
Abstract
Breast-conserving surgery is facing the challenge of objective tumor margin identification intraoperatively. Near-infrared fluorescence imaging would be an ideal approach to visualize tumor margins during surgeries. In this preliminary study, the feasibility of methylene blue–based near-infrared fluorescence imaging technique for breast cancer detection was assessed in resected human breast specimens after breast cancer surgeries. Thirty patients with breast cancer scheduled for surgical treatment were enrolled, including 10 patients with preoperative chemotherapy and 20 patients without. Each of them received an injection of 1 mg/kg methylene blue intravenously 3 hours before the surgery. Then, a home-developed methylene blue–specific near-infrared fluorescence imaging system was employed to image the resected breast tissues and identify the tumor by the fluorescence contrast. Specimens were taken for pathological examinations as the reference. There were no severe adverse events attributable to methylene blue. Of 20 patients, who did not receive preoperative chemotherapy, 16 exhibited fluorescent contrast on their resected tissues (signal-to-background ratio: 1.94 ± 0.71). In contrast, tumors were identified in 3 of 10 specimens from patients who underwent preoperative chemotherapy (signal-to-background ratio: 1.63 ± 0.38). A total of 35 tissues were sampled from 30 specimens. Besides 30 tumor samples, 5 more suspicious samples with fluorescence signal were confirmed to be benign hemorrhagic tissues. Therefore, a sensitivity of 0.63 and a positive predictive value of 0.79 were achieved by the methylene blue fluorescence imaging strategy. Here, we demonstrate the feasibility of using methylene blue fluorescence imaging to identify breast cancer. Preoperative chemotherapy had an impact on imaging effect, which may reduce the detection rate. After all, methylene blue fluorescence imaging has great potential to be used into breast-conserving surgery for tumor-positive margins detection, but further clinical trial study is needed (http://www.chictr.org.cn/ Clinical Trial Registry ID: ChiCTR1800015400, Near-infrared fluorescence imaging applied in breast cancer identification with methylene blue).
Keywords
Introduction
Breast cancer is 1 of the 3 most common cancers worldwide and is especially a common malignancy in women. 1 Cancer statistics from 2018 estimate that breast cancer accounted for approximately 30% of all cancer cases and 14% of cancer deaths among women. 2 Common surgical treatments for solid breast tumors include mastectomy and breast conservation therapy. 3 In the era of precision medicine, breast-conserving surgery (BCS) leads to minimal trauma and is followed by rapid recovery, which is a standard option for patients. For BCS, one of the most important elements to improve survival and reduce the need for subsequent adjuvant therapies is the acquisition of negative cutting edge. 4 However, removal of tumors with negative margins is challenging in BCS due to the lack of a convenient and objective method to assist breast cancer identification, intraoperatively. It has been reported that 11% to 40% BCS patients had to perform re-excision due to inadequate margins. 5 -7 A real-time intraoperative and breast cancer–specific imaging approach is highly desirable to minimize the rates of re-excision, unnecessary radical resections, and possible overtreatment. 4,8
Currently, tumor detection methods during surgery rely on visual palpation, intraoperative ultrasound, and frozen section analysis. 9 Although useful, these methods are experience dependent, time-consuming, and constrained by sample errors. 10 Therefore, an intraoperative imaging method as an adjunct to them can be both helpful to surgeons in recognizing breast tumors during resection and to pathologists in locating suspicious lesions in resected tissues for rapid pathological examination. 11
Near-infrared (NIR) fluorescence imaging (FI) has been reported for intraoperative applications because of its ability to identify tumor margins, sentinel lymph nodes (SLNs), and vital structures (blood vessels, nerves, and so on) in real time with no ionizing radiation. 12 -16 At present, only indocyanine green (ICG) and methylene blue (MB) are approved by the Food and Drug Administration 17 as clinically available NIR fluorescence dyes. Indocyanine green–based NIR-FI is proven to be very successful in SLN detection in breast cancer surgeries. 14,18 -20 However, it is seldom applicable for breast cancer imaging, which hinders the clinical impact of NIR-FI.
Different from ICG with excitation and emission wavelength of 780 nm and 820 nm, respectively, MB can be excited by 665 nm light, and its peak emission is in 686 nm. Several groups have demonstrated the feasibility and benefits of using MB-based NIR-FI for tumor lesion detection during surgeries, such as the identification of the solitary fibrous tumor in pancreas, 21 the parathyroid adenomas, 22,23 and the paraganglioma. 24 There was only 1 study performed by Tummers et al in the Netherlands using MB-FI for breast cancer identification, 25 in which 20 of 24 patients with breast cancer showed effective fluorescent signal in tumors. This opened a new door of using intraoperative MB-FI for breast cancer surgeons and pathologists to achieve more precise and faster surgical treatment.
