
Abstract
Background:
The present study was designed to investigate the presence or absence of calcification and whether calcification size affect the diagnostic accuracy of ultrasonography (US) and computed tomography (CT) in predicting the benign or malignant nature of thyroid nodules.
Material and Methods:
From May 2014 to April 2019, 445 patients underwent thyroid US and neck CT before thyroid surgery. In each case, US and CT were retrospectively examined by radiologists. We divided the patients into 3 groups according to the type of calcification: no calcification, microcalcification, and macrocalcification. And macrocalcification group divided into rim calcifications and non-rim calcifications groups. We evaluated the diagnostic accuracy of US and CT for differentiating malignant from benign thyroid nodules using histopathological results as a reference standard.
Results:
In the overall population, adding CT to US resulted in greater sensitivity, lower specificity, and lower accuracy in the prediction of the benign or malignant nature of nodules. In the group with no calcification, US had a significantly greater accuracy than CT and combined US/CT. In the group with macrocalcification, especially in rim calcifications, adding CT to US resulted in greater sensitivity than US, and CT exhibited greater sensitivity and accuracy than US.
Conclusion:
US is superior to CT for the prediction of the benign or malignant nature of nodules in thyroid lesions according to calcification and CT is also currently not recommended as a routine imaging tool for thyroid nodules. However, the superior sensitivity and accuracy of CT in lesions with macrocalcification especially in rim calcifications may enable CT to play a complementary role in identifying benign and malignant nodules.
Introduction
Thyroid nodules are a common problem, with an estimated prevalence of 4-7% for palpable nodules. 1 Most nodules are benign; however, 4-5% of nodules are malignant, as suggested by the ultimate pathological diagnosis. 1 To avoid over- or undertreatment and their potential complications, it is important to predict the benign or malignant nature of nodules as accurately as possible preoperatively. 2,3 Thyroid ultrasonography (US) is the primary alternative method recommended by the guidelines and has been widely used to differentiate malignant from benign nodules and to assist with fine-needle aspiration cytology (FNAC) for suspected malignant nodules. 4,5 Predicted malignant nodules had combinations of all US features, including microcalcification, hypo echogenicity, irregular margins, the absence of a halo, intranodular vascularity, etc. 6 -8 However, some studies have shown that the characteristics of benign and malignant tumors partially overlap. 8,9 The sensitivity and specificity of US findings for malignant thyroid nodules had a wide range of variations. 10,11 The findings of US were affected by the US equipment, the experience or skills of radiologists, and different US criteria. There are also several important reasons for the variation in sensitivity and specificity. Meanwhile, the accuracy of preoperative FNAC is still controversial. 12,13
Computed tomography (CT) is a standard imaging modality for the evaluation of head and neck lesions but is currently not recommended as a routine imaging tool for thyroid nodules because of its low resolution for soft tissue, radiation hazards, and high costs. 5,14 However, CT has numerous advantages, such as a wide field of view, objectivity, and a detailed display of bone or air-containing organs. 15 Some previous studies have attempted to distinguish malignant from benign thyroid lesions by CT. 16 -19 A mean attenuation value greater than 55 Hounsfield units (HU) has been demonstrated to be a useful predictive factor of malignancy in CT. 18 In addition, HU values of calcified thyroid nodules may be helpful for differentiating malignant from benign nodules. 20 The degree and pattern of nodular enhancement are helpful CT features for distinguishing malignant from benign solid thyroid nodules. 21 However, there are not enough CT features to reliably differentiate malignant from benign thyroid lesions. 16
Calcification is a common finding in thyroid US or CT imaging. It may present various patterns, including microcalcification (tiny, punctate echogenic foci of
Material and Methods
Participants
Our institutional review board approved this retrospective study and waived the requirement for informed consent. From May 2014 to April 2019, 445 patients whose underwent thyroid US of nodular thyroid lesions followed by a neck CT scan within a close interval were enrolled.
Ultrasound
US examinations were performed prospectively before surgery by radiologists with experience in thyroid US. Thyroid US was performed with an 8-10 MHz linear transducer (660, Toshiba). The scanning protocol in all cases included both transverse and longitudinal real-time imaging of the thyroid nodules, with the use of representative Digital Imaging and Communications in Medicine images. Two experienced head and neck radiologists reviewed all of the US images. For the US of thyroid nodules, the 2 reviewers were asked to establish criteria from the ACR TI-RADS and published literature. 29 -31 The criteria included size, internal content, the presence of a spongiform appearance, shape, margin, echotexture, echogenicity of solid portions, and calcification. The radiologists did not know any of the surgical diagnoses and ultrasound findings. Each of the radiologists was asked to review the studies independently in a single session, and different results were determined after the consultation of the 2 radiologists. Calcification was classified as microcalcification (tiny, punctate echogenic foci of 2 mm or less) or macrocalcification (punctate echogenic foci or peripheral curvilinear calcification larger than 2 mm, including rim calcifications and non-rim calcifications). Rim calcifications were defined as curvilinear hyperechoic structures parallel to the margin of the nodule and encompassing 120°or more of the circumference. Calcification was based on pathology and US results.
