gap, we conducted a subgroup analysis of mRPCC patients, and found that pSUR intervention in the more advanced mRPCC (T3-4, N2-3 and with multiple metastatic sites) did not produce the expected survival benefit. However, this result needs to be verified by other prospective and multi-center studies.
In contrast, chemotherapy is currently the accepted treatment option for advanced UTUC. A recent meta-analysis concluded that there was a survival benefit in mUTUC patients with pSUR. 11 Furthermoer, Nazzani et al reported that, in non-surgery mUTUC patients, there were still a survival benefit for accepting chemotherapy. 12 In our study, we further confirmed the prognostic benefit of chemotherapy in various subgroups.
There are also some limitations with our study. Firstly, cases in this study were from retrospective cohorts, therefore more prospective, randomized clinical trials should be conducted to further confirm the study findings. Secondly, only patient data of between 2010 and 2015 for the metastatic information was available, and the majority of the enrolled patients were white, so the findings needed to be confirmed in other cohorts, such as an Asian cohort. Thirdly, there were potentially important confounders, such as smoking status, tumor volume of primary and metastatic site, comorbidities and index, time to surgery after diagnosis, surgical margins, surgical technique (i.e. robotic, laparoscopic…), chemotherapy delivery timing, number of cycles and specific chemotherapy agents, specific lymphadenectomy progress, for which data were not available in our database. Therefore, we hope that further prospective studies could be conducted to confirm our findings.
In summary, in this retrospective study, we described the metastatic patterns of mRPCC and the prognosis outcomes of DL metastases, pSUR and chemotherapy. Our findings provide more information to assist with future clinical therapeutic intervention and translational study designs.
Supplemental Material
Supplemental Material, sj-pdf-1-tct-10.1177_15330338211004914 - Prognostic Value of Site-Specific Metastases and Therapeutic Roles of Surgery and Chemotherapy for Patients With Metastatic Renal Pelvis Cancer: A SEER Based Study
Supplemental Material, sj-pdf-1-tct-10.1177_15330338211004914 for Prognostic Value of Site-Specific Metastases and Therapeutic Roles of Surgery and Chemotherapy for Patients With Metastatic Renal Pelvis Cancer: A SEER Based Study by Wei-Kang Chen, Zhi-Gang Wu, Yun-Bei Xiao, Qin-Quan Wang, Dong-Dong Yu, Jian Cai and Chao-Feng Zhou in Technology in Cancer Research & Treatment
Supplemental Material
Supplemental Material, sj-tif-1-tct-10.1177_15330338211004914 - Prognostic Value of Site-Specific Metastases and Therapeutic Roles of Surgery and Chemotherapy for Patients With Metastatic Renal Pelvis Cancer: A SEER Based Study
Supplemental Material, sj-tif-1-tct-10.1177_15330338211004914 for Prognostic Value of Site-Specific Metastases and Therapeutic Roles of Surgery and Chemotherapy for Patients With Metastatic Renal Pelvis Cancer: A SEER Based Study by Wei-Kang Chen, Zhi-Gang Wu, Yun-Bei Xiao, Qin-Quan Wang, Dong-Dong Yu, Jian Cai and Chao-Feng Zhou in Technology in Cancer Research & Treatment
Footnotes
Authors’ Note
(I) Conception and design: Weikang Chen, Jian Cai, Dongdong Yu and Chaofeng Zhou. (II) Administrative support: Jian Cai. (III) Provision of study materials or patients: Zhigang Wu, Yunbei Xiao and Qinquan Wang. (IV) Collection and assembly of data: Weikang Chen. (V) Data analysis and interpretation: WeiKang Chen. (VI) Manuscript writing: All authors. (VII) Final approval of manuscript: All authors. The data that support the findings of this study are openly available in Surveillance, Epidemiology, and End Results database (![]() ). The data that support the findings of this study are openly available in Surveillance, Epidemiology, and End Results database (https://seer.cancer.gov/seerstat/). We were granted permission from the National Cancer Institute USA to access the SEER dataset for research purposes only (reference number: 21111-Nov2018). All the data from the SEER database were de-identified, and the extracted data did not require informed consent. The authors have completed the STROBE reporting checklist.
). The data that support the findings of this study are openly available in Surveillance, Epidemiology, and End Results database (https://seer.cancer.gov/seerstat/). We were granted permission from the National Cancer Institute USA to access the SEER dataset for research purposes only (reference number: 21111-Nov2018). All the data from the SEER database were de-identified, and the extracted data did not require informed consent. The authors have completed the STROBE reporting checklist.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. All authors have completed the ICMJE uniform disclosure form. All authors have no conflicts of interest to declare.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.