
Abstract
Purpose:
Information on the short- and long-term outcomes of induction chemoradiotherapy followed by surgery for cT3-4 non-small cell lung cancer is limited. We analyzed the short- and long-term outcomes of induction chemoradiotherapy followed by surgery for cT3-4 non-small cell lung cancer.
Methods:
Patients with non-small cell lung cancer who underwent induction chemoradiotherapy followed by surgery for cT3-4 non-small cell lung cancer were retrospectively reviewed (initial treatment group, n = 31). Their results were compared to those patients who underwent surgery as an initial treatment during the same period (initial surgery group, n = 35).
Results:
Downstaging was achieved in 14 (45%) patients in the initial treatment group. R0 resection was achieved in 28 (90%) patients in the initial treatment group and 31 (88%) patients in the initial surgery group. The 90-day mortality rate was 3% in each group. Postoperative complications occurred in 16 (52%) patients in the initial treatment group and 13 (37%) patients in the initial surgery group. The 5-year overall survival rate of the initial treatment group was significantly higher than that of the initial surgery group (62.6% vs 43.5%, P = .04). The 5-year overall survival rates of the initial treatment N0-1 group and the initial surgery N0-1 group were 88.9% and 49.3%, respectively; the difference was statistically significant (P = .02). Multivariate analysis using 4 factors (age [≤65 vs >65], cN [cN0-1 vs cN2], general condition [chemoradiotherapy fit vs chemoradiotherapy unfit], and treatment mode [induction chemoradiotherapy followed by surgery vs surgery as an initial treatment]) revealed that treatment mode (induction chemoradiotherapy followed by surgery) and cN status (cN0-1) were significantly associated with good overall survival and disease-free survival.
Conclusions:
Induction chemoradiotherapy followed by surgery for cT3-4 non-small cell lung cancer could be performed with an acceptable degree of surgical risk. At present, it is thought to be one of the reasonable treatment approaches for selected patients with cT3-4 disease, even those with a cN0-1 status.
Introduction
Lung cancer is the leading cause of cancer death worldwide. 1 The modern treatment options for non-small cell lung cancer (NSCLC) include surgery, chemotherapy, radiotherapy (RT), molecular targeted therapy, and immunotherapy. In general, systemic therapies (ie, chemotherapy) are selected for patients with stage IV NSCLC, while surgery remains an important treatment option for stage I to III NSCLC.
Patients with locally advanced lung cancer (ie, cT3-4 and/or N2-3 disease) are good candidates for multidisciplinary treatment. Induction chemoradiotherapy (CRT) followed by surgery is a viable treatment strategy for clinical N2 NSCLC. 2 -4 Induction CRT followed by surgery is an established treatment for cT3-4 NSCLCs located in the superior sulcus tumors (SSTs). 5 -8 However, whether induction CRT followed by surgery or surgery as an initial treatment (IT) should be selected for cT3-4 NSCLCs other than SSTs remains controversial. In particular, surgery as an IT is empirically applied for cT3-4N0-1 disease in many institutions without any clear evidence to prove that the strategy is better than other treatment options.
In this setting, some institutions have reported the favorable results of induction CRT followed by surgery for cT3-4 NSCLC. 9,10 Recently, a prospective multi-institutional phase II study of induction CRT followed by surgery for NSCLC with chest wall involvement showed good results. 11
In our institution, induction CRT followed by surgery has been proactively applied for cT3-4 NSCLCs. In the present study, we retrospectively analyzed the short- and long-term outcomes of induction CRT followed by surgery for cT3-4 NSCLC to demonstrate the efficacy of this treatment strategy. The results of patients who were treated with this strategy were compared to those who underwent surgery as an IT for cT3-4 NSCLC in the same period.
Method
Patients and Data Collection
Patients with NSCLC who underwent induction CRT followed by surgery for clinical T3-4 NSCLC involving the adjacent organs at Osaka University Hospital between 1996 and 2014 were reviewed. The staging was assessed according to the International Association of Study of Lung Cancer Staging Manual in Thoracic Oncology, 7th edition. 12 Patients with SSTs were excluded from this analysis to reduce the heterogeneity of the patients; these patients represent a distinct population from patients with other T3-4 disease because there is good evidence to support the superiority of induction CRT. 6,7 Patients whose cT status was determined based on a size of >7 cm or the presence of pulmonary metastasis were excluded from this analysis because the study aimed to recruit patients with disease involving adjacent organs.
