
Abstract
Hepatocellular carcinoma (HCC) remains to a common cause of tumor mortality worldwide and represents the most common type of lethal hepatic malignancy. The incidence of HCC is swiftly increasing in western countries and southeast Asia. Despite poor prognosis, traditional treatments for advanced HCC appear to be minimally effective or even useless since patients are usually diagnosed in the advanced stage of disease. In recent years, immune checkpoint blockade has shown promising results in multiple pre-clinical and clinical trials of different solid tumors, including advanced HCC. Novel drugs targeting immune checkpoints, such as nivolumab (anti-PD-1), durvalumab (anti-PD-L1), and tremelimumab (anti-CTLA-4) have been shown to be highly effective and relatively safe in monotherapy or in combination treatment of advanced liver cancer. Unlike other immunotherapies, this approach can rouse human anti-tumor immunity by relieving T-cell exhaustion and inhibiting the evasion of HCC by blocking co-inhibitory signaling transduction accurately. In this review, we will provide current knowledge of several major immune checkpoints and summarize recent data from clinical trials that applied immune checkpoint inhibitors alone or in combination. In addition, this review will discuss the limitations and future prospective of immune checkpoint-targeted therapy for advanced HCC.
Introduction
Hepatocellular carcinoma (HCC) is the sixth most common tumor and currently possesses the third highest cancer mortality rate globally. 1 The incidence of liver cancer shows an increasing trend every year and will maintain a high rate according to the prediction. 2-4 Despite the current progress in treatment, the 5-year overall survival of HCC is only 12%. 3,5 The etiology of HCC is mainly related to Hepatitis B virus or Hepatitis C virus infection, alcohol consumption, aflatoxin exposure, non-alcoholic steatohepatitis, or other metabolic disease. 6 The early detection of HCC may provide better outcomes for patients, but most HCC patients have already developed unresectable disease at the time of the first diagnosis. 7 Thus, the effectiveness of traditional strategies, such as partial hepatectomy, transarterial chemoembolization (TACE), and radiofrequency ablation is not sufficient for advanced HCC patients, and these treatments are always palliative. 8 During the past decade, several novel treatments have emerged; among these, immune checkpoint blockade shows promising therapeutic efficacy. The first clinical application of immune checkpoint inhibitor therapy was in 2010 9 ; thereafter, many encouraging experimental results have supported the clinical promise of immune checkpoint blockade. 10,11 Unlike traditional immunotherapies that enhance human anti-tumor immune function, immune checkpoint blockade arouses the immune response at the molecular level by retarding the co-inhibitory signal pathway, which reverses T-cell exhaustion and suppresses the immune escape of tumor cells. 12
Immune Checkpoints in HCC