The purpose of our work was to pursuit this direction and verify the feasibility of using MB and our home-developed MB-specific NIR-FI system for breast cancer detection in resected human tissues during mastectomy and BCS.
Materials and Methods
Fluorescence Imaging System
In this study, the MB-FI system used to detect breast tumors was developed by the CAS Key Laboratory of Molecular Imaging. The system was designed to detect the MB emission wavelength (Figure 1A). Because the excitation and the emission wavelengths of MB are relatively close, in order to minimize the light pollution of the excitation light to the imaging, we chose the upper edge of MB peak excitation spectrum to be 650 nm and the lower edge of MB peak emission spectrum to be 695 nm as the parameters of the system. The system mainly included 3 components (Figure 1B): (1) Image acquisition: the NIR-fluorescence signal was detected using a lens (FL-CC0814A-2M; Ricoh Co, Ltd, Tokyo, Japan), through the light filter (narrow band pass filter, 695 ± 10 nm), then transmitted to a charge-coupled device camera (MVC1300MF-M00; Beijing Microview Science and Technology Co, Ltd, Beijing, China). (2) Illumination design: a 650-nm NIR excitation light source was used (L-650/5WF; Zhongshan You Sheng Photoelectric Technology Co, Ltd, Zhongshan, Guangdong, China) to provide the source light. (3) Imaging and control component: process the signal and obtain the images by using the imaging software designed by the Key Laboratory of Molecular Imaging, Beijing, China. Real-time imaging data were recorded in video rate. However, the system, as a prototype equipment, was unable to display white light and fluorescence images simultaneously.

System and experiment workflow. (A) Methylene blue–fluorescence imaging (MB-FI) structure and principle, (B) MB-FI system, and (C) Experiment workflow. MB-FI was performed on resected breast tissues in the pathology room.
Patients
Patients were enrolled according to the hospitalization order. Thirty female patients (age 32-68 years, median age 53 years) diagnosed with breast cancer who were scheduled for resection surgery were enrolled in this study between March 2018 and August 2018. The clinical trial was registered at the Chinese Clinical Trial Registry (http://www.chictr.org.cn/, ChiCTR1800015400) and approved by institutional review board of the hospital (20171105). All patients provided written informed consent to be examined in this study. Both patients with and without preoperative chemotherapy were enrolled, and the preoperative chemotherapy was taxotere–epirubicin–cyclophosphamide. Magnetic resonance imaging (1.5 T EXCITE HD, GE. Repetition time = 6.1 milliseconds, echo time = 2.9 milliseconds, inversion time = 13 milliseconds, and field of view = 36 × 36 cm) was applied to patients for clinical examination with the contrast agent Gd-DPTA. Breast tumors of enrolled patients included invasive ductal carcinoma (IDC) in 22 patients, mixed carcinoma in 4 patients, mucinous adenocarcinoma (MUC) in 1 patient, and ductal carcinoma in situ (DCIS) in 3 patients. Patients with a history of severe food or drug allergy, diabetes, or serious organ diseases such as those of the heart and lung, abnormal liver and kidney function, pregnancy, or lactation were excluded from the study.
Imaging Procedure
Methylene blue was purchased from Jumpcan Pharmaceutical Group Co, Ltd, Taixing, China. Patients were given MB through a peripheral vein 3 hours before surgery. To determine the appropriate experimental conditions, the first 3 experimental cases were administered with a dose of 0.5 mg/kg of MB intravenously to each, but this dosage failed. Subsequently, we increased the dose to 1 mg/kg of body weight. This dose led to a detectable fluorescence signal in tumor areas, and the following 30 patients enrolled in the study were administered according to this dose standard.
The trial was performed on ex vivo specimens from patients with breast cancer in the pathology room next to the operating room. After routine injection of MB, patients received surgical treatment, either modified radical mastectomy (MRM) or BCS. During the experimental process, the surgical procedure was not influenced by MB-FI (Figure 1C). After surgical resection, the MB-FI of breast surgical specimens was performed ex vivo in the pathology room, in order to detect breast tumors. Then, the sampled tissues were sent for pathological examination. The fluorescence images were displayed and recorded in video rate. Because of the limitation of the penetration depth by FI, the specimens were bisected longitudinally based on the locations of the breast masses. In this study, the signal-to-background ratio (SBR) threshold value was defined at 1.3, according to the imaging results and corresponding pathological examinations of first 6 cases. The identified breast masses, nondetectable masses by MB-FI and other suspicious tissues with fluorescence signal detected, were removed and set aside for pathological examinations. According to the standard pathological procedure with hematoxylin and eosin (H&E) staining analysis, all the sampled tissues were examined by pathologists.
