
Abstract
Objective:
To evaluate the efficacy and safety of hypofractionated stereotactic radiotherapy using CyberKnife for high volume cavernous sinus cavernous hemangiomas.
Materials and Methods:
We collected data from 12 patients with high volume cavernous sinus cavernous hemangiomas treated with hypofractionated stereotactic radiotherapy using CyberKnife in our institute, including 2 men and 10 women/female child, aged 4 to 60 years. Initial tumor volumes ranged from 11.8 to 96.6 cm3 with a median of 24.3 cm3. Irradiation doses were 19.5 Gy with 3 fractions in 2 patients, 21 Gy with 3 fractions in 8 patients, 25 Gy with 5 fractions in 1 patient, and 30 Gy with 3 fractions in 1 patient. We used 109 to 155 beams during treatment, and target volumes reached over 95% of the prescribed dose. Follow-up ranged from 3 to 54 months. We evaluated the efficacy and safety of the CyberKnife system based on changes in the diagnostic images and involved cranial nerves or symptoms.
Results:
Of the 12 patients, 11 were followed for 3 to 54 months with a mean follow-up of 16.3 months; 1 patient was lost to in-person follow-up. Lesion volumes in the followed 11 patients were calculated after fractionated radiotherapy. All tumor volumes decreased (28.6%-94.1%) and symptoms improved (including blurred vision, visual field defects, diplopia, headaches, and facial numbness) after therapy. Postoperative magnetic resonance images revealed a tumor volume range of 2.8 to 41.0 cm3 (median, 6.5 cm3), significantly lower compared with the pretreatment range of 11.8 to 70.1 cm3 (median, 24.3 cm3; T = 0.00, P = .003 < .05). A single patient experienced radiotherapy-related cerebral edema, which resolved after 5 days of mannitol and dexamethasone.
Conclusions:
Based on the current results, though preliminary, hypofractionated stereotactic radiotherapy using CyberKnife is an effective and safe alternative for high volume cavernous sinus cavernous hemangiomas and is the recommended primary treatment in high-risk patients with this condition.
Keywords
Introduction
Cavernous sinus cavernous hemangioma (CSCH) is a rare extra-axial vascular neoplasm that accounts for 2% to 3% of all cavernous sinus (CS) tumors. 1 Cavernous sinus cavernous hemangiomas differ from other intra-axial cavernous malformations in the brain as they represent true vascular neoplasms, and the associated symptoms result from progressive tumor growth and mass effects. 2 The optimal treatment strategy remains controversial, especially for high volume CSCHs. Most patients with mild neurological dysfunction or nonspecific symptoms are diagnosed incidentally on computed tomography (CT) or magnetic resonance imaging (MRI); therefore, the clinical detection rate is low. Different treatments are based on tumor size, location, and relationship with the surrounding tissue. A microsurgical approach may result in severe bleeding and even operative death, 3 whereas total removal rates by surgical excision are only 30% to 44%. 4 CyberKnife (Accuray, Sunnyvale, California) as a new device permits fractionated stereotactic radiotherapy (SRT) for intracranial lesions. Used with real-time imaging, the CyberKnife system can deliver a maximum radiation dose directly to the tumor from different angles with submillimeter precision and is considered quite accurate. In this study, we evaluated the safety and efficacy of fractionated SRT using the CyberKnife system in 12 patients with high volume CSCHs treated between 2012 and 2017 in our institute.