The liver’s vasculature receives venous blood from the digestive tract, which exposes the liver to myriad gut pathogens and dietary components. The liver immune microenvironment must be mediated with precision to maintain immune tolerance and prevent auto-immunity. The process of immune distinction between gut pathogens allows the liver microenvironment to self-polarize, leading to immunosuppression, which profoundly modulates HCC growth by facilitating immune evasion. 13,14 Chronic liver inflammation accompanied by HCC may further polarize the liver microenvironment toward immunosuppression. 15 Therefore, in recent years, the focus of HCC immunotherapy has shifted from a single focus on stimulating the immune system to an approach that considers the immune tolerance of tumor cells. 16 Of all liver cells, hepatocytes account for 80%, and non-parenchymal cells account for 20%. The non-parenchymal liver cells include liver sinusoidal endothelial cells (LSECs), hepatic stellate cells (HSCs), Kupffer cell s(KCs), dendritic cells (DCs), and lymphocytes. 7 In the liver, LSECs account for about 50% of the non-parenchymal cells and constitutively serve as antigen-presenting cells (APCs) responsible for antigen recognition and presentation, together with KCs and DCs. These non-parenchymal cells also possess the crucial capability of maintaining self-immune tolerance by expressing immune suppression molecules, such as PD-L1 or PD-L2, and secreting anti-inflammatory cytokines, such as interleukin-10 (IL-10). 12,17,18 In the HCC tumor microenvironment, tumor cells express specific antigens that can be recognized by major histocompatibility complex (MHC) molecules on APCs and presented to T-cell receptors (TCRs) in the immune system network. 19 However, the transmission of a single stimulus signal by TCRs is insufficient to trigger T-cell activation or suppression, which requires co-regulatory signals, which can be divided into 2 categories: stimulatory and inhibitory ones (Figure 1). The stimulatory molecules expressed on T-cells, such as CD28, can bind to the corresponding ligands, such as CD80 (B7 -1) or CD86(B7-2), on the surface of APCs or cancer cells to produce a co-stimulating signal, which, together with the signal transmitted by the T-cell receptors, leads to the activation and proliferation of T-cells. On the contrary, inhibitory co-regulatory molecules can produce co-inhibitory signals that dephosphorylate T-cell receptors, leading to the development of immune evasion in HCC. 20 One type of inhibitory immune regulator is the immune checkpoint molecule. Studies have shown that the interaction between immune checkpoint molecules on the surface of immune cells and cancer cells plays a major role in HCC immune evasion. Immune checkpoint receptor-ligand pairs include PD-1–PD-L1/PD-L2, CTLA4–CD80/CD86, Tim-3–Galectin9, and LAG-3–MHC. 21 Thus, by binding to their ligands, PD-1, CTLA-4, and other immune checkpoint molecules can send out “braking signals” to turn down the first stimulatory signal transmitted by T-cell receptors. The difference is that PD-1 blockade can reverse T-cell exhaustion and function during the effector phase, while CTLA-4 blockade affects the immune priming stage. 