Thyroid CT
A total of 445 patients underwent contrast-enhanced CT with an MDCT scanner (iCT 256, PHILIPS) with a reconstructed slice thickness of 2 mm for nonenhanced axial, enhanced axial, coronal, and sagittal images with 0.5-0.6 mm of collimation. A 90-mL dose of iodinated contrast medium (iopromide, Ultravist 300, Bayer Schering Pharma) was administered intravenously at a rate of 3 mL/s with an automated injector. A 3 mL/s flush of normal saline solution was injected immediately after the administration of the contrast medium to reduce artifacts induced in the subclavian vein. The scan delay was 50 s. CT images were prospectively interpreted by another head and neck radiologist who was blinded to the surgical diagnosis and US findings. The following CT features of thyroid nodules were retrospectively investigated: the degree and pattern of attenuation, configuration, margin, shape, pattern of calcification, and degree and pattern of nodular enhancement. 21
Statistical Analysis
The sensitivity, specificity, and accuracy of US, CT, and combined US/CT for identifying benign or malignant nodules were determined by patient-based analysis. Sensitivity was defined based on the diagnosis of malignant nodules. The final status of nodules was determined on the basis of the pathology results of surgical specimens. To assess the sensitivity or accuracy of the combination of US and CT, nodules were defined as malignant if either US or CT criteria were met. To assess the specificity of combined US/CT, nodules were defined as benign if both US and CT criteria were met. We performed subgroup analysis to compare the findings according to type of calcification (no calcification, microcalcification (<2 mm), and macrocalcification (>2 mm). The McNemar test was used to compare the sensitivity and specificity of US, CT, and combined US/CT for the detection of benign or malignant nodules. All statistical analyses were performed with statistical software (SPSS 19.0), and P values of less than 0.05 were considered statistically significant.
Results
Patients
The characteristics of the patients are summarized in Table 1. A total of 445 patients (333 women and 112 men; mean age = 48.3 years; age range = 13-81 years) were included in this study. Among these patients, 351 (78.9%) had benign nodules, and 94 (21.1%) had malignant nodules. Microcalcification was diagnosed in 72 patients (16.2%), and macrocalcification was diagnosed in 102 patients (22.9%).
Study Population (N = 445).

Abbreviation: PTC, papillary carcinoma; mPTC, papillary thyroid carcinoma.
Diagnostic Performances of US, CT, and US/CT
Table 2 presents the sensitivities, specificities, and accuracies of US, CT, and US/CT for the detection of benign and malignant nodules through compartment-by-compartment analysis in the 3 groups according to the type of calcification: no calcification, microcalcification, and macrocalcification.