A total of 120 patients with cT3-4 (with adjacent organ involvement) cN0-2cM0 disease underwent treatment. Four patients with cT3-4 (with adjacent organ involvement) N3and/orM1b disease who underwent induction CRT followed by surgery were also included in the present study because the analysis of the outcomes of induction CRT followed by surgery was the main purpose of this study. Patients who received the best supportive care were not included in the present study; then, a total of 124 patients were reviewed. The treatment mode of these 124 patients was as follows: surgery as an IT in 35 (initial surgery [IS] group), induction CRT followed by surgery in 31 (IT group), definite CRT in 27, induction computed tomography (CT) followed by surgery in 13, RT alone in 13, CT alone in 3, and induction RT followed by surgery in 2. In the present study, the results of 31 patients who underwent CRT followed by surgery (IT group) were retrospectively analyzed. Thirty-five patients who underwent IS with curative intent for clinical T3-4 NSCLC involving the adjacent organs (IS group) were analyzed as a control group. The clinical records of all 66 patients were thoroughly reviewed in a retrospective manner. The data on the patients’ medical history (pulmonary, cardiovascular and cerebrovascular diseases, diabetes mellitus, and kidney diseases) and respiratory function were collected. The criteria for chronic obstructive pulmonary disease (COPD) that were applied in the present study were outlined in the Guidelines for the Diagnosis and Treatment of COPD, 3rd edition, which was published by the Japanese Respiratory Society. 13 The criteria for chronic kidney disease in this study were outlined in The Clinical Practice Guideline Book for Diagnosis and Treatment of Chronic Kidney Disease, 2012 by the Japanese Society of Nephrology. 14 The postoperative complications were graded according to the Clavien-Dindo classification of surgical complications. 15 All of the specimens were diagnosed by pathologists in our hospital. The effectiveness of induction CRT was assessed according to the general rules for clinical and pathological records of lung cancer of the Japanese Lung Cancer Society. 16 When a pathologic complete response was achieved by induction therapy, the yp stage was defined as stage 0. This study is approved by the Ethical Review Board for Clinical Studies at Osaka University (control number 10026-3).
Selection of Treatment Mode for cT3-4 Disease
Selection of treatment mode was decided on multidisciplinary cancer board. For cT3-4 (with invasion to adjacent organs) cN0-2M0 disease, resectability is evaluated by thoracic surgeons based on radiologic examinations as 3 classifications, that is, resectable, marginally resectable, and unresectable. When the disease was evaluated as marginally resectable, CRT is selected, and resectability is reevaluated when 40 Gy of RT is finished. When the disease was evaluated as resectable at that point, surgery was performed, and the patient underwent induction CRT followed by surgery as a result. On the contrary, when the disease was evaluated as unresectable at that point, additional 20 Gy of RT is performed.
Induction CRT
Platinum doublet chemotherapy was usually used, and the regimen was determined by the cancer board in each case. Basically, 2 courses of chemotherapy with concurrent RT using a conventional fraction (2 Gy/d) were administered. The total dose of RT was generally 40 Gy.
Surgery, Postoperative Therapy, and Follow-Up
A hemi-clamshell approach was selected for patients with tumors involving the mediastinal structures and mediastinal lymph nodes. 17 The extent of resection was determined by the location and extent of the disease. Sleeve lobectomy was proactively performed to preserve the respiratory function; however, pneumonectomy was an option when complete resection could be achieved. 18,19 The combined resection of the great vessels and the heart was proactively performed. 20,21 When the phrenic nerve was involved by the tumor, it was resected and plication of the diaphragm was performed to preserve the respiratory function. 22
In general, adjuvant therapy is not indicated for patients with complete resection of the disease following induction CRT. Adjuvant chemotherapy, RT, or CRT was indicated for patients who underwent incomplete resection.
Chest roentgenograms and measurements of the serum carcinoembryonic antigen level (as a tumor marker) were performed every 3 to 6 months after surgery, and contrast chest CT, contrast brain CT or magnetic resonance imaging, and bone scintigraphy or positron emission tomography/CT were routinely performed each year during follow-up as surveillance to detect the recurrence of lung cancer.
Statistical Analysis
The differences in the clinical variables of the 2 groups were evaluated using Student t test or the χ2 exact test. The overall survival (OS) and disease-free survival (DFS) after surgery were analyzed using the Kaplan-Meier method. The significance of the differences between the subgroups was calculated using the log-rank test. A Cox proportional hazards model was used for multivariate analysis. The statistical analyses were performed using the JMP Pro 13 software program (SAS Institute, Berkley, California).