5 T-cell exhaustion, which is strongly associated with tumor evasion, is defined as diminishing activation and proliferation of T-cells, accompanied by high expression of inhibitory immune molecules. These conditions represent a favorable preneoplastic setting. 22,23 Compared with normal effector T-cells or memory T-cells, exhausted T-cells cannot mature into memory T-cells and appear to be function degraded. 24 The inhibitory immune checkpoint signal pathway and long-term exposure of T-cell receptors to antigens have been identified as key inducers of T-cell exhaustion. 25 HCC carcinogenesis and progression are related to immune checkpoint feedback and the activation of immunosuppressive components in the tumor microenvironment, including regulatory T-cells (Tregs), myeloid-derived suppressor cells (MDSCs), and tumor-associated macrophages (TAMs), as well as anti-inflammatory cytokines. 18
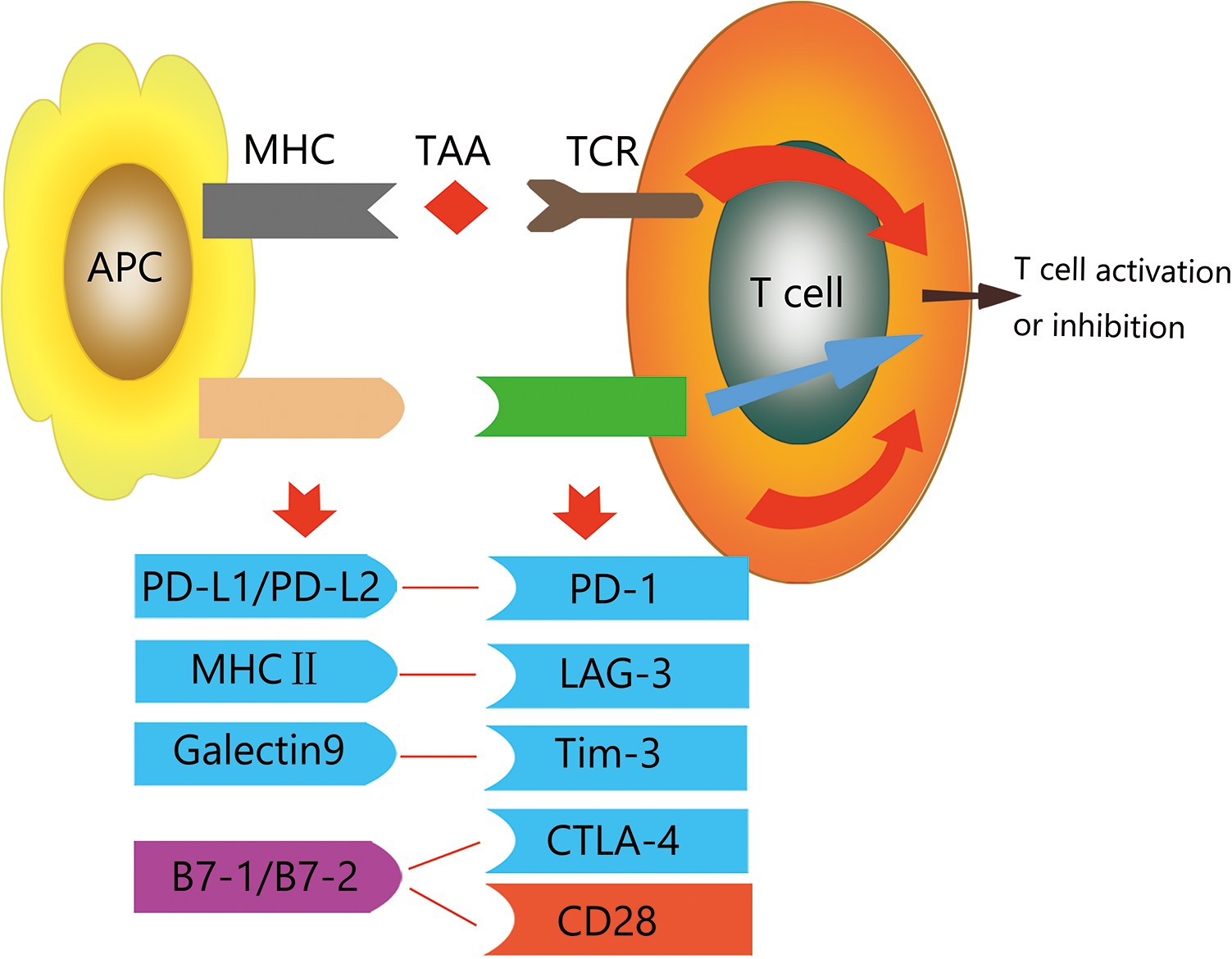
Co-stimulatory signals are marked in red; co-inhibitory signals are marked in blue. B7-1/B7-2 are marked in purple. By binding with their ligands, various pairs of co-stimulatory signals can positively or negatively affect T cell activity.
Researchers have developed monoclonal antibodies that target various checkpoints, such as immune checkpoint inhibitors (ICIs), to block the recognition of immune checkpoint molecules on tumor cells by immune cells, thus restoring the anti-tumor activity of T-cells. 26
Programmed Cell Death Protein-1 (PD-1) and Its Ligand (PD-L1/PD-L2)
Up to now, the PD-1-PD-L1/PD-L2 pair has been the most studied inhibitory immune checkpoint. This checkpoint plays a pivotal role in suppressing effector T-cell function. 21 The specific molecular mechanism is described below. When T-cells recognize the antigens of tumor tissue presented by APCs, some of them migrate and proliferate as tumor-infiltrating cytotoxic T-lymphocytes and release cytotoxic agents such as perforin and granzymes, which attack tumor cells and generate cytokines that activate the immune system in a positive feedback loop. PD-1 is an inhibitory receptor that belongs to the CD28 immunoglobulin superfamily expressed on CD8+ T-cells, B cells, NK cells, and other lymphocytes. 12 Its ligand, PD-L1, is expressed on the surface of hepatocytes, hepatic stellate cells, liver sinusoidal endothelial cells, and Kupffer cells. 12 HCC cells can up-regulate surface PD-L1 expression in response to IFN-γ or other cytokines, and the increase in PD-1/PD-L1 expression decreases T-cell activity, resulting in poor prognosis and high rates of recurrence. 27 By binding to the PD-1 receptor and its ligand, PD-L1, the first co-stimulatory signal transmitted by APCs is inhibited. 28 After that, the activation and proliferation of T-cells is diminished though SHP2; the secretion of cytotoxic factors is also reduced, leading to T-cell exhaustion. This process can be terminated by PD-1 or PD-L1 antibodies, and the tumor evasion of the immune response can thus be avoided. Such agents include nivolumab, pembrolizumab, and durvalumab.
Cytotoxic T Lymphocyte Protein-4 (CTLA-4) Pathway
CTLA-4 (CD152) mainly exists in intracellular compartments in naive T-cells at low levels and localizes to the plasma membranes of activated T-cells after TAA presentation with TCR feedback. 29 As a homologue of CD28, CTLA-4 serves as a co-inhibitory receptor, regulating the proliferation of lymphocytes. Because of its internal molecular structure, it has great affinity for competing with CD28 for its ligands (B7-1/B7-2), leading to the increased production of immune regulatory cytokines, such as IL-10 and TGF-beta. 12 Unlike the PD-1/PD-L1 pathway, CTLA-4 mainly effects T-cell activation at the priming stage. 30 After TAA recognition by the T-cell receptor, CTLA-4 can bind to B7 family molecules to generate a second co-inhibitory signal downstream, which activates IDO that suppress the response of T-cells and interferes with the binding of CD28 molecules to the B7 family. 31 CTLA-4 also acts as a mediator, constitutively presented on Tregs, that contributes to self-immune tolerance, which unfortunately also provides an opportunity for HCC immune evasion. 32 The most commonly used CTLA-4 inhibitors are ipilimumab and tremelimumab.
Mucin Domain-Containing Molecule-3 (Tim-3) Pathway
Tim-3 is an immunosuppressive transmembrane protein first identified on IFN-γ-secreting CD4+ T-helper 1 cells and also present on CD8+ cytotoxic T-cells, NK cells, and DCs. 33 The most well studied Tim-3 ligand is galectin-9. Tim-3 plays a crucial negative regulatory function in the T-cell immune response, contributing to immune dysfunction and Th1 cell apoptosis, and impairing the ability of T-cells to produce IFN-γ by binding with its ligand galectin-9. 34 -36 Compared with adjacent tissues, Tim-3 expression is enriched in CD4+ and CD8+ T-cells in HCC. Increased expression of Tim-3 in tumor-infiltrating T-cells in chronic HBV infection indicates T-cell exhaustion and predicts poor prognosis in advanced HCC patients. 37 The blockade of Tim-3 results in the enhanced expansion of HBV-specific CTLs, and the molecular mechanism of Tim-3 suggests its role as another practical immunotherapeutic molecular target. 36
Lymphocyte Activation Gene 3 Protein (LAG-3) Pathway
LAG-3 is an immunoglobulin membrane protein that binds with MHC-II molecules. LAG-3 conducts inhibitory signal to suppress T-cell co-stimulatory function and cytokine production. 38 LAG-3 is significantly upregulated in tumor-infiltrating CD8+ T-cells in the context of T-cell exhaustion. 39 Currently, the combination of anti-LAG-3 with PD-1 blockade is under testing in a phase I trial (NCT01968109). The synergistic effect of immune checkpoint combination in advanced HCC treatment has received enthusiastic attention.
Results of Clinical Trials of Immune Checkpoint Inhibitors
Currently, multiple clinical trials are underway to verify the efficacy and safety profile of immune checkpoint inhibitors. According to recent data from in vitro experiments, antibodies against PD-1/PD-L1, Tim3, or LAG3 can restore the responses of HCC-derived T-cells to tumor antigens, and combinations of these antibodies have additive effects. 22 We have summarized some ongoing clinical trials of representative immune checkpoint inhibitors in Tables 1, 2, and 3.
Summary of Ongoing Clinical Trials of Immune Checkpoint PD-1 Inhibitors for Hepatocellular Carcinoma.

Summary of Ongoing Clinical Trials of Immune Checkpoint PD-1 Inhibitors for Hepatocellular Carcinoma.

Summary of Ongoing Clinical Trials of Immune Checkpoint PD-L1 and CTLA-4 Inhibitors for Hepatocellular Carcinoma.

PD-1 and PD-L1 Inhibitors
Compared with other immune checkpoint inhibitors, PD-1/PD-L1 blockade is associated with a relatively high objective response rate (10%-20%) and a good safety profile. The first report of PD-1 blockade in advanced HCC patients was in 2015 at the American Society of Clinical Oncology Annual Meeting. The PD-1/PD-L1 pathway is currently considered to be a promising target of immune checkpoint therapy.