Statistical Analysis
Signal-to-background ratio was quantitatively determined based on the recorded images. To calculate the SBR, we delineated the region of interest (ROI) using the image-processing software ImageJ (National Institutes of Health, Bethesda, Maryland). Then, the mean brightness value of the ROI (BROI) was calculated within a range of 0 to 255. Surrounding tissue brightness was calculated 3 times in different locations in the same way and averaged as the background brightness (Bbackground). The SBR values were obtained by dividing BROI by Bbackground and was calculated 3 times and averaged to reduce calculation error.
Mann-Whitney U test was used to evaluate differences in the variables. Pearson χ2 test or Fisher exact test (2 sided), if appropriate, was used to analyze the variable distribution differences between the 2 tumor groups (fluorescence signals detectable and nondetectable). Based on the pathological examination results of the sampled tissues, sensitivity and positive predictive rate were calculated, respectively. Data calculations, graphing, and analysis were performed using SPSS Version 25 (IBM Corporation, Armonk, New York) and GraphPad Prism Version 7 (GraphPad Software Corporation, San Diego, California). P values <.050 were considered statistically significant.
Results
General
A total of 30 patients who met study criteria were included in this study, of which 10 patients had received preoperative chemotherapy and 20 patients did not. In nonpreoperative chemotherapy group, 16 of 20 resected breast tissues showed detectable fluorescent signals in tumor areas using our MB-FI system. Of 10 tumors, 3 were detected in specimens of patients with preoperative chemotherapy (Figure 2A). Therefore, 19 of 30 resected breast tissues showed detectable fluorescent signals, while the other 11 were nondetectable. Patients’ characteristics are counted in Table 1. During experiments, there were 5 extra suspicious tissues with fluorescence light spots in the nonpreoperative chemotherapy group (SBR: 2.19 ± 0.40). Fluorescence intensity between tumors and suspicious tissues was calculated (Figure 2B). The mean SBR for tumors was 1.94 ± 0.71 (range: 1.31-3.90) and 1.63 ± 0.38 (range: 1.39-2.06) in the nonchemotherapy and chemotherapy group, respectively (Figure 2C). Representative white and fluorescence images of tumor in nonchemotherapy group, tumor in chemotherapy group, and suspicious tissue in nonchemotherapy group are shown in Figure 2D to F. After statistics, a total of 35 sampled tissues were collected, including 30 tumor tissues of every enrolled patients and 5 suspicious tissues.
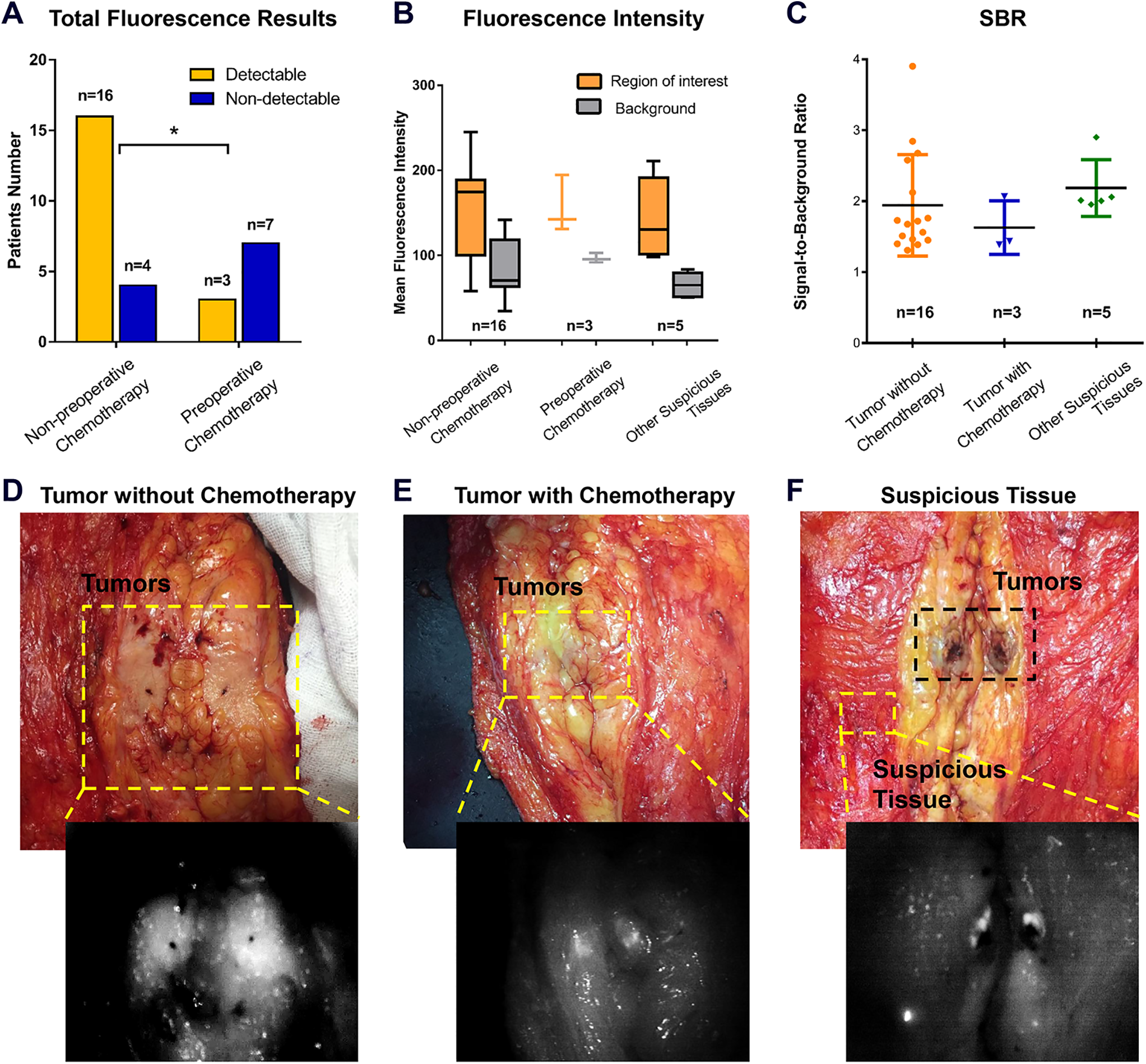
Fluorescence imaging statistics and representative images of tumors and suspicious tissue. A, Total fluorescence imaging results between groups with and without chemotherapy. B, Fluorescence intensity between tumors of nonpreoperative chemotherapy, tumors of preoperative chemotherapy, and suspicious tissues. C, Signal-to-background ratio (SBR) between 3 different groups, tumor without chemotherapy: 1.94 ± 0.71; tumor with chemotherapy: 1.63 ± 0.38; and other suspicious tissues: 2.19 ± 0.40. D, White light and fluorescence images of tumor (yellow frame) without chemotherapy. E, White light and fluorescence images of tumor (yellow frame) with chemotherapy. F, White light and fluorescence images of suspicious tissue (yellow frame).
Patients Characteristics with 1 mg/kg MB.a

Abbreviations: BCS, breast-conserving surgery; BMI, body mass index; DCIS, ductal carcinoma in situ; ER, estrogen receptor; Her2/NEU, human epidermal growth factor receptor 2; IDC, invasive ductal carcinoma; ILC, invasive lobular carcinoma; MB, methylene blue; MRM, modified radical mastectomy; MUC, mucinous adenocarcinoma; PR, progesterone receptor.
a N = 30.
During the intravenous injection of MB, 2 of the enrolled patients had mild vascular pain. No other serious adverse reactions were noted.
Breast Tumor Imaging
Nineteen of 30 resected breast tissues showed detectable fluorescent signals in the tumor areas by our MB-FI system (Figure 1A and B), while the other 11 were nondetectable (Table 1). Statistical analysis revealed that preoperative chemotherapy influenced the imaging performance significantly (Table 1; P < .05). For patients without preoperative chemotherapy, MB-FI visualized tumors in 16 of 20 tissues. One of the imaging results is shown in Figure 3A. According to the location of the tumor detected by palpation, the breast cancer specimen of this patient was longitudinally bisected ex vivo to expose the tumor to the surface. Fluorescence signals were detected in the tumor areas. Sliced tissue with tumor was demonstrated to be IDC. No fluorescence signals were detected in the necrotic tissue areas.

Imaging results of patient 15 with invasive ductal carcinoma (IDC) and patient 30 with mucinous adenocarcinoma (MUC). A, (a) magnetic resonance (MR) image, tumor pointed by red arrow, tumor size: 2 cm; (b-d) Tumor bisected in specimen, tumors pointed by black frame in (b), signal-to-background ratio (SBR): 2.68 ± 0.60, suspicious tissue circled by black frame in (d); (e) hematoxylin and eosin (H&E)–stained image of suspicious tissue indicated by black frame in (d) and hemorrhage area marked by large red arrows in (e). Scale bar: 300 µm. (f-h) Sliced tissue with breast tumor and necrosis, grade III, estrogen receptor (ER)+, progesterone receptor (PR)+, and Her2/NEU+. (i) H&E-stained image of breast tumor in fluorescence signal detectable area (pointed by red arrow). Scale bar: 100 µm; (j) H&E-stained image of necrotic tissue (pointed by black arrow). Scale bar: 100 µm. B, (a) Fluorescence image of MUC, tumor size: 2 cm; (b) Color image, tumors pointed by black frame; and (c) H&E-stained image. Scale bar: 300 µm.
The 4 tissues with undetectable signals in nonpreoperative chemotherapy group comprised 1 case of MUC (Figure 3B) and 3 cases of IDC. In addition, in 1 specimen from a patient with mixed carcinoma including MUC, IDC, and invasive lobular carcinoma (ILC), fluorescence signals were detectable in all suspected tumor areas except the MUC area (Supplementary Figure S1). In contrast, only 3 of 10 breast tissues showed fluorescent contrast in the preoperative chemotherapy group. All the 10 patients in the preoperative chemotherapy group were diagnosed with IDC.
Suspicious Tissue Imaging
In the nonpreoperative chemotherapy group, besides acquiring 20 malignant tissue samples inside breast tumor areas, 5 extra suspicious tissues around the tumor with high fluorescence signal were also sampled for the pathological examination (Figure 3A). The final pathological results confirmed that they were benign tissues with hemorrhage (Figure 3A-E). The mean SBR for these 5 suspicious tissues was 2.19 ± 0.40 (range: 1.95-2.90).
Sampled Tissue Statistics
During the study, 30 breast tumor tissues and 5 suspicious tissues were sampled. Pathological examination confirmed that the tumor tissues were malignant, while the 5 extra bright spots were benign tissues. The statistical analysis of the 35 samples demonstrated that the sensitivity was 0.63 and the positive predictive value was 0.79 by using this MB-based NIR-FI strategies (Table 2).
Total Statistics of Sampled Tissues.a

a N = 35.
Discussion
In this study, we assessed the feasibility of breast tumor identification using MB-based NIR-FI technique on resected human breast tissues during breast surgery. A MB-FI system specially developed for MB excitation and detection was used for imaging. Instead of conventional subcutaneous injection of MB for locating SLN in breast cancer surgeries, 26 MB was intravenously injected 3 hours before surgeries, with the dose of 1 mg/kg of the patient body weight. Thirty patients scheduled for surgeries (28 MRM and 2 BCS) were enrolled to evaluate whether MB could accumulate in breast tumor and be visualized by NIR-FI, as described by Tummers et al study. 25 Tummers et al showed that 20 of 24 breast tumors were detected by NIR-FI method. The histological type of 4 nondetectable tumors were IDC, MUC, DCIS, and primary mucoepidermoid carcinoma, respectively.
In our study, 19 of 30 patients exhibited fluorescent contrast on their resected tissues, which were lower than Tummers et al study. However, we found that preoperative chemotherapy affected the performance of MB-FI. The fluorescence detection rate was 80.0% and 30.0% for patients without and with chemotherapy (P < .05), respectively (Table 1).
Preoperative chemotherapy, also termed as neoadjuvant chemotherapy, is defined as the administration of systemic chemotherapeutic agent prior to downstage tumors and local control of surgery. 27 During this treatment, circulation factors, which caused stimulation of similar tumor growth, were restricted and resulted in proliferation of breast cancer cells substantial reduction. 28 We hypothesize that the preoperative chemotherapy was likely to interfere with the accumulation of MB in tumors by restricting circulation factors, which remarkably reduced the efficacy of MB-FI.
For the 20 patients without chemotherapy, 4 resected tissues did not show sufficient fluorescence contrast. Three of them were confirmed to be IDC, and the other was MUC. We found that the majority (9 of 12) of patients with IDC showed fluorescent signals, but patients with MUC behaved very differently. Besides this nondetectable MUC, we found another patient carried mixed breast carcinoma (Supplementary Figure S1), including MUC, IDC, and ILC. Interestingly, IDC and ILC areas lighted up, whereas the MUC area was dark (Supplementary Figure S1B). Same phenomena of the hardly detectable tumor with MUC histological type were also reported by the previous studies. 25,29
The MB-FI system captured 5 extra bright spots outside tumor areas from the 20 nonchemotherapy patients. However, pathological examinations confirmed that they were all benign tissues with hemorrhage. Therefore, we suspect that such fluorescent bright spots were caused by leakage of MB from blood vessels and retention in the tissue. After statistics of overall imaging results, a sensitivity of 0.63 and a positive predictive value of 0.79 were obtained from this study (Table 2). When we excluded the chemotherapy interferences, 16 tumors from 20 patients were detectable with a mean SBR of 1.94 ± 0.71; thus, the tumor detectable rate of nonpreoperative chemotherapy group is 0.8. These results showed the feasibility of translating MB-FI for breast tumor visualization. With more clinical trials and injection dose studies of MB-FI performed, this technique would have a good potential of benefiting surgical outcomes. As to the mechanism of MB accumulation in breast tumors, it is still confused, which needs further studies to explore.
This preliminary study also revealed some limitations of the MB-FI strategy. First, compared to ICG, MB showed an even less penetration depth due to its shorter wavelength of excitation and emission. For tumors deeper than 1 cm from the skin, it is impossible for the imaging system to detect any fluorescent signal. Therefore, it is more suitable to apply MB-FI during the resection on incisal edges for identifying the residual tumor as well as applying it on resected tissues for selective specimen acquisition in rapid pathological examinations. Second, our home-developed MB-FI system was not fully automated for intraoperative imaging and was not user-friendly enough for surgeons and pathologists, which still needs further improvements.
Conclusions
The MB-based NIR-FI strategy showed a good performance on the ex vivo tumor visualization from patients with breast cancer. It offered a sensitivity of 0.63 and a positive predictive value of 0.79. The effect of MB-FI was adversely influenced by preoperative chemotherapy in this study. More prospective researches are necessary to further explore its clinical values.
Supplemental Material
Supplementary - Methylene Blue–Based Near-Infrared Fluorescence Imaging for Breast Cancer Visualization in Resected Human Tissues
Supplementary for Methylene Blue–Based Near-Infrared Fluorescence Imaging for Breast Cancer Visualization in Resected Human Tissues by Chong Zhang, Daqing Jiang, Bo Huang, Cong Wang, Lin Zhao, Xianxin Xie, Zhaohe Zhang, Kun Wang, Jie Tian and Yahong Luo in Technology in Cancer Research & Treatment
Supplemental Material
Supplemental Material, S_Fig_1 - Methylene Blue–Based Near-Infrared Fluorescence Imaging for Breast Cancer Visualization in Resected Human Tissues
Supplemental Material, S_Fig_1 for Methylene Blue–Based Near-Infrared Fluorescence Imaging for Breast Cancer Visualization in Resected Human Tissues by Chong Zhang, Daqing Jiang, Bo Huang, Cong Wang, Lin Zhao, Xianxin Xie, Zhaohe Zhang, Kun Wang, Jie Tian and Yahong Luo in Technology in Cancer Research & Treatment
Footnotes
Authors’ Note
Chong Zhang, MSc, Daqing Jiang, MMed, and Bo Huang, MD, contributed equally to this work and should be considered as co-first authors.
Acknowledgments
The authors thank Yamin Mao, Kunshan He, and Haiyan Liu for helpful discussion; Weijun and Didi Xie for patient information; and Mo Li and Jie Bai for patients care. The Institutional Review Board of the Cancer Hospital of China Medical University approved this study (approval number, 20171105), and all patients provided written informed consent to be examined in this study. The clinical trial was registered at the Chinese Clinical Trial Registry (![]() , ChiCTR1800015400).
, ChiCTR1800015400).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Ministry of Science and Technology of China under Grant No. 2017YFA0205200 and 2016YFC0103803, the National Natural Science Foundation of China under Grant Nos. 81227901, 81527805, and 61671449, the Chinese Academy of Sciences under Grant No. KFJ-STS-ZDTP-059, YJKYYQ20180048, GJJSTD20170004, and QYZDJ-SSW-JSC005.
Supplemental Material
Supplemental material for this article is available online.
Abbreviations
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.