Materials and Methods
We enrolled 12 patients with high volume CSCHs between 2012 and 2017 in our institute. Written informed consent was obtained from each participant prior to study inclusion, and the study was approved by the local ethics committee of the Chinese People’s Liberation Army General Hospital (No. S2018-119-01). Patients’ diagnoses were based mainly on MRI findings, and 2 patients’ diagnoses were also confirmed by histopathology after surgical resection. Patient inclusion criteria were tumor volume >20 cm3 or the longest diameter >4 cm. We enrolled 10 female/female child and 2 male/male child patients with a median age of 44 years (range, 4-60 years) at diagnosis. Patients’ main symptoms included blurred vision (n = 6), visual field defects (n = 3), diplopia (n = 2), facial numbness (n = 2), tinnitus (n = 1), headache (n = 6), dizziness (n = 3), epilepsy (n =1), limb weakness (n = 2), and unsteady gait (n = 1; Table 1). All patients underwent pretreatment CT (Siemens, Forchheim, Germany) and MRI (Siemens, Erlangan, Germany), and findings confirmed high volume CSCH. Computed tomography images showed slightly increased intensity with rare calcification. T2WI-weighted and fluid-attenuated inversion recovery sequences showed ultrahigh and uniform signals using enhanced sequences. We also saw areas of relative hypoperfusion on 3-dimensional arterial spin labelling imaging. No patients had preoperative embolization, and all underwent fractionated SRT.
Clinical Data and Post-CyberKnife Follow-Up of Patients With CSCH.
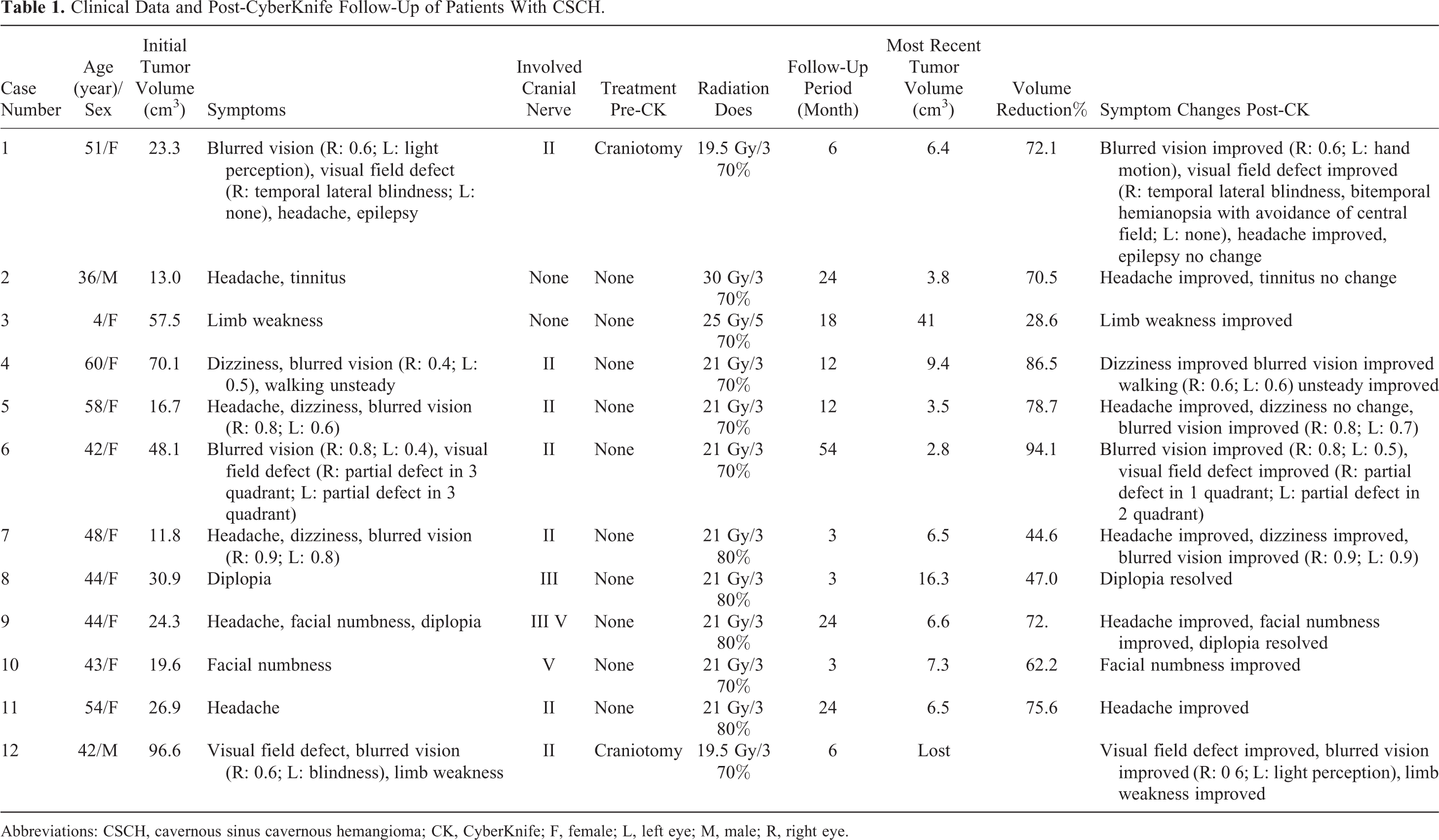
Abbreviations: CSCH, cavernous sinus cavernous hemangioma; CK, CyberKnife; F, female; L, left eye; M, male; R, right eye.