Nivolumab is a fully human IgG4 anti-PD-1 antibody approved by the FDA in 2017 for advanced HCC patients who had previous sorafenib treatment or sorafenib resistance. A prospective, multi-cohort, open-label, non-comparative, phase I/II trial of nivolumab as well as nivolumab in combination with ipilimumab in advanced HCC patients with or without chronic viral hepatitis (NCT01658878, CheckMate 040) was completed recently. In this study, nivolumab was assessed as a first-line treatment in advanced HCC patients with no previous sorafenib treatment or sorafenib intolerance and as a second-line treatment in patients who had disease progression after receiving sorafenib. Forty-eight eligible patients were treated with nivolumab 0.1-10mg/kg every 2 weeks during the dose-escalation phase; another 214 advanced HCC patients were treated with nivolumab 3.0 mg/kg during the dose-expansion phase. Nivolumab displayed a manageable safety profile as well as acceptable tolerability. The outcomes revealed that objective response rates (ORR) of 15% and 20% for the dose-escalation and dose-expansion phases, respectively. The disease control rates were 58% and 64%, respectively. In addition, the median overall survival (OS) was 15.0 months, and the median time to progression (TTP) was 3.4 months in the dose-escalation phase. In the dose-expansion phase, TTP was 4.1 months. 40 The experimental results yielded a safety profile suggesting that nivolumab is effective in advanced HCC patients, and, based on this trial, the FDA accelerated the approval of nivolumab as a second-line treatment for advanced or metastatic HCC patients who had previously received sorafenib. The favorable results of this study led to another randomized, open-label, multi-center, phase III trial of Opdivo (nivolumab) vs. sorafenib as first-line treatment in advanced HCC patients. The trial, sponsored by Bristol-Myers Squibb, is already active and will be completed in 2021 (NCT02576509, CheckMate-459). In that study, the primary outcome measure will be OS, and the secondary outcome measures will be ORR and progression-free survival (PFS). However, the data released recently for OS did not achieve statistical significance (https://clinicaltrials.gov/ct2/show/NCT02576509).
Pembrolizumab is an anti-PD-1 humanized IgG4 antibody, which presents inhibition to a variety of metastatic cancers. In 2019, the FDA approved pembrolizumab for the treatment of unresectable or metastatic melanoma. In the field of HCC treatment, a non-randomized, open-label, multi-center, phase II study of pembrolizumab as monotherapy in advanced HCC patients (NCT02702414, KEYNOTE-224) was first presented at ASCO in 2018 and is estimated to complete before June 2021. The trial aims to evaluate the effectiveness and safety of pembrolizumab in the treatment of advanced HCC that has not responded to treatment with sorafenib and in patients who cannot tolerate sorafenib. The primary outcome of this trial is ORR, and duration of response (DOR) will serve as a secondary outcome. The interim data showed that ORR was approximately 16.3%, and the disease control rate was 44%, with median OS of 12.9 months and TPP of 4.9 months. However, the safety profile of pembrolizumab monotherapy requires attention, as approximately 73% of patients experience adverse events; 20% of such cases are serious adverse events, such as grade 3/4 hepatotoxicity. 41 Another randomized, double-blind, phase III trial was conducted to evaluate the efficacy of pembrolizumab with best supportive care vs. placebo with best supportive care after systemic treatment in advanced HCC patients (NCT02702401, KEYNOTE-240). However, the improvements in OS and PFS in advanced HCC patients in the pembrolizumab cohort were not significantly different from those in the placebo group. Nonetheless, pembrolizumab has a good safety profile. 42
A phase I/II trial of durvalumab monotherapy for HCC patients has been completed. The results were published in 2017 (NCT01693562). Among 40 enrolled HCC patients, the overall response rate was 10.3%, and the median OS was 13.2 months. 43 A randomized, open-label, multi-center, phase III study of durvalumab and tremelimumab as first-line treatment in advanced HCC patients with no prior systemic therapy is ongoing. The primary outcome of this trial is OS (NCT03298451). 44 Another randomized, open-label study of durvalumab as monotherapy or in combination with tremelimumab or bevacizumab in advanced HCC patients is currently active (NCT02519348).
CTLA-4 Inhibitors
Tremelimumab, the first practical CTLA-4 blockade inhibitor for HCC patients, is still not approved by the FDA, but several clinical trials of combination therapy that includes tremelimumab are currently ongoing (Table 3). Some of these clinical trials have already provided encouraging results. A non-randomized, open-label, multi-center, phase II study (NCT01008358) of an anti-CTLA-4 monoclonal antibody (CP-675,206, tremelimumab) for the treatment of advanced HCC patients was completed, and the encouraging outcomes were published in 2013. 45 Patients with chronic HCV infection or unresectable disease were treated with tremelimumab monotherapy at a dose of 15 mg/kg every 90 days until disease progression or severe toxicity development. Among all 21 patients enrolled, the partial response rate was 17.6%, while the disease control rate was 76.4%. The median OS was 8.2 months, while the median time-to-progression was 6.48 months (95% confidence interval: 3.95–9.14). The results showed a good safety profile: the drug was well tolerated, and the adverse events were mild. Although approximately 45% of patients had grade 3 or 4 elevations in transaminases after the first dose, liver function usually remained stable. Interestingly, the researchers also observed a >200-fold decrease in serum viral load in 12 HCV ipatients, which suggests that CTLA-4 inhibitors or tremelimumab may have an impact on virus control in HCC patients. 45 Another non-randomized, open-label, phase I pilot study of tremelimumab in combination with RFA or TACE was published in 2017 (NCT01853618). Thirty-two HCC patients were enrolled, and 19 of all participants were evaluated as candidates for subsequent ablation. The results revealed that 5 patients achieved a confirmed partial response, while 12 of 14 HCV patients were observed to have decreased viral load. Patients who showed clinical benefits had a clear increase in CD8+ T-cells. The median OS was 12.3 months. The 6-month and 12-month probabilities of PFS were 57.1% and 33.1%, respectively, with no dose-limited toxicity encountered. 46
Targeting Combination Therapy to the Immune Checkpoint in HCC
Multiple anti-tumor immune approaches have already been used in advanced HCC treatment, with impressive outcomes. However, contradictory results are also observed, suggesting that immune checkpoint blockade require further research. Immune checkpoint blockade can lead to disinhibition of the liver’s immunosuppressive microenvironment, while other anti-tumor approaches, such as antiangiogenic drugs or ablation treatment, may stimulate the immune system. 47 At the present time, combined immunotherapy for HCC has received wide attention. Various approaches can act on many aspects, providing new effective schemes for individualized clinical treatment. 12 The focus of experiments being conducted by companies has been on combination strategies. Currently, primary combination immunotherapy for HCC includes immune checkpoint blockade, immune checkpoint blockade plus locoregional approaches or chemotherapies, and immune checkpoint inhibition plus antiangiogenic drugs. Several trials are ongoing, while some have already been completed, with published results. Those studies are summarized in this section.
Combination of Multiple Immune Checkpoint Inhibitors
Data from preclinical trials of immune checkpoint combination treatment in a series of patients with solid tumors showed higher overall survival and response rate, compared with the results of monotherapy. 48 This also provides a platform for dual immune checkpoint treatment in advanced HCC. As summarized above, nivolumab (anti-PD-1) and ipilimumab (anti-CTLA-4) were employed together in treatment and showed encouraging outcomes in the Check-Mate 040 study (NCT01658878). Since the blockade of PD-1/PD-L1 requires activated CD8+ T-cells, activation of the anti-CTLA-4 pathway may increase the number and anti-tumor ability of cytotoxic T-cells by binding with its ligands, which can enhance the efficacy of PD-1 blockade. 22,47 Blocking the PD-1 and CTLA-4 pathways simultaneously, as the focus of current trials, has already achieved better anti-tumor efficacy than either antibody monotherapy in malignant melanoma. 49 In regard to HCC, a phase I/II study was conducted to assess combination treatment with durvalumab (anti-PD-L1) and tremelimumab (anti-CTLA-4), as mentioned above (NCT02519348). The data from phase I showed that the confirmed overall response rate was 15%, and the sum of the complete and partial response rates was 20%, among 40 enrolled participants. The most common treatment-related grade ≥3 adverse event was an asymptomatic increase in AST (10%). 50 The results suggested that combination treatment possesses a better safety profile and may be more effective than immune checkpoint inhibitor monotherapy. Another phase III study of durvalumab and tremelimumab combination therapy vs. durvalumab monotherapy is underway to reveal the difference between these 2 kinds of treatment (NCT03298451).