Comparison of the Diagnostic Performance of US, CT, and Combined US/CT for Benign or Malignant Nodes According to the Type of Calcification in Thyroid Lesions Patients.
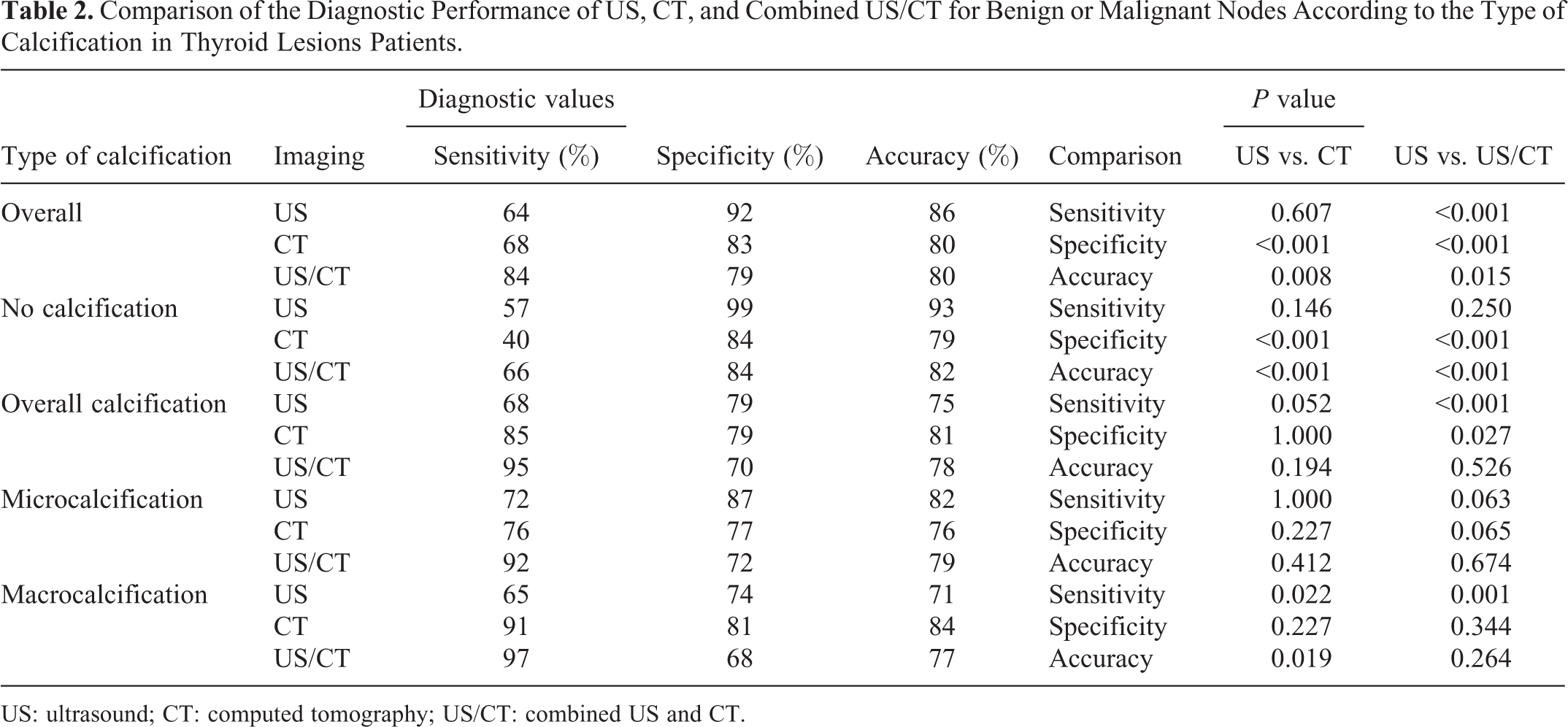
US: ultrasound; CT: computed tomography; US/CT: combined US and CT.
For all lesions, US, CT, and US/CT had sensitivities of 64%, 68%, and 84%, specificities of 92%, 83%, and 79%, and accuracies of 86%, 80%, and 80%, respectively. In all tumors, adding CT to US resulted in greater sensitivity (P < 0.001), lower specificity (P < 0.001), and lower accuracy (P = 0.015) in the identification of benign and malignant nodules.
In the group with no calcification, US, CT, and US/CT had a specificity of 99%, 84%, 84% and an accuracy of 93%, 79%, 82%, respectively. US had greater specificity than CT and combined US/CT in the identification of benign nodules (P < 0.001, P < 0.001, respectively). US had a significantly greater accuracy than CT and combined US/CT in the detection of benign and malignant nodules (P < 0.001, P < 0.001, respectively). Regarding all types of calcification (microcalcification and macrocalcification), US, CT, and US/CT had accuracies of 75%, 81%, 78%, respectively, and there was no significant difference (P = 0.194, P = 0.526). The accuracy of US in the no calcification group was significantly greater than that in the overall calcification group (P < 0.001); however, CT and US/CT were not significantly different (P = 0.534 and P = 0.381, respectively).
Regarding the group with microcalcification, US, CT, and US/CT had accuracies of 82%, 76%, and 79%, respectively. The accuracy of US was not significantly different from CT and combined US/CT in the identification of benign and malignant nodules (P = 0.412, P = 0.674, respectively). However, for the macrocalcification group, US, CT, and US/CT had sensitivities of 65%, 91%, 97%, and accuracies of 71%, 84%, 77%, respectively. Adding CT to US resulted in greater sensitivity than US in the detection of malignant nodules (P = 0.001). Additionally, CT exhibited greater sensitivity and accuracy than US (P = 0.022, P = 0.019, respectively).
Macrocalcification group divided into 2 groups with rim calcifications and non-rim calcifications (Table 3). For the rim calcifications group, US, CT, and US/CT had sensitivities of 56%, 94%, 94%, and accuracies of 66%, 84%, 74%, respectively. CT exhibited greater sensitivity and accuracy than US (P = 0.039, P = 0.024, respectively). Adding CT to US resulted in greater sensitivity than US in the detection of malignant nodules (P = 0.039). However, for the non-rim calcifications group, the accuracy of US was not significantly different from CT and combined US/CT (P = 0.625, P = 0.125, respectively).
Comparison of the Diagnostic Performance of US, CT, and Combined US/CT for Benign or Malignant Nodes According to the Type of Macrocalcification in Thyroid Lesions Patients.

US: ultrasound; CT: computed tomography; US/CT: combined US and CT.