Results
Overall Survival of Patients With cT3-4N0-3M0 Disease
In the present study, the time between treatment and the last follow-up examination of all 124 patients ranged from 1 to 245 months (median: 49 months). Eighty-six cases were classified as resectable or marginally resectable, while 38 were classified as unresectable. Thirty-six patients started CRT with the intention of undergoing a subsequent operation; however, 5 cases were classified as unresectable after 2 courses of chemotherapy and RT (40 Gy). These 5 patients underwent definitive CRT. Finally, 31 patients underwent induction CRT followed by surgery.
We analyzed OS according to resectability, which was determined before treatment based on the results of radiological examinations (Figure 1). The 5-year OS rates of resectable or marginally resectable patients were significantly higher than those of unresectable patients (54.3% vs 32.4%; P = .01).

Kaplan-Meier plots of overall survival rate according to the resectability which is determined before treatment by radiological examinations. The 5-year overall survival rate of resectable or marginally resectable patients were significantly higher than that of unresectable patients (54.3% vs 32.4%, P = .01).
The OS rates of these patients according to the mode of treatment are shown in Figure 2 (patients who underwent CT alone or induction RT followed by surgery were omitted due to the small numbers of patients). The 5-year OS rates of patients who underwent surgery as an IT, induction CRT followed by surgery, definitive CRT, induction CT followed by surgery, and RT alone were 43.5%, 62.6%, 49.2%, 58.0%, and 12.9%, respectively.
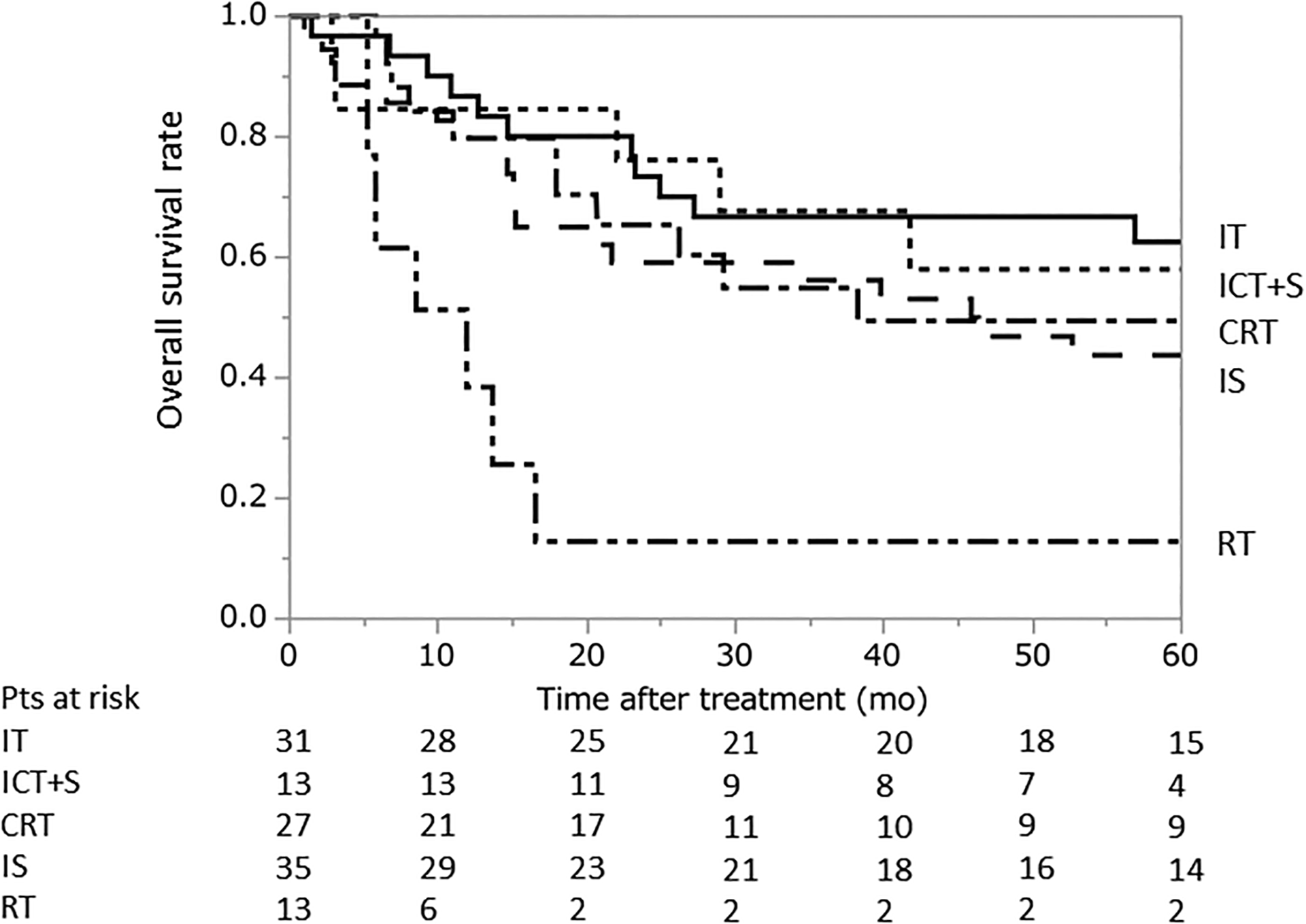
Kaplan-Meier plots of the overall survival rates according to treatment mode. The 5-year overall survival rates of patients who underwent surgery as an initial treatment, induction CRT followed by surgery, definitive CRT, induction CT followed by surgery, and RT alone were 43.6%, 62.6%, 49.2%, 58.0%, and 12.9%, respectively. CRT indicates chemoradiotherapy.
Patient Characteristics of the IT and IS Groups
In the present study, the time between surgery and the latest follow-up examination ranged from 1 to 192 months (median: 46 months). The characteristics of the IT (n = 31) and IS (n = 35) groups are shown in Table 1. The mean age of the IT group was significantly younger than that of the IS group (57.7 vs 68.2 years; P < .01). There were no significant differences between the 2 groups with regard to sex and smoking status. There were no significant differences in the body mass index and respiratory function tests between the 2 groups. In terms of comorbid diseases, the rates of cerebrovascular disease and interstitial lung disease in the IS group were significantly higher in comparison to the IT group (P = .04 and .02, respectively). In the IS group, 14 patients were considered to be fit for induction CRT, while 21 patients were considered to be unfit based on their general condition or the detection of comorbid diseases. The reasons why the patients were considered to be unfit for induction CRT included advanced age (n = 6), interstitial lung disease (n = 4), pneumonia (n = 3), an impaired respiratory function (n = 2), an impaired renal function (n = 1), and other reasons (n = 5).
The Patient Characteristics.

Abbreviations: COPD, chronic obstructive pulmonary disease; FEV, forced expiratory volume; IT, induction treatment; IS, initial surgery; PA, pulmonary artery; VC, vital capacity; NS, not significant.
a When multiple organs were involved in 1 patient, the higher T stage or representative organ is selected.
The involved organs differed between the 2 groups. In the IS group, there were 11 (31%) patients with tumors with a parietal pleura or a mediastinal pleura; in contrast, there were no patients with these conditions in the IT group. There was a significant difference in the clinical N statuses of the patients in the 2 groups; 19 (61%) patients in the IT group were diagnosed with cN2 disease, while 21 (60%) patients in the IS group were diagnosed with cN0 disease. Thus, the c-stage differed between the 2 groups. The histological types did not differ between the 2 groups to a statistically significant extent.
Induction CRT
The details of induction CRT are summarized in Table 2. Cisplatin-based regimens were used in 21 patients and carboplatin-based regimens were used in 9 patients. A partial response was achieved in 17 (55%) patients. One to 6 cycles of chemotherapy were administered. Twenty-three (74%) patients received 2 cycles of chemotherapy. Radiotherapy was performed concurrently in 27 (87%) patients, while it was performed sequentially in 4 (13%) patients. Downstaging was achieved in 14 (45%) patients. A pathologic complete response was achieved in 7 (23%) patients.
The Details of the Induction Chemoradiotherapy Regimens.

Abbreviations: CBDCA, carboplatin; CDDP, cisplatin; CR, complete response; DTX, docetaxel; ETP, etoposide; GEM, gemcitabine; MMC, mitomycin C; PTX, pacritaxel; VDS, vindesine; VNR, vinorelbine.
The Operative and Pathologic Factors
The operative and pathologic factors are summarized in Table 3. In the IT group, a hemi-clamshell approach was selected as the surgical approach in 13 (39%) patients, while it was selected for 3 (9%) patients in the IS group (P < .01). In both the groups, approximately 70% of the patients underwent lobectomy, and the distribution and the extent of resection did not differ to a statistically significant extent. The rate of patients who underwent pulmonary artery plasty in the IT group was significantly higher than that in the IS group (32% vs 11%, P = .04). Combined resection of the mediastinal pleura (only the pleura and not mediastinal structures) was performed in 4 (11%) patients in the IS group, and no patients in the IT group (P = .02). ND2 was performed in about 80% to 90% of the cases in both the groups. The operation time of the IT group was significantly longer than that of the IS group (P < .01). In the IT group, the amount of blood loss of was significantly larger, and the rate of patients who received blood transfusion was significantly higher in comparison to the IS group (P < .01). R0 resection was achieved in 28 (90%) patients in the IT group and 31 (88%) patients in the IS group; these rates did not differ to a statistically significant extent.
The Operative and Pathologic Factors.

Abbreviations: PA, pulmonary artery; IT, induction treatment; IS, initial surgery.
a Includes 1 median sternotomy.
b Includes 1 thoracoscopic surgery.
Postoperative Complications
There were no cases of 30-day mortality in either group. Among all 66 patients, 2 patients died (one in each group) within 90 days after surgery; thus, the 90-day mortality rate was 3% in both the IT and the IS groups. In detail, the patient in the IT group who underwent right upper lobectomy with the resection of the carina and carinal reconstruction following induction CRT had anastomotic leakage and eventually died on postoperative day 44. The patient in the IS group died on postoperative day 33, after undergoing left pneumonectomy and having a massive pulmonary artery embolism. Postoperative complications (any grade) occurred in 16 (52%) patients in the IT group and 13 (37%) patients in the IS group; these rates did not differ to a statistically significant extent. Postoperative complications (grade ≥ 3) occurred in 7 (23%) patients in the IT group and 6 (17%) patients in the IS group; these rates did not differ to a statistically significant extent. The details of the postoperative complications are shown in Table 4.
The Details of the Postoperative Complications.
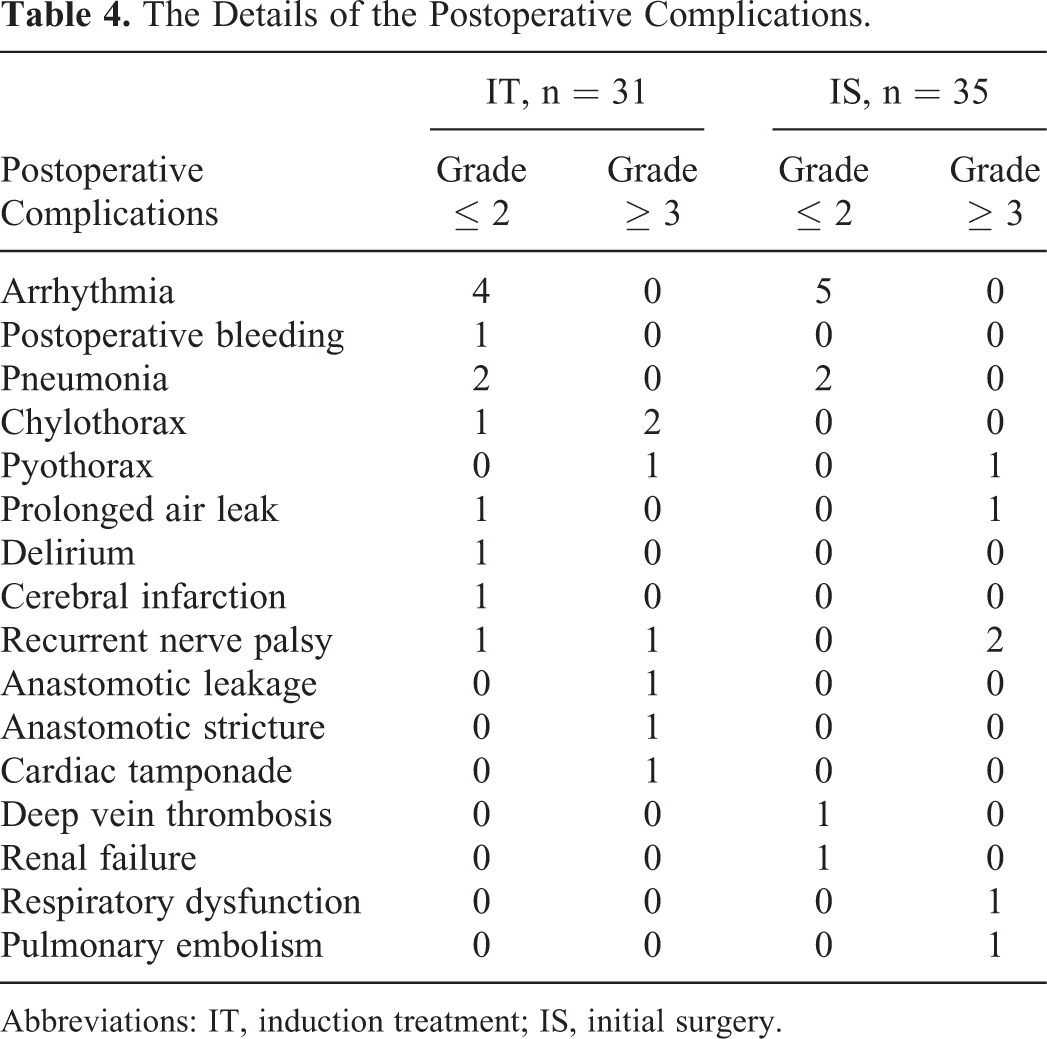
Abbreviations: IT, induction treatment; IS, initial surgery.