The CT scan specifications were tube voltage: 120 kV, tube current: 320 mAs, slice thickness: 1 mm, field of view: 260 mm, and matrix size: 512 × 512. The MRI scanning parameters were T1WI: TR1650/TE3 milliseconds, slice thickness: 1.0 mm; and T2WI: TR5500/TE93 milliseconds, slice thickness: 1.0 mm. Rigid fusion registration for the MRI T1WI enhancement sequence and CT scans was performed using the image processing software, MIM Maestro version 6.5.4 (MIM software Inc, Cleveland, Ohio). The prescribed dose was defined as 70% to 80% of the maximal dose for the planning target volume. Irradiation doses received by the lesions were 19.5 Gy/3F in 2 patients, 21 Gy/3F in 8 patients, 25 Gy/5F in 1 patient, and 30 Gy/3F in 1 patient. We used 109 to 155 radiation beams, and the prescribed isodose covered at least 95% of the planned target volume. Patients were followed as outpatients to evaluate clinical symptoms and imaging changes. One patient was lost to in-person follow-up for MRI imaging but was available by telephone.
We measured tumor dimensions using the Coniglobus formula: V = 1/6π ×a (diameter length) × b (diameter width) × m (slice thickness) × c (slice number). We used SPSS version 17.0 (SPSS Inc, Chicago, Illinois) for statistical analyses and the Wilcoxon paired t test to analysis the data of volume changes. Value of P < .05 was considered significant.
Results
Eleven patients underwent MRI follow-up after treatment. One patient was lost to in-person evaluation but was available by telephone. Follow-up ranged from 3 to 54 months (mean, 16.3 months). The initial tumor volume was 11.8 to 96.6 cm3 in all 12 patients. Excluding the data from the patient who did not undergo MRI follow-up, the pretreatment tumor size range was 11.8 to 70.1 cm3. Lesions decreased in size by 28.6% to 94.1% compared with pretreatment. We evaluated patients’ postoperative symptoms during follow-up, and findings are shown in Table 1. Symptoms resolved completely in 1 (8.3%) patient, and improved in 11 (91.6%) patients. Figure 1 shows the changes of visual field of patient 11 after treatment. A single patient experienced radiotherapy-related cerebral edema with symptoms of headache, nausea, and vomiting, which resolved after 5 days of mannitol and dexamethasone treatment. We saw no new neurological deficits in the remaining patients. Tumor control was achieved in 11 patients during follow-up, which was also confirmed by analyzing the volume data. Postoperative MRI in 11 patients revealed posttreatment tumor volumes of 2.8 to 41.0 cm3 (median, 6.5 cm3), which was significantly lower than the pretreatment volumes (P value, only .003), and a decrease of 28.6% to 94.1% (median, 72.1%). Figures 1 and 2 describe findings in 2 typical patients. Figure 3 shows patients’ tumor volume change during follow-up. Table 2 shows the summary of the radiation parameters in treatment plans.
