
Abstract
Introduction:
This research quantifies and compares the effect of hip prostheses on dose distributions calculated using collapsed cone convolution superposition and Monte Carlo (with and without correcting for the density of the implant and surrounding tissues). The use of full volumetric modulated arc therapy arcs versus volumetric modulated arc therapy arcs avoiding the hip implants (skip arcs) was also studied.
Materials and Methods:
Six prostate patients with hip prostheses were included in this study. The hip prostheses and the streaking artifacts on the computed tomography images were contoured by a single physician, and full volumetric modulated arc therapy arcs were created in the Pinnacle3 TPS. Copies of each plan were made, and the doses were recalculated with the densities of the prostheses and surrounding tissues overridden. The plans were then exported to Monaco and recalculated using a Monte Carlo dose calculation algorithm, with and without densities of the prosthesis and surrounding tissues overridden.
Results:
With density overrides, Pinnacle3 had a 4.4% error for ion chamber measurements. Monaco was within 0.2% of ion chamber measurement when density overrides were used. On average, when density overrides were used in Pinnacle3 for patient dose calculations, the planning target volume D95 value dropped from 99.3% to 82.7%. Monaco also showed decreased planning target volume coverage when plans were recalculated with correct density information. Full arc plans (with density overrides) for the patient with a bilateral prosthesis provided significant bladder sparing and some rectal sparing compared to skip arc plans.
Conclusion:
When planning for prostate patients with hip prostheses, correct density information for implants and surrounding tissues should be used to optimize the plan and ensure optimal accuracy. If available, a Monte Carlo algorithm should be used as a second check. Full arcs could be used to spare dose to organs at risk, while maintaining adequate planning target volume coverage, when using a Monte Carlo dose calculation algorithm.
Keywords
Introduction
The Center for Disease Control reported that in 2010, 310 800 total hip replacements were performed among patients aged 45 years and older. 1 In addition, the number of patients receiving total hip replacement has more than doubled since the year 2000. Currently, 1 in 9 men will develop prostate cancer in their lifetime. 2 With these statistics in mind, the number of patients with prostate cancer who have undergone total hip replacement surgery will continue to increase in the future.
External beam radiation therapy (EBRT) is a standard treatment for patients with prostate cancer. Although EBRT is a routine treatment for prostate cancer, patients with unilateral or bilateral metal hip prostheses introduce several challenges that make treatment planning and accurate dose delivery difficult. Numerous studies have demonstrated the difficulties associated with planning and delivering an accurate plan to patients with metal hip prostheses. Some studies have shown that metal artifact reduction techniques aid in increasing image quality and therefore improving structure delineation in the pelvis. 3 –8 Although metal artifact reduction has an important role in the clinic, our work is primarily focused on the dose calculation and treatment techniques used for patients undergoing computed tomography (CT) who are severely affected by streaking artifacts.
Numerous studies have evaluated the performance of various treatment planning systems in the presence of metal hip prosthesis. 9 –15 The collapsed cone convolution superposition (CCCS) dose calculation algorithm utilized by several treatment planning systems is accurate in homogeneous situations. However, when planning in regions near metal hip prostheses, the CCCS algorithm fails to accurately calculate dose. Ade and du Plessis 9 showed errors of up to 23.2% when using the CCCS algorithm in the XiO Treatment Planning System (ELEKTA, Stockholm, Sweden). The Pinnacle Treatment Planning System (Philips, Fitchburg, Wisconsin) also utilizes CCCS for its dose calculation methods. Investigators have reported that the CCCS algorithm in Pinnacle also struggles with accurately calculating dose in the vicinity of a hip prosthesis. 10,11,14 The high density of the prosthesis results in streaking artifacts and incorrect CT number reporting for the prosthesis and the surrounding tissues. All 3 of these studies showed that the CCCS algorithm in Pinnacle overestimates the dose calculated in regions surrounding a metal hip prosthesis. 10,11,14 These studies also investigated the use of density overrides in Pinnacle, and all observed that Pinnacle actually underestimates the dose when the correct physical densities are assigned to the hip prosthesis.
Monte Carlo (MC) methods are regarded as the “gold standard” for patient dose calculations and have become increasingly relevant in the clinic in recent years. Unlike CCCS, MC has been shown to accurately calculate dose in regions near high-density hip prostheses. 9,12 –15 True MC methods (ie, EGSnrc, MCNP, PENELOPE, etc) for patient dose calculations are computationally challenging to implement in the clinic, but some treatment planning systems have developed their own MC algorithms that can easily be used for patient dose calculations without the long computation times associated with true MC methods. Ade and du Plessis 9 studied the Monaco Treatment Planning System (ELEKTA), which uses an MC algorithm, demonstrating that it calculated dose within 4% of the measured dose in the presence of a hip prosthesis. The study showed that the MC algorithm used in Monaco was significantly more accurate than the CCCS algorithm used in XiO.
Because so many studies have demonstrated the uncertainties associated with dose calculation in the presence of metal hip prostheses, the American Association of Physicists in Medicine Task Group 63 recommend that planners avoid orienting the beam through the prosthesis. 16 Although this technique can help to improve the accuracy of the dose calculation, avoiding the hip prosthesis may lead to higher doses in the surrounding organs at risk (OAR), such as the bladder and rectum. Volumetric modulated arc therapy (VMAT) has been shown to be superior to intensity-modulated radiotherapy therapy (IMRT) in providing better target coverage and increased OAR sparing. 17 –19 Rana et al showed that using several “skip arcs” (those that avoid going through the prosthesis) for a patient with a bilateral hip prosthesis was superior to traditional IMRT in terms of producing better plan conformity and lower bladder and rectum doses. All published studies investigating the use of VMAT for patients with prostate cancer with hip prosthesis have used skip arcs, and none have addressed the potential of using full VMAT arcs when a robust and accurate treatment planning system is available.
The objective of our study is to compare the abilities of the CCCS algorithm in Pinnacle Treatment Planning System and the MC algorithm in the Monaco Treatment Planning System to accurately calculate patient dose in the presence of metallic hip prostheses. The use of density overrides for the prosthesis and surrounding tissues was studied for both treatment planning systems. In addition, we aimed to test the viability of using full VMAT arcs instead of the traditionally used skip arcs to try and achieve lower doses to surrounding OAR.
Materials and Methods
Measurements With Hip Prosthesis
The MC algorithm in Monaco was previously validated for both homogeneous and inhomogeneous settings. Both treatment planning systems, Pinnacle and Monaco, utilized the same commissioning beam data. A phantom for measurements was created by placing a titanium alloy (TMZF) hip prosthesis (Stryker, Kalamazoo, Missouri) within slabs of bolus, as seen in Figure 1. A plan was created in Pinnacle using a 6 cm × 6 cm field with a 6 MV lateral beam (oriented through the prosthesis) and a dose of 400 cGy assigned to the isocenter, which was placed at the chamber center. Extra care was taken during the setup of the phantom and position as well as the absence of air pockets were verified using kV imaging. The positioning was verified by comparison against the simulation scan. The dose was calculated using the CCCS dose calculation algorithm in Pinnacle, without correcting for the densities of the prosthesis and bolus. The plan was then copied, and the prosthesis and streaking artifacts were contoured. The physical density of the prosthesis was overridden to 5 g/cm3 and the physical density of the bolus was overridden to 1 g/cm3. The exact composition of the TMZF alloy used in the prosthesis is proprietary information, so 5 g/cm3 was chosen as a reasonable estimation for the physical density. 20 Small deviation from this value should not have a significant impact on the dose calculation. The plan was then recalculated in Pinnacle using the same number of monitor units as in the plan without density overrides.

Experimental setup with hip prosthesis placed within slabs of bolus. The top pictures show the simulation computed tomography before (left) and after (right) density overrides were applied. An ion chamber was placed at isocenter with a lateral 6 MV photon beam oriented through the prosthesis.
Both plans (with and without density overrides) were transferred to the Monaco Treatment Planning System and the dose to the chamber was recalculated using the MC algorithm. In Monaco, the electron density relative to water is overridden unlike the physical density in Pinnacle. For the prosthesis, the relative electron density when compared to water was calculated to be 3.7, which is the relative electron density of titanium.
The plan created in Pinnacle (6 cm × 6 cm field, 400 cGy assigned to the chamber center) was delivered to the phantom. Measurements were taken with a 0.3 cm3 Semiflex 3-dimensional ion chamber (PTW, Freiburg, Germany) and the plan delivery was repeated 5 times. The average of the 5 readings was compared to the doses calculated in the chamber volume across the 4 plans.