Postoperative Therapy
Two patients in the IT group received postoperative therapy. One patient with ypN2 disease received adjuvant chemotherapy, and 1 patient who underwent R2 resection received chemoradiation. On the other hand, 8 patients received postoperative therapy in the IS group. Three patients received adjuvant chemotherapy and 5 patients received RT (including one patient who underwent R2 resection).
The Long-Term Outcomes
To date, 10 patients in the IT group and 16 patients in the IS group have experienced recurrence. In the IT group, the patterns of recurrence were local relapse (n = 5), distant (n = 3), local and distant (n = 1), and unknown (n = 1). In the IS group, the patterns of recurrence were local relapse (n = 4), distant (n = 11), and local and distant (n = 2). The rates of local relapse in the 2 groups did not differ to a statistically significant extent.
The 5-year DFS rates of the IT and IS groups were 59.6% and 36.3%, respectively (P = .10). The 5-year OS rates of the IT and IS groups were 62.6% and 43.5%, respectively, and the difference was statistically significant (P = .04; Figure 3) Next, we analyzed the long-term outcomes of the cN0 -1 patients in both the groups. The 5-year DFS rates of the IT N0-1 and IS N0-1 groups were 88.9% and 42.4%, respectively, and the difference was statistically significant (P = .02). The 5-year OS rates of the IT N0-1 group and the IS N0-1 group were 88.9% and 49.3%, respectively; the difference was statistically significant (P = .02; Figure 4). Because there was difference in the comorbid conditions (as shown in Table 1), it is possible that the long-term outcomes of the IS group were influenced by their comorbid conditions. To reduce this influence, we excluded patients who were considered to be unfit for induction CRT and reanalyzed the long-term outcomes of the IT N0-1 group and the IS N0-1 “induction CRT-fit” group. The characteristics of these 2 groups are shown in Table 5. There were no differences between the 2 groups with regard to age, sex, respiratory function, or comorbid diseases. The operation time was longer in the IT N0-1 group; there were no differences in the other factors. Even after these adjustments, both the 5-year DFS and the OS of the IT N0-1 group were significantly higher in comparison to the IS N0-1 “induction CRT-fit” group (DFS: 88.9% vs 41.7%, P = .01, OS: 88.9% vs 50.0%, P = .01; shown in Figure 5).

(Upper) Kaplan-Meier plots of the disease-free survival rates of the initial treatment (IT) and Initial Surgery (IS) groups. The 5-year disease-free survival rates of the IT and IS groups were 59.6% and 36.3%, respectively (P = .10). (Lower) Kaplan-Meier plots of the overall survival rates of the IT and IS groups. The 5-year overall survival rates of the IT and IS groups were 62.6% and 43.5%, respectively; the difference was statistically significant (P = .04).

(Upper) Kaplan-Meier plots of the disease-free survival rates of the initial treatment (IT) N0-1 and Initial Surgery (IS) N0-1 groups. The 5-year disease-free survival rates of the IT N0-1 group and the IS N0-1 group were 88.9% and 42.4%, respectively; the difference was statistically significant (P = .02). (Lower) Kaplan-Meier plots of the overall survival rates of the IT N0-1 and IS N0-1 groups. The 5-year overall survival rates of the IT N0-1 and the IS N0-1 groups were 88.9% and 49.3%, respectively; the difference was statistically significant (P = .02).
The Characteristics of the IT N0-1 Group and the IS N0-1 “Induction CRT-fit” Group.

Abbreviations: CRT, chemoradiotherapy; IT, induction treatment; IS, initial surgery; NS, not significant; COPD, chronic obstructive pulmonary disease; FEV, forced expiratory; PA, pulmonary artery; VC, vital capacity.