Combination of Angiogenesis Inhibitors and Immune Checkpoint Inhibitors
Sorafenib, lenvatinib, and other tyrosine protein kinases inhibitors (TKIs) remain first-line therapy for advanced HCC patients. TKIs can not only present anti-angiogenic effects but also enhance the process of synergistic immunotherapy by regulating the expression of immune checkpoint molecules. They may strengthen the drug function of immune checkpoint inhibitors, while the latter can potentially reduce acquired anti-angiogenesis drug resistance in patients. 47,51 A phase I trial of combination therapy with bevacizumab and atezolizumab in HCC patients was conducted, and the interim results indicated that the RECIST criteria response rate was 32%. As for the safety and tolerability of drugs, approximately 27% of participants experience grade 3-4 treatment-related adverse events (typically hypertension). Interestingly, patients with HCV infection or AFP ≥400 ng/mL appeared to have more responses, 78% (52% for 6 months or more, 26% for 12 months or more) of which persisted over 6 months. 52 The progress of this study led to a randomized, phase III trial to compare atezolizumab plus bevacizumab with sorafenib as first-line treatment (NCT03434379). 53 By August 29, 2019, the primary analysis date, the hazard ratio for death with atezolizumab–bevacizumab was 0.58 of that with sorafenib. OS at 12 months and median PFS were 67.2% and 6.8 months in the atezolizumab–bevacizumab group, compared to 54.6% and 4.3 months in the sorafenib group. The incidence of grade 3 or grade 4 adverse events was approximately 55% in both groups. The updated results revealed that, in patients with unresectable HCC, atezolizumab combined with bevacizumab resulted in better OS and PFS outcomes than sorafenib. 54 Another phase I trial of lenvatinib plus pembrolizumab for HCC patients is underway, and preliminary results were reported at the ASCO meeting in 2018 (NCT03006926). The RECIST criteria response rate was 42% of 26 evaluated patients, and the median PFS was 9.69 months. The adverse events rate showed an acceptable safety profile, with 17% hypertension and 17% alanine aminotransferase elevation. 55 A phase Ib trial of axitinib in combination with avelumab as first-line treatment in HCC patients was recently completed, and the results showed good tolerance and RECIST ORR of 13.6% (NCT03289533). 56
Combination of Locoregional Therapy With Immune Checkpoint Inhibitors
In the HCC setting, one of the key reasons to apply locoregional treatment such as radiofrequency ablation (RFA) or transcatheter arterial chemoembolization (TACE) is to release tumor-associated antigens or neoantigens from HCC tissue into the circulatory system. This process can boost the efficacy of immune molecule-targeted inhibitors in the HCC microenvironment. Several trials on the combination of immune checkpoint inhibition and local treatment are currently underway. A non-randomized, open-label, phase I trial of nivolumab plus TACE is recruiting and aims to evaluate the safety of this therapy in 3 cohorts (NCT03143270). 57 Another open-label, phase II trial of TACE combined with nivolumab in intermediate-stage HCC is also recruiting, with ORR as the primary outcome measure (NCT03572582). The latter treatment will be divided into a 4-week cycle, and nivolumab will be administered at a dose of 240 mg every 2 weeks. The outcomes are eagerly awaited. At present, nivolumab is not the only immune checkpoint inhibitor administered; one phase Ib study investigated the use of TACE with doxorubicin solution and gelatin sponge particles followed by pembrolizumab at a dose of 200 mg (NCT03397654). The primary endpoint of the study was safety profile evaluation; PFS was measured as a secondary outcome. Tremelimumab, another immune checkpoint inhibitor, was tested by Duffy et al. as a local treatment in 32 advanced HCC patients. Nineteen of 32 patients were evaluated, and 26.3% (5 of 19) achieved a confirmed partial response. The median PFS was 7.4 months, and decreases in viral load were observed in 12 patients infected with HCV (12 of 14). 46
Challenges of Immune Checkpoint Inhibitor Therapy in Advanced HCC
Firstly, HCC is a malignancy with high incidence, mortality, and recurrence. 4 Considering the variety in tumor staging (most patients are diagnosed at advanced stages) and the clinical condition of HCC patients, the management of immunotherapy (including immune checkpoint blockade) can be complex. 58,59 As a result, the individualized administration of immune checkpoint-targeted therapy combined with traditional treatment should be applied with flexibility. Limitations of the use of immune checkpoint inhibitors in HCC patients vary among individuals. The incidence and severity of treatment-related adverse events are the first considerations. According to the data available so far, the most common adverse events are fatigue and fever. 60 Severe adverse reactions may appear as a grade 3/4 rise in AST, pemphigoid, or adrenal insufficiency. Severe adverse reactions such as these require more attention; it is important to figure out the root cause in order to reduce treatment-related hepatotoxicity. A few patients may also experience serious adverse events involving different organs such as skin, gut, and lung. Fortunately, the toxicity of immune checkpoint inhibitor monotherapy or combination treatment appears to be milder than that of molecule-targeted agents such as tyrosine-kinase inhibitors. 29,61