Comparison Patient Dose Calculations in Pinnacle and Monaco
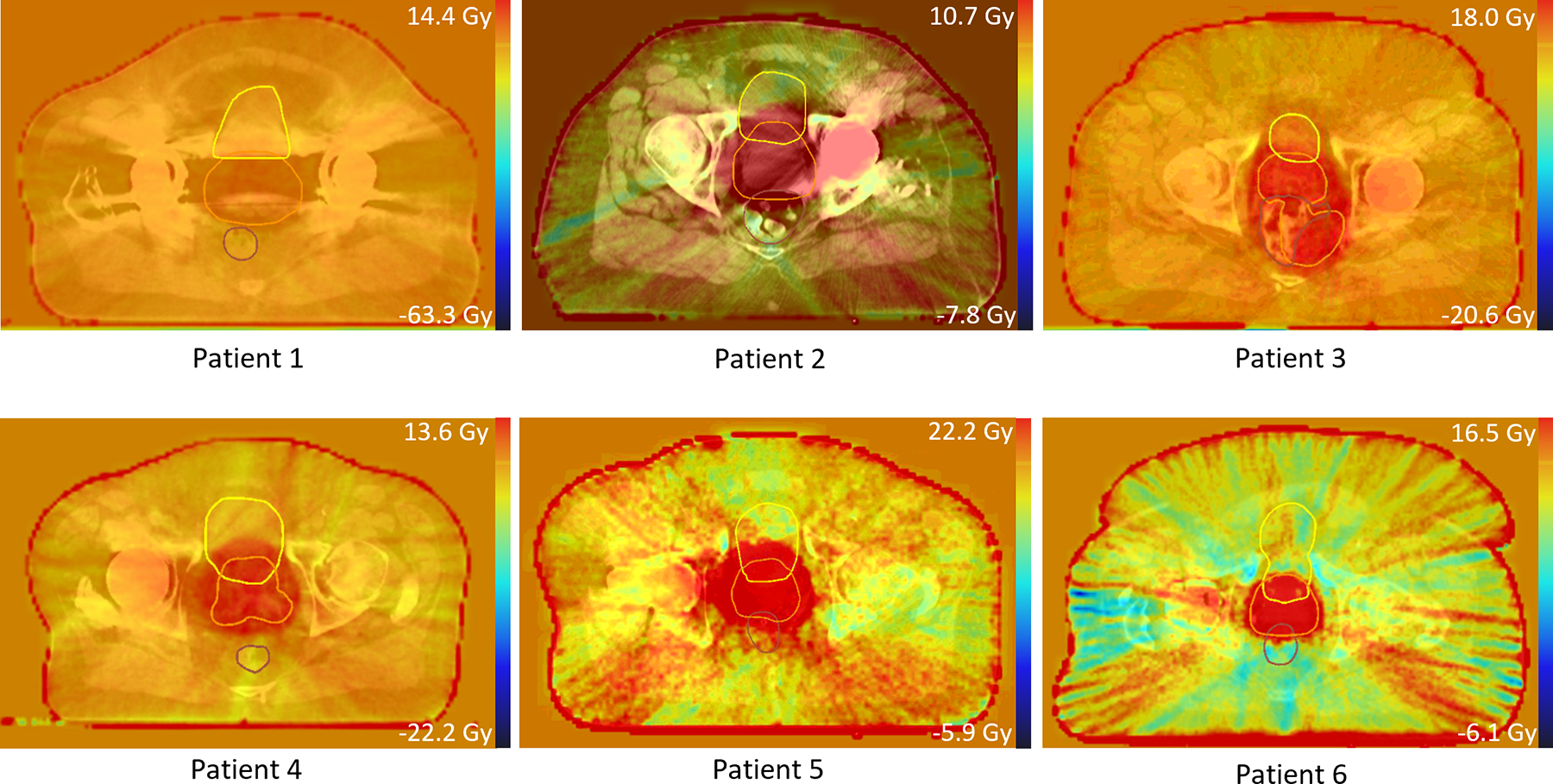
Six previously treated patients with prostate cancer with hip prostheses were chosen for this study. Figure 2 displays the most severely affected slice in Pinnacle, with the planning target volume (PTV) in orange, the bladder in yellow, and the rectum in brown. Patient 1 has a bilateral hip prosthesis, while patients 2 through 6 each have a unilateral prosthesis. The Window/Level option in Pinnacle was set to the “Bone” preset (Window = 1401, Level = 700) to improve the visualization of the prosthesis in each CT. The prosthesis was then carefully contoured in each slice. The Window/Level setting was then returned to the “Abdomen” preset (Window = 401, Level = 800), and the tissues surrounding the prosthesis that were affected by streaking artifacts were then contoured. Initially, the physical densities for the prosthesis and surrounding tissues were not overridden. For each patient, a plan utilizing full VMAT arcs was created with a dose of 7800 cGy over 39 fractions assigned to the PTV. Plans were optimized to ensure 95% of the prescribed dose covered at least 95% of the PTV volume and to meet the OAR dose constraints established by QUANTEC. 21,22 All dose calculations in Pinnacle were performed using 0.3 cm × 0.3 cm × 0.3 cm grid spacing. Copies of these plans were made, and the doses were recalculated with the densities of the prosthesis and surrounding tissues overridden (5 and 1 g/cm3, respectively). The plans were then exported to the Monaco Treatment Planning System and recalculated using an MC dose calculation algorithm. The relative electron density to water of each patient’s prosthesis was overridden to 4.5 in Monaco, and surrounding tissues were overridden to 1.0. Metallic hip prosthetics are commonly made from titanium (relative electron density of 3.7), chromium (relative electron density of 6.0), or cobalt (relative electron density of 7.3). The relative electron density for each patient’s prosthesis was chosen to be 4.5 as a reasonable estimate because the composition of each patient’s prosthesis is unknown. Dose calculations in Monaco were performed using 0.3 cm × 0.3 cm × 0.3 cm grid spacing and a statistical uncertainty of 0.70%. Each patient’s plans were exported to VelocityAI (Varian, Palo Alto, California) for further analysis and comparison.

The most severely affected computed tomography slice for each patient. Patient 1 has a bilateral prosthesis, while all other patients have unilateral prostheses. Regions in orange are the planning target volume, regions in yellow are the bladder, and regions in brown are the rectum.
Using Full VMAT Arcs Versus Skip Arcs