(Upper) Kaplan-Meier plots of the overall survival rates of the initial treatment (IT) N0-1 and Initial Surgery (IS) N0-1 “induction CRT-fit” groups. The 5-year overall survival rates of the IT N0-1 and IS N0-1 “induction CRT-fit” groups were 88.9% and 41.7%, respectively; the difference was statistically significant (P = .01). (Lower) Kaplan-Meier plots of the overall survival rates of the IT N0-1 and IS N0-1 “induction CRT-fit” groups. The 5-year overall survival rates of the IT N0-1 group and the IS N0-1 “induction CRT-fit” group were 88.9% and 50.0%, respectively; the difference was statistically significant (P = .01).
Multivariate Analysis
To test whether the treatment mode independently affects survival, a multivariate analysis was conducted for OS and DFS. The 3 factors that were considered to be associated with the outcomes age (≤65 vs >65), cN (cN0-1 vs cN2-3), general condition (CRT fit vs CRT unfit), and treatment mode (induction CRT followed by surgery vs. surgery as an IT) were selected as covariates. The results of the multivariate analysis are shown in Table 6. As a result, treatment mode (induction CRT followed by surgery) and cN status (cN0-1) were found to be significantly associated with good OS and DFS.
Results of Multivariate Analysis.

Abbreviations: CRT, chemoradiotherapy; CI, confidence interval.
Discussion
In the present study, we demonstrated that induction CRT followed by surgery is clinically feasible for cT3-4 NSCLC. The OS of the IT group was significantly better than that of the IS group and that difference was also observed in the cN0-1 population. Furthermore, the long-term outcomes of the patients in the IT N0-1 group were significantly better than those in the IS N0-1 “induction CRT-fit” group who showed equivalent characteristics.
Theoretically, induction CRT has some advantages and disadvantages in comparison to surgery as the IT. The advantages are as follows. First, there is a possibility that induction CRT could provide a higher rate of complete resection in comparison to surgery as the IT. To ensure the surgical margin is occasionally difficult in cT3-4 NSCLC, in such cases, the use of induction CRT to diminish the tumor may improve local control. Second, performing systemic treatment first can help to eliminate micrometastasis developing through blood flow or pleural dissemination in the early period. The tolerability of preoperative CRT may be better than postoperative chemotherapy because the general condition of the patient may change after surgery. Thirdly, the response to chemotherapy can be assessed; this information can be useful for planning postoperative chemotherapy or chemotherapy for recurrent disease. The disadvantages are as follows: Firstly, the rate of postoperative complications may be increased as a result of tissue damage when the respiratory function decreases due to induction therapy. 23 Secondly, if there is no response to induction CRT (ie, the tumor becomes enlarged during chemotherapy or new metastasis occurs), the optimal timing of surgery can be delayed. Thirdly, common adverse effects of chemotherapy (ie, infection) can occur.
We demonstrated the theoretical advantages and disadvantages of induction CRT; however, it is difficult to determine the best treatment strategy because a randomized trial is not practical due to the rarity of the disease. In the present study, the R0 resection rate in the IT group was 90% while that in the IS group was 88%. Considering the advanced stage of the disease, this figure seems satisfactory. Unfortunately, we could not assess the adverse effects of induction CRT in the present study because the data were not included in our database. The 90-day mortality rate was 3%, and the rate of postoperative complications in the IT group was as high as 52%. One patient who underwent right upper lobectomy with the resection of the carina and carinal reconstruction following induction CRT died in the IT group. The rate of 3% is similar to that in Daly’s series, which was 2.1%. 23 In the most recent report on pulmonary resection combined with bronchoplasty after induction CRT from one of the leading institutions in Japan, the mortality rate was 5%. 23 Based on these data, we believe that the mortality and morbidity rates were acceptable considering the extension of the disease and the extensive type of resection.
Several groups have reported evidence in favor of induction CRT for patients with locally advanced NSCLC. In terms of SST, established reports from Japan and North America have demonstrated that induction CRT followed by surgery provides favorable outcomes. 6 -8 Patients with clinical N2 disease are also good candidates for induction CRT, and this strategy is adopted in many institutions worldwide. 2 -4 On the other hand, data on induction CRT followed by surgery in patients with cT3-4 NSCLC (besides SST) remain limited.
Some authors have reported that induction CRT is not beneficial for cT3-4 NSCLC. Lococo et al 24 reported data from a multicenter study in Italy. The outcomes of 31 patients with cT3-4N0 NSCLC (besides SST) who underwent induction CRT followed by surgery were compared to those of 40 patients with cT3-4N0 NSCLC (besides SST) who underwent IS. They concluded that there was no clear evidence that induction CRT improved the prognosis. Uramoto et al 25 reported the outcomes of 409 patients with pT3-4 disease who underwent surgery and demonstrated that induction therapy does not influence survival. Kawaguchi et al 26 performed a study using data on 531 patients with pT3 NSCLC from a Japanese nationwide database (Japan Lung Cancer Registry, 2004). Eighty-nine of these patients underwent induction therapy; however, there was no difference in survival between the IS and the induction therapy groups.