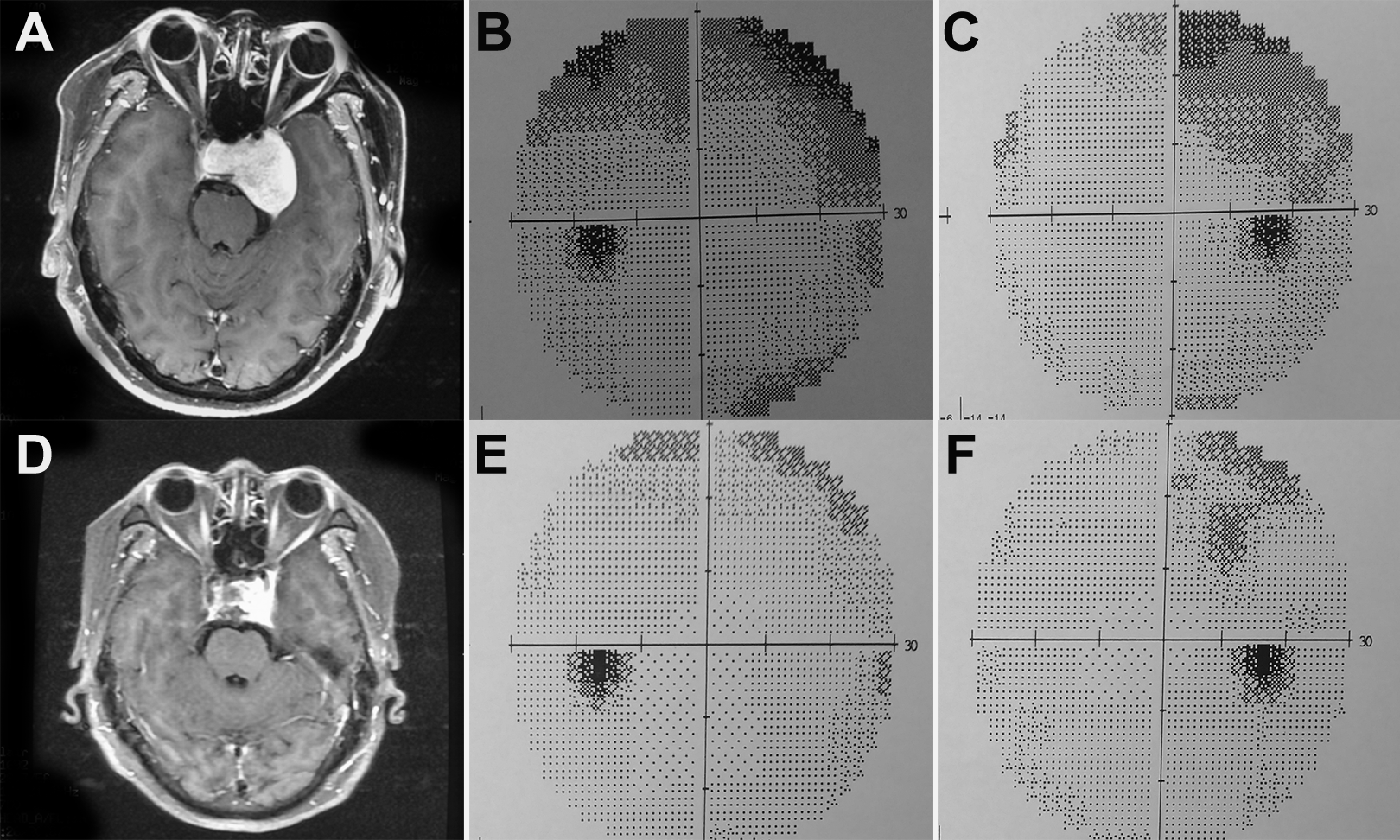
Findings in patient 11. Magnetic resonance images of patient 11 showing a cavernous sinus cavernous hemangioma on the left side. This patient was a 54-year-old woman whose only symptom was headache. A, Axial T1-weighted contrast-enhanced images showing strong enhancement and a pretreatment tumor volume of 26.93 cm3. B, The visual field in her left eye pretreatment. C, The visual field in her right eye pretreatment. D, Axial T1-weighted contrast-enhanced image 24 months after treatment showing that the tumor volume decreased to 6.55 cm3, and that her visual field deficit had improved. E, The visual field in her left eye 24 months after treatment. F, The visual field in her right eye 24 months after treatment.