Two patients (one with a bilateral prosthesis, patient 1, and one with a unilateral prosthesis, patient 6) were selected for evaluating the use of full VMAT arcs versus the traditionally used skip arcs. For each patient, the first plan created in Pinnacle (using 2 full arcs) was reoptimized with the densities of the prosthesis and surrounding tissues overridden. A second plan was created using the skip arc that avoided going through the prosthesis. The skip arc plans were also optimized with the densities of the prosthesis and surrounding tissues overridden. Both sets of plans were transferred to Monaco and recalculated using an MC algorithm, with the correct relative electron densities assigned to the prosthesis and tissues. The plans were exported to VelocityAI for further analysis. The tumor control probability (TCP) and normal tissue complication probability (NTCP) were calculated using an application previously developed at our institution to determine which plan would have the greatest therapeutic benefit. 23 The parameters used for calculating the TCP and NTCP values can be seen in Table 1, which were repeated from the work of Mavroidis et al. 24
Summary of Parameters Used to Calculate TCP and NTCP Values.a

Abbreviation: NTCP, normal tissue complication probability; TCP, tumor control probability; PTV, planning target volume.
a D50 is the dose that is associated with the 50% response rate, γ is the maximum normalized value of the dose–response gradient, and s is the relative seriality parameter. 25
Results
Measurements
Table 2 displays the results from the measurements taken with the hip prosthesis in the bolus phantom. When density overrides were not used, Pinnacle had an error of 9.2% for correctly calculating the dose to the chamber. Employing density overrides gave a slight improvement in the dose calculation in Pinnacle and brought the error down to 4.4%. Even without using the relative electron density overrides, Monaco, utilizing the MC dose calculation, was able to calculate the dose to the chamber within 3.6% error. However, when the relative electron densities of the prosthesis and bolus were overridden, Monaco’s MC algorithm showed excellent agreement with the ion chamber measurements and had only 0.2% error.
Results of Ion Chamber Measurements From Bolus Phantom Containing Hip Prosthesis.

Abbreviation: W, with.
Patient Dose Calculations in Pinnacle and Monaco
Figure 3 illustrates the difference in dose between the Pinnacle plan with density overrides and the Pinnacle plan without overrides (ie, corrected Pinnacle plan dose minus uncorrected Pinnacle plan dose) for the same slices shown in Figure 2. Darker areas represent a decrease in dose when the physical densities of the prosthesis and surrounding tissues were overridden, whereas brighter areas reflect increased dose. Similarly, Figure 4 shows the same slices and corresponding dose differences when the uncorrected Monaco plan dose was subtracted from the corrected Monaco plan dose. Similarly to the plans generated by Pinnacle, there were generally cold spots arising in the PTV when electron densities were overridden in Monaco. Figure 5 displays the dose distribution when the corrected Pinnacle plan dose was subtracted from the corrected Monaco plan dose. When the 2 treatment planning systems were compared using their respective dose calculation algorithms (ie, CCCS for Pinnacle and MC for Monaco), there an obvious increase in PTV dose when plans were recalculated using the MC algorithm in Monaco, meaning that the CCCS algorithm in Pinnacle underestimated the dose.

Dose distributions generated in VelocityAI showing the difference in dose between the Pinnacle plan with density overrides and the Pinnacle plan without overrides (ie, corrected Pinnacle plan dose minus uncorrected Pinnacle plan dose). The slices shown in are the same as those shown in Figure 2. All plans utilized 2 full VMAT arcs and did not avoid entry or exit through the prosthesis. A color bar scale is provided to show the relative variation in dose across both plans for each patient. Negative values indicate a decrease in dose from one plan to another. Doses to the PTV generally appear to decrease for each patient when physical densities are overridden. PTV indicates planning target volume; VMAT, volumetric modulated arc therapy.

Dose distributions generated in VelocityAI showing the difference in dose between the plans calculated in Monaco (ie, corrected Monaco plan dose minus uncorrected Monaco dose). The slices shown are the same as those shown in Figure 2. These plans were optimized in Pinnacle and recalculated in Monaco. A color bar scale is provided to show the relative variation in dose across both plans for each patient. Negative values indicate a decrease in dose from one plan to another. Doses to the planning target volume generally appear to decrease for each patient when electron densities are overridden.
Dose distributions generated in VelocityAI showing the difference in dose between the plans calculated in Monaco and Pinnacle, both with density overrides (ie, corrected Monaco plan dose minus corrected Pinnacle dose). A color bar scale is provided to show the relative variation in dose across both plans for each patient. Negative values indicate a decrease in dose from one plan to another. When densities of the prosthesis and surrounding tissues are overridden, Pinnacle tends to underestimate dose when compared to the density-corrected Monaco plans.
While dose distributions provide visualization of changes in dose between plans, dose–volume data are needed to conclusively determine whether the changes in dose are clinically significant. Table 3 displays the PTV D95 values (ie, the percentage of the prescription dose that covers at least 95% of the PTV). When density overrides were applied within Pinnacle, 5 of the 6 patients saw a decrease in PTV coverage, with 4 of the plans becoming clinically unacceptable. However, when plans were recalculated in Monaco with the electron densities overridden, all but one patient (patient 1) maintained acceptable coverage, with at least 95% of the PTV receiving 95% of the prescribed dose. The averages across all patients for all 4 plan scenarios are shown as well. Even with density overrides, the CCCS algorithm tends to underestimate dose to the PTV when compared to MC.
Percentage of PTV Volume Receiving at Least 95% of the Prescription Dose for All Patients and Across All Plans.

Abbreviation: PTV, planning target volume; W, with.
Full VMAT Arcs Versus Skip Arcs
Figure 6 shows dose volume histograms for the bladder, rectum, and PTV from patient 1 when full VMAT arcs were compared to skip arc VMAT plans in both Pinnacle and Monaco. The changes in dose volume histograms for patient 6 were minor, so they were not included. The relevant dose–volume information for OAR and PTV from all four plans from both patients can be seen in Table 4. As previously mentioned, correct density information was used to optimize the plans in Pinnacle, and there is generally reasonable agreement (within 4%) between both systems for both types of plans (full arc and skip arc). When full arcs were used, PTV coverage remained acceptable, with over 95% of the target volume receiving at least 95% of the prescription dose. For the patient with bilateral prosthesis, OAR sparing was generally increased when full arcs were used. In particular, the bladder was largely spared when full arcs were used, as opposed to skip arcs.