On the other hand, some authors reported that induction CRT was beneficial for patients with cT3-4 disease. Daly et al 10 compared the outcomes of 47 patients with cT3-4N0 NSCLC who underwent induction CRT followed by surgery with those of 63 patients who did not receive induction CRT. They reported that patients who did not receive induction CRT had an increased risk of death, even after adjustment for potential confounding variables. That group remained at an increased risk of death. Shien et al 9 reported similar results to our own. They compared 36 patients with cT3-4 NSCLC (including 4 SSTs) who underwent induction CRT followed by surgery with 40 patients who underwent IS. They demonstrated that OS was significantly better in the induction CRT group, and this difference was observed when the analysis was limited to cT3-4N0-1 disease.
As described earlier, it is difficult to reach a consensus on the strategy for cT3-4 NSCLC at the present time. One reason for that difficulty is that most of the reports have come from retrospective analyses that were performed at a single institution. The treatment strategies for cT3-4 NSCLC differ among institutions. Furthermore, the strategy that is applied is selected at the surgeon’s discretion. In institutions where induction CRT is proactively selected, the medically fit, younger patients tend to undergo induction CRT rather than IS. In this situation, it is thought that the outcomes of induction CRT followed by surgery would tend to be better than those of IS due to the difference in the patient background. Propensity score matching is useful for reducing the influence of the patient selection bias on the outcomes. In Shien et al’s series (mentioned above), 9 they also demonstrated that the survival of patients who underwent induction CRT followed by surgery was significantly better than that of patients who underwent IS after the adjustment of potentially confounding variables. In the present study, we excluded patients who were considered to be unfit for induction CRT and reanalyzed the long-term outcomes of the IT N0-1 group and IS N0-1 “induction CRT-fit” group; after these steps, both the 5-year DFS and OS of the IT N0-1 group were significantly higher in comparison to the IS N0-1 “induction CRT-fit” group. These data suggest that induction CRT is beneficial for cT3-4 NSCLC; however, a bias could not be completely ruled out because of the retrospective nature of the study. Another reason for difficulty in reaching a consensus on the strategy for cT3-4 NSCLC is the heterogeneity of the patient group. 27 For example, the surgical risk for T4 aortic invasion and T3 parietal pleural invasion is essentially different. Thus, the composition of the patient groups is different, which makes them difficult to compare. For this reason, a prospective multi-institutional study for each patient group is needed to obtain credible data to determine the best treatment strategy for cT3-4 NSCLC. Kawaguchi et al 11 recently reported the results of a prospective multi-institutional study of induction CRT for patients with cT3N0-1 NSCLC having chest wall invasion. They noted a favorable outcome, with a 5-year OS rate of 63%. Further studies will be needed to confirm the benefit for other cT3-4 patient groups.
In the present study, the 5-year OS rates of the IT, ICT+S, CRT, IS, and RT groups were 62.6%, 58.0%, 49.2%, 43.5%, and 12.9%, respectively. Although these values should not be directly compared due to the retrospective nature of the present study, the 5-year OS of patients who underwent induction CRT followed by surgery was the best. On the other hand, the outcome of patients who underwent CRT was favorable in comparison to previous reports on the outcomes of CRT in patients with stage III NSCLC. It is considered that the favorable outcome of CRT may be explained by the cN status. In fact, the cN status of the CRT patients (n = 27) was N0 in 6, N1 in 2, and N2 in 19 patients (ie, 30% were cN0 -1). Recently, very favorable results of combination of immunotherapy and CRT (durvalumab after CRT) in stage III NSCLC were reported. 28 Whether induction CRT followed by surgery (as presented in the present study) or a combination of immunotherapy and CRT is better for locally advanced NSCLC is the next question.
The present study is associated with some limitations. Firstly, the induction chemotherapy regimens were not unified due to the retrospective nature of the study. Further studies are needed to determine the optimal regimen. Secondly, the study period was relatively long. Marked advancements in radiological examination techniques occurred during the study period. This might have affected patient selection. Thirdly, the number of patients was limited. A multicenter study with a larger study population would be desirable.
In conclusion, induction CRT followed by surgery for cT3-4 NSCLC could be performed with an acceptable degree of surgical risk. At present, it is thought to be one of reasonable treatment approaches for selected patients with cT3-4 disease, even those with a cN0-1 status.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.