Findings in patient 4. Magnetic resonance images of patient 4 showing a cavernous sinus cavernous hemangioma on the right side. This patient was a 60-year-old woman who experienced dizziness, blurred vision, and unsteady gait. A, Axial T1-weighted image showing a low-signal intensity lesion. B, Axial T2-weighted image showing a high-signal intensity lesion. C, Axial T1-weighted contrast-enhanced image showing strong enhancement. D, Coronal T1-weighted contrast-enhanced image showing a pretreatment tumor volume of 70.11 cm3. E, Axial T1-weighted contrast-enhanced image 6 months after treatment. F, Coronal T1-weighted contrast-enhanced image showing a decreased posttreatment tumor volume of 9.45 cm3. The patient’s clinical symptoms had also improved.

Patients’ tumor volume changes during follow-up.
Summary of the Radiation Parameters in Treatment Plans.
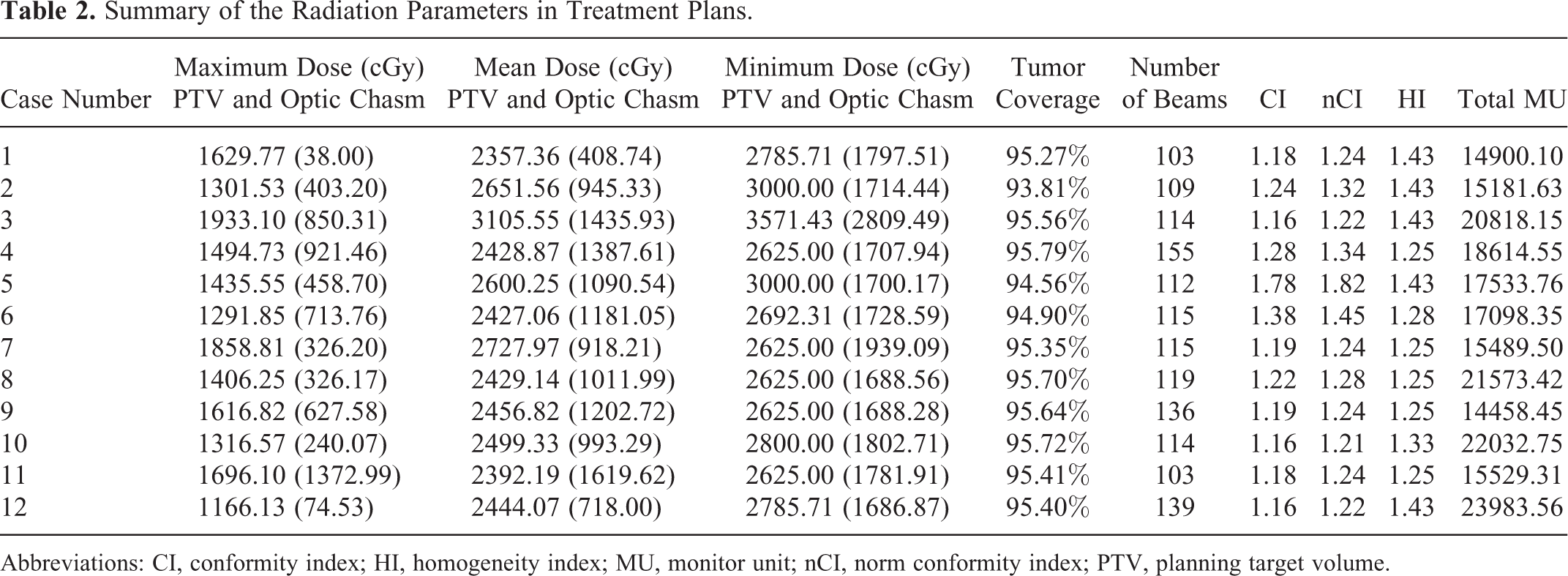
Abbreviations: CI, conformity index; HI, homogeneity index; MU, monitor unit; nCI, norm conformity index; PTV, planning target volume.
Discussion
Cavernous sinus cavernous hemangioma is a rare extra-axial vascular tumor derived from vascular malformations that is seen most commonly in middle-aged women. 4 Of the 12 patients, 10 were women in this study. The cavernous sinus region is filled with nerves and blood vessels. The inherent highly vascular nature of CSCHs and their proximity to crucial cranial nerves and the intracavernous portion of the internal carotid artery make them difficult tumors to resect surgically. 2 Traditional surgical resection may cause intracranial nerve dysfunction and massive hemorrhage, and complete CSCHs resection is challenging because of cranial nerve involvement and severe bleeding. Fraser et al reported that the short-term complication rates after craniotomy were as high as 72% and were related predominantly to cranial nerve deficits, compared with 22% after radiosurgery 5 ; the long-term morbidity rate was 20%. 5 Surgical mortality and morbidity rates of 36% to 38% have been reported. 6
Because of the high mortality and morbidity rates associated with surgery, if complete surgical resection cannot be accomplished, radiotherapy should be considered. Conventional radiotherapy was reported for treating CSCHs in previous studies; however, most of the relevant studies were case reports. 7 –10 The tumors decreased significantly in size, and neurological symptoms improved with a radiation dose of 30 to 50 Gy in these studies. However, data on complications are not comparable with our data because these studies provided limited clinical data on definitive fractionated radiotherapy. One case report also showed that fractionated treatment with 40 Gy induced endothelial cell damage and fibrosis within CSCH lesions. 11 In 2007, Park et al summarized the clinical results of 10 patients with high volume CSCHs (mean, 34.1 cm3) who received definitive fractionated radiotherapy with a total dose of 50 to 54 Gy. The study showed a tumor volume reduction of 72.9% (range, 18.9%-95.3%) at a median follow-up of 6.8 years, and all 10 of the cranial neuropathies observed before radiation therapy had improved, with complete symptomatic remission in 9 (90%) patients and partial remission in 1 (10%) patient. The long-term results of the study appear better than ours, possibly because of the higher equivalent doses and longer follow-up period. Peng Li et al reported gamma knife radiosurgery (GKS) for high volume CSCHs (mean 30.4 cm3) of 16 patients with a tumor volume reduction of 59.55% (11.6%-100%) and symptoms completely resolved in 25% of patients at a mean follow-up of 21.5 months. The results also seem poor than conventional radiotherapy with a shorter follow-up time. So these previous studies substantiated the role of fractionated radiotherapy in treating CSCHs, which should not be ignored despite the disadvantages of longer treatment periods.
In 1999, Iwai et al first reported favorable outcomes after GKS for CSCHs with markedly decreased tumor size after radiosurgery and no morbidity. 12 Since then, stereotactic radiosurgery (SRS) is recommended as either an adjunct to craniotomy or as the primary treatment for small CSCHs. More recently, radiosurgery has emerged as an alternative treatment to microsurgery. A systematic review and meta-analysis of 59 patients undergoing GKS for CSCHs reported remarkable tumor shrinkage in 40 (67.8%) patients, partial shrinkage in 15 (25.4%) patients, and no change in 4 (6.8%) patients. 13 Symptoms completely resolved in 15.21% of patients, improved in 60.86%, and remained unchanged in 23.93%, with a single patient having additional trigeminal nerve disturbance. 13 In our study, symptoms resolved completely in 1 (8.3%) patient and improved in 11 (91.6%) patients. Yamamoto et al, in a seven-institute Japanese study, suggested that GKS can be the primary treatment if a tumor shows clear neuroimaging characteristics of CSCH with small lesions proven to be neither meningioma nor schwannoma. 14 In our study, no patients developed new neurological deficits following treatment, indicating that radiosurgery was relatively safe for high volume CSCHs. Currently, radiosurgery is being used more commonly and is a promising option for primary or postoperative management of patients with CSCHs. 15