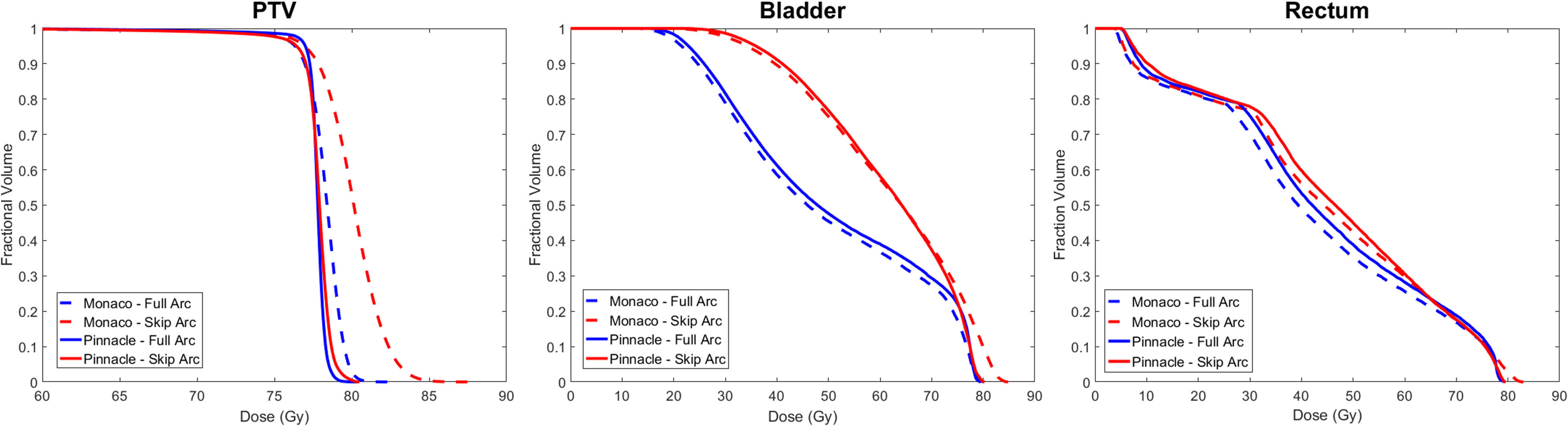
Dose volume histograms for the patient with the bilateral prosthesis for the planning target volume, bladder, and rectum. Lines in blue represent full arc plans and skip arcs plans are represented by red lines. Dashed lines represent plans calculated in Monaco and solid lines represent plans calculated in Pinnacle.
Relevant Dose–Volume Information for OAR and PTV From All Four Plans From Patient 1 (Bilateral Prosthesis) and Patient 6 (Unilateral Prosthesis).

Abbreviation: PTV, planning target volume.
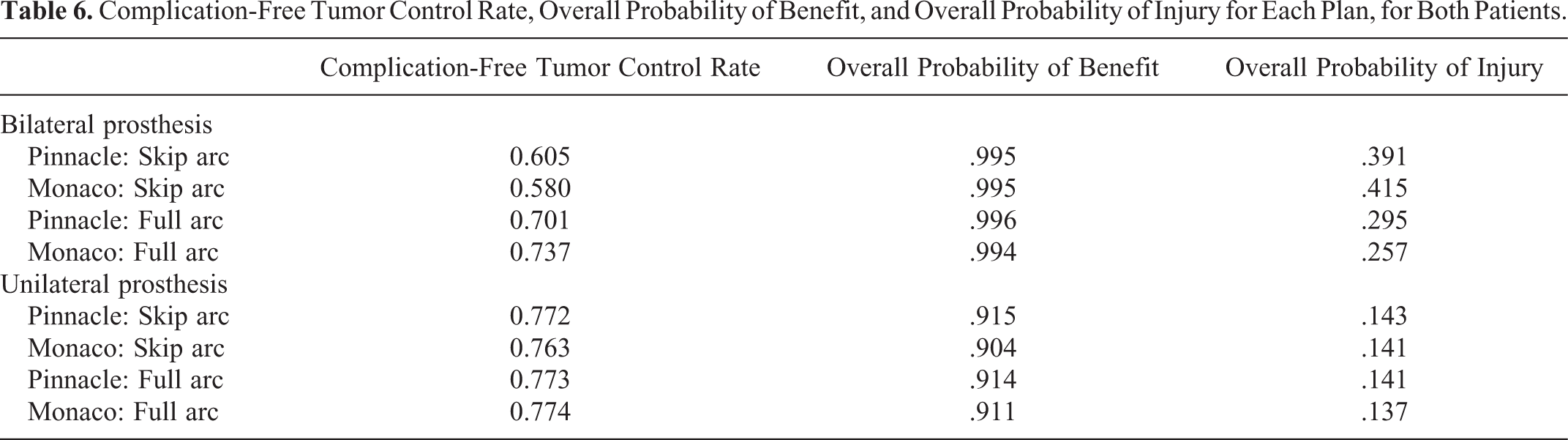
The results from TCP calculations for PTV and NTCP calculations for the bladder, rectum, and femoral head (for the patient with unilateral prosthesis) can be seen in Table 5. There was no significant difference between plans in terms of tumor control. The full arc plans demonstrated a significant improvement in the NTCP for bladder versus the skip arc for the patient with bilateral prosthesis. For the latter plans, the NTCP values for Pinnacle and Monaco, respectively, were 26.0% and 28.9%, whereas for the full arc plans, the NTCP values were 13.9% and 12.2%, respectively. The Monaco full arc plan generated minimal improvement for the rectum with an NTCP value of 15.4% versus the Monaco skip arc NTCP value of 17.8%. The full arcs plans saw little improvement from the skip arc plans for the patient with a unilateral prosthesis. Table 6 displays the complication-free tumor control rate for each plan. The complication-free tumor control rate is derived from the probability of benefit, which is the overall TCP, and the probability of injury, which is the overall normal tissue complication rate. The full arc plans demonstrated superior complication-free tumor control rates of 70.1% and 73.7% (Pinnacle and Monaco, respectively), while the skip arc plans had the considerably lower values of 60.5% and 58.0% (Pinnacle and Monaco, respectively) for the patient with bilateral prosthesis. Overall, the full arc plans were superior in both complication-free tumor control and risk for normal tissue injury for the patient with bilateral prosthesis, while the patient with unilateral prosthesis saw little gain or loss in plan quality.
Results From TCP Calculations for PTV and NTCP Calculations for the Bladder, Rectum, and Femoral Head (for the Patient With Unilateral Prosthesis).

Abbreviations: NTCP, normal tissue complication probability; PTV, planning target volume; TCP, tumor control probability.
Complication-Free Tumor Control Rate, Overall Probability of Benefit, and Overall Probability of Injury for Each Plan, for Both Patients.
Discussion
Various studies have shown that the CCCS dose calculation algorithm often fails at calculating dose accurately in inhomogeneous geometries. 9 –11,14 Conversely, MC has consistently proven to be an accurate dose calculation algorithm in both homogeneous and inhomogeneous situations, particularly for patients with high-density implants. 9,12 –15 Our measurements with the hip prosthesis in the bolus phantom agree with previous studies as errors in Pinnacle approached 10% when density overrides were not used. Even with the densities of the bolus and prosthesis overridden in Pinnacle, the CCCS algorithm was only able to calculate the dose to the chamber within 4.4% accuracy. Our results agree with the study conducted by Ade and du Plessis, which demonstrated a 4% error in the Monaco Treatment Planning System. However, this study did not discuss the use of electron density overrides in Monaco. Our results showed high accuracy in calculating dose to the chamber (within 0.2%) when the electron densities were overridden to the appropriate values.
When patient dose calculations were performed, a similar trend was observed in the PTV coverage for the majority of patient plans. Patient 1 was the major outlier among all patient plans and saw the biggest decrease in PTV dose when plans were recalculated likely because this patient had a bilateral prosthesis. When doses were recalculated (not reoptimized) with physical density overrides in Pinnacle, the CCCS algorithm generally underestimated the PTV dose when compared to the Monaco plans with electron density overrides. The CCCS algorithm in Pinnacle assumes the non-air voxels to be water of varying physical density. When the density override feature in Pinnacle is used, the algorithm does not consider variations in composition and only calculates the dose to the density-scaled water. In Monaco, the user has the ability to override the electron density of a region, rather than the physical density. Rijken and Colyer 10 attribute the underestimation of dose in the algorithm to the fact that it does not take into account the difference in the total mass attenuation coefficient between water and the metal in question. At the nominal energy for a 6 MV photon beam, the total mass attenuation coefficient for titanium is slightly lower than that of water. 25 Because Pinnacle assumes the structures to be density-scaled water, rather than an entirely different medium with a higher Z, the CCCS algorithm will underestimate the dose.
When the full arc plans for patient 1 (bilateral prosthesis) and patient 6 (unilateral prosthesis) were optimized with the correct physical densities in Pinnacle, the plans showed good agreement with the recalculated plans in Monaco. The difference in PTV coverage between the full arc plans (in both Pinnacle and Monaco) and the skip arc plans was essentially negligible. However, for the patient with a bilateral prosthesis, there was a considerable difference in OAR sparing when full arc plans were used in comparison with skip arcs plans. Bladder sparing significantly improved with the use of full arc plans, particularly for the V50 and V65 values. Although not as drastic, the rectum sparing also improved when full arcs were used. There was little significant change in dose–volume metrics between the full arc and skip arc plans for the patient with a unilateral prosthesis. The NTCP calculations were used to assess the clinical significance of improved OAR sparing from using full arcs. Regarding TCP, the difference between the skip arc and full arc plans was negligible. For patient 1 (bilateral prosthesis), the Monaco full arcs plan showed a slight improvement in the rectum normal tumor complication probability; however, the difference between the 4 plans was small. The risk of injury to the bladder significantly decreased when full arc plans were used. For patient 6 (unilateral prosthesis), there was little change in overall probability of benefit or injury when comparing full arcs versus skip arcs. Our results show that, for patients with a bilateral hip prosthesis, full arc VMAT plans are the best choice to ensure a better complication-free tumor control rate.
Previous studies that have shown the usefulness of VMAT has recommended that the beam avoid entering the prosthesis. 18,19 Avoiding beam entry through the prosthesis can place an unnecessary amount of dose into the bladder and rectum, particularly for patients with a bilateral prosthesis. With an accurate dose calculation method, such as MC, a planner could potentially create accurate full arcs plans that do not avoid the prosthesis and provide increased sparing to sensitive OAR. The results of our study are 3-fold. First, planners should always use the actual densities for the prosthesis and surrounding tissues, whether physical density (as in Pinnacle) or electron density (as in Monaco), when optimizing plans to ensure accuracy. Furthermore, an accurate dose calculation method, such as MC, should be used if available. This method can serve as a second check to ensure that plans are produced with acceptable accuracy. Finally, if an accurate dose calculation method is available, planners can use full VMAT arcs, without avoiding the prosthesis, for patients with a bilateral prosthesis to improve OAR sparing (particularly for the bladder) without sacrificing PTV coverage. Full VMAT arcs have the potential to decrease the risk of injury to healthy tissues without diminishing the probability of effectively controlling the tumor.
Conclusions
This study quantifies and compares the CCCS algorithm used in Pinnacle with the MC algorithm used in Monaco for patients with prostate cancer with hip prostheses. Measurements were taken in a phantom made from bolus containing a hip prosthesis using an ion chamber. Without overriding the physical densities, the CCCS algorithm in Pinnacle demonstrated a significant 9.2% error in calculating dose. Overriding the physical densities of the prosthesis resulted in improvement of the calculated dose with 4.4% error in Pinnacle. Monaco’s MC algorithm showed a 3.6% error when the electron densities of the prosthesis and bolus were not overridden decreasing to 0.2% when the electron densities were overridden to the correct values. We compared the use of density overrides for dose calculation within both systems for 6 patients (1 of these patients had a bilateral prosthesis). The PTV coverage decreased significantly when plans were recalculated (but not reoptimized) with correct physical densities in Pinnacle. Monaco showed a similar trend—PTV coverage decreased when the plans were recalculated with the correct electron densities. However, in 5 of the 6 patients, the CCCS algorithm in Pinnacle underestimated the dose when compared to the Monaco MC algorithm when density overrides were applied in both systems. We investigated the use of full VMAT arc plans, instead of the traditionally used skip arc plans that avoid entry through the prosthesis. For 2 patients, one with a bilateral prosthesis and one with a unilateral prosthesis, both TCP and NTCP calculations were performed to investigate the radiobiological impact in using full arcs versus skip arcs. The results of these calculations demonstrated that, for patients with a bilateral prosthesis, full VMAT arcs can significantly decrease the risk of injury to normal tissue (particularly the bladder) while simultaneously maintaining adequate tumor control.
The findings of this study illustrate the importance of utilizing accurate density information for the prosthesis and surrounding tissues when optimizing treatment plans. Monte Carlo dose calculations should be performed as a second check to ensure accuracy. Finally, if an accurate method of dose calculation is available, planners can use full VMAT arcs instead of arcs that avoid the prosthesis to improve OAR sparing and maintain adequate PTV coverage, particularly for patients with a bilateral prosthesis.
Footnotes
Authors’ Note
An ethics statement regarding animal/human studies is not applicable.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The project described was supported by the National Center for Advancing Translational Sciences, National Institutes of Health, through Grant TL1 TR002647. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH. This project was also supported by the Cancer Prevention and Research Institute of Texas (CPRIT) Research Training Award (RP170345). .