Discussion
The overall sensitivities of combined US/CT (84%) were significantly higher than those of US (64%) for malignant nodules. However, the overall specificity of US (92%) was significantly higher than that of combined US/CT (79%) for benign nodules, and the overall accuracy of US (86%) was also significantly higher than that of combined US/CT (80%) and CT (80%) for benign and malignant nodules (Table 2). Our findings were consistent with the results of other well-designed studies. 16,32
In this study, we mainly focused on the diagnostic performance of US and CT in detecting benign and malignant nodules depending on the presence or absence of calcification and calcification size. In the no calcification group, US had greater specificity and accuracy than CT and combined US/CT. Several previous studies have shown similar results. Ishigaki S et al 32 evaluated the usefulness of multislice computed tomography (MSCT) in comparison with ultrasonography (US) for the differentiation of benign from malignant thyroid nodules, and US was found to be better than MSCT. In addition, CT underestimates the number of nodules relative to US for incidental thyroid lesions. 16
In the microcalcification group, US had greater specificity and accuracy than CT and combined US/CT, but there was no significant difference. Some studies have complemented our shortcomings because of the probable size of specimens in the microcalcification group. Several previous studies reported that US was more sensitive than CT for the detection of calcifications in thyroid nodules. 21,27 According to Lee et al., 33 US is superior to CT in the evaluation of microcalcifications. In addition, US combined with sonography-guided FNAC is a useful method for diagnosing thyroid microcalcifications. 34 Microcalcifications are more common in malignant nodules than in benign nodules. 21,27 No significant difference in CT was observed in the incidence of microcalcifications between malignant and benign nodules, and CT may have missed the microcalcifications in those nodules. 35
However, in the macrocalcification group, combined US/CT had greater sensitivity than US. CT had greater sensitivity and accuracy than US. Meanwhile, CT exhibited greater sensitivity and accuracy than US in rim calcifications group, without in the non-rim calcifications group (Table 3). The findings may explain why calcification size and type in US has a greater effect on differentiating malignant from benign nodules than that in CT. Our study also proved these findings. The accuracy of US in the no calcification group was significantly greater than that in the overall calcification group (microcalcification and macrocalcification groups); however, CT and US/CT were not significantly different. Several previous studies reported that US is superior to CT in the evaluation of microcalcifications, whereas macrocalcifications had different characteristics in US and CT. 33 Yang et al. 36 also reported an important CT feature in which the size of solitary calcified nodules increases after contrast-enhanced CT, representing a high risk for papillary thyroid carcinoma (PTC). Moreover, an interesting study 37 showed that the superiority of US for the detection of calcifications and identification of malignancy in PTC compared to that in CT was dependent on nodule size, as the performance of CT declined with the reduction of nodule size. However, there was no significant difference in the diagnostic accuracy rates of US, CT, and combined US/CT in patients with papillary thyroid microcarcinoma (mPTC). 28 We hypothesize that the relationship between calcification size and nodule size may help to distinguish benign from malignant nodules. This hypothesis warrants future study.
Our study shows that CT has greater sensitivity and accuracy than US in distinguishing benign from malignant nodules in nodules with macrocalcification, especially in rim calcifications group. Rim calcifications seriously affect the judgment of US. The structure and nature of nodule in rim calcifications may not clear in US. However, CT may not be affected by rim calcifications, which play a complementary role for US. Some studies have also reported that CT has advantages in the diagnosis of cervical lymph node metastasis compared with US. Ahn et al. 38 aimed to investigate the diagnostic ability of CT and US in the preoperative evaluation of the cervical central and lateral nodal status of thyroid cancer. The superior sensitivity of CT in per level analysis may enable CT to play a complementary role in determining the surgical extent in selected patients with thyroid cancer. Yang et al. 39 reported that CT is superior to US for detecting central LNM in patients with PTC tumor sizes > 1 cm.
Our study had several limitations. First, our study has a shortcoming, as we analyzed many papillary cancers but few other cancers. Second, this was a retrospective study from a single institution, which introduced the possibility of selection bias, including nodule for size, etc. Third, the degree of interference was unclear for US and CT based on the size of calcification and the nodule, which requires future study. Fourth, the types of nodules were lack of diversity.
In conclusion, US is superior to CT for the identification of benign and malignant nodules in all lesions. However, CT has superior diagnostic accuracy compared to US for benign and malignant nodules in lesions with macrocalcification.
Footnotes
Authors’ Note
Jian-Hui Wu and Wei Zeng contributed equally to this work. The datasets generated and analyzed during the current study are available from the corresponding author on reasonable request. Our study was approved by the Ethics Committee of the Zhongshan Affiliated Hospital of Sun Yat-sen University (approval no. 2019083). All patients provided written informed consent prior to enrollment in the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.