Another issue that requires our attention is the necessity of identifying predictive biomarkers in order to protect patients who respond poorly to ICIs from potentially life-threatening toxic effects. Although PD-L1 expression in tumor tissue is currently the most widely studied biomarker, previous research has shown that the expression of PD-L1 in advanced HCC does not affect the rate of an objective response to anti-PD-1 therapy. 40,62 Microsatellite instability (MSI) is a hypermutation caused by a mismatch repair defect (dMMR), and it is the first FDA-approved predictive biomarker for anti-PD-1 therapy. 63 However, MSI seems to be a rare event in HCC. 64 Tumor mutational burden (TMB) is the sum of non-synonymous mutations in the coding region of the somatic genome. Non-synonymous somatic mutations alter the amino acid sequence of the protein encoded by the affected gene, thereby forming neoantigens and helping to enhance the immunogenicity of tumor cells. On the other hand, a large number of studies have shown that TMB can also play a key role in predicting the response to ICIs. 65,66 When compared with other types of tumors, HCC was found to have a higher average TMB and is expected to respond well to ICI. 67 Interestingly, in a study that included the metagenomic sequencing of periodic fecal samples, Zheng et al. characterized the gut microbiome during anti-PD-1 immunotherapy in HCC. They observed that the stool samples of patients who responded to PD-1 (n = 3) had richer microbial composition than did those of non-responders (n = 5), which indicates that the role of the gut microbiome in response to ICI immunotherapy in HCC needs to be further investigated. 68 Agent resistance is also considered a difficult challenge in the treatment of patients with HCC or other solid tumors, since the incidence rate is notable, and the underlying mechanism needs to be clarified. 69,70 Despite these promising responses, the majority of patients demonstrate primary or acquired resistance, failing to respond to ICI or experience relapse after treatment. 71 Few efforts to elucidate HCC-specific resistance to ICI have focused on the underlying mechanisms, understanding of which is essential for the development of combination therapies. 38 For example, tumors with a low mutation rate, such as pancreatic and prostate cancer, are poorly immunogenic and resistant to anti-PD-1 agents. 72 Therefore, sensitivity to ICIs would likely be restored by treatment facilitating the release of tumor antigens, including radiotherapy and chemotherapy. 73 Previous research has shown that resistance to ICI therapy is associated with elevated Foxp3+/CD8+ Treg cell ratios. 74 Thus, monoclonal antibodies that selectively deplete tumor-associated Treg act synergistically with anti-PD-1/PD-L1 therapy in animal models of ICI-resistant cancer. 75 -77
Conclusion
HCC pathogenesis is a complex course, with multiple immune-related signal pathways involved. Considering this rationale, novel immune checkpoint blockade agents were developed and play a pivotal role in tumor escape inhibition. In this review, we summarized liver immune microenvironment function and the mechanism of HCC immune escape, as well as the action of immune checkpoint blockade. Ongoing trials have also been listed to provide additional perspective on immunotherapy in advanced HCC. Based on the encouraging results of multiple completed and ongoing trials, immune checkpoint combination treatment will be the focus of future efforts to improve the prognosis of patient with advanced HCC. In the next decade, more clinical evidence will expand current knowledge about the role of the immune system in the occurrence and development of HCC, and the mechanism of new potential immune biomarkers will be explored and demonstrated. Further basic and clinical studies are eagerly needed to elucidate the safety and efficacy of novel immune checkpoint inhibitors.
Conflict of Interest Statement: No conflict of interest exits in the submission of this manuscript, and the manuscript has been approved by all authors for publication. I would like to declare on behalf of my co-authors that the paper was original work that has not been published previously and is not under consideration for publication elsewhere, in whole or in part. All the authors listed have approved the manuscript that is enclosed.
Footnotes
Abbreviations
Authors’ Note
Bai ji and Yahui Liu contributed equally. No animal and human studies were included in this review.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China (NSFC; No. 81802805), the Jilin Province Health Technology Innovation Project (No.2017J047), and the Jilin Province Medical Scientist Fund Project (3D5197909428).