The CyberKnife system is one of the best devices for SRT. The system offers both single- and multisession radiotherapy options. Traditional SRS was limited by high radiation doses when the tumor was adjacent to optical pathways. Hypofractionated SRT using CyberKnife can minimize radiation doses to the surrounding normal tissue and provide less neurotoxicity because of intervals between treatment sessions that allow for the recovery of normal cells. Fractioned SRT has radiobiological advantages over SRS because of reoxygenation of hypoxic tumor cells and redistribution of the cell cycle to a more sensitive phase between fractions. 16,17
The conventional goal of GKS is achieving tumor growth control, and reducing the mass volume is important to restore nerve function particularly related to direct compression of the cranial nerves. 18 Single-session GKS is more effective for small or medium-sized CSCHs than for larger tumors. Hypofractionated SRT using CyberKnife has been used for primary or postoperative management of patients with CSCHs with favorable results. Wang et al reported that magnetic resonance images showed a mean 77% tumor volume reduction (range, 44%-99%) in 14 patients with large (volume >20 cm3) CSCHs in a mean follow-up of 15 months (range, 6-36 months). 19 Our study showed a mean tumor volume reduction of 66% (range, 28.69%-94.16%), with all patients showing improved symptoms to different degrees, and no new neurological deficits. Only 1 (8.33%) patient in our study developed radiation-related cerebral edema with headache, nausea, and vomiting, which resolved with treatment. Radiation-induced optic neuropathy is an iatrogenic complication that causes severe, irreversible vision loss in one or both eyes within months to years following radiation therapy. The previous study observed more rapid tumor volume reduction in more short mean follow-up time. 19 The risk of radiation-related sequelae might be higher if the beneficial effects of fractionation are not used in benign cavernous sinus tumors. 20 Patients undergoing radiosurgery for parasellar lesions routinely receive maximum radiation doses to the optic pathways of 10 to 12 Gy, with a reported incidence of radiation-related optic nerve injuries of <2%. 21 Toxicity rates after SRS of 1.7% were reported in a meta-analysis of 10 CSCH studies (59 patients) with only 1 patient having additional trigeminal nerve disturbance without visual complications. 13
Currently, the new-generation device, Gamma Knife Icon (Elekta, Stockholm, Sweden), can also perform multifraction SRS. In a recent study, using the Gamma Knife was associated with the most flexible workflow and excellent dosimetry but could be limited by the treatment time required to treat multiple large brain metastases (at least 1 target volume larger than 10 cm3) with multifraction SRS compared with the CyberKnife and other linear accelerator radiosurgery devices. 22 The effect of the Gamma Knife on control in large-volume tumors needs to be confirmed by more clinical research.
The main limitations of our study are the retrospective design, small number of patients, and relatively short follow-up. Although no deaths or sever complications after a mean period of 16.3 months were reported, the follow-up periods were not sufficiently long. Only 5 of 11 of our patients had longer than a 1-year follow-up. Obviously, much longer follow-up and a larger population will be required to establish the long-term efficacy of hypofractionated SRT using CyberKnife for these high-volume lesions. So we cannot overemphasize the conclusion because these findings are preliminary. Although a longer follow-up period and a larger population are necessary to confirm these early results, this preliminary analysis is very encouraging. This article documents our preliminary experience of hypofractionated SRT using CyberKnife for high volume cavernous sinus hemangiomas.
Conclusion
Based on the current results, hypofractionated SRT using CyberKnife is an effective and safe alternative to microsurgery for the management of high volume CSCHs. Our patients experienced effective tumor shrinkage and improved cranial nerve deficits posttreatment. Therefore, hypofractionated SRT using CyberKnife can be considered a primary treatment for high volume CSCHs with a multisession protocol. Further investigation of hypofractionated SRT for high volume CSCHs is warranted to confirm our findings.
Footnotes
Acknowledgments
The authors acknowledge Dr Jiuhong Chen for her valuable advice of revising the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.