
Abstract
Purpose:
To establish a computed tomography–based prognostic model for patients with hepatocellular carcinoma treated with transarterial chemoembolization.
Materials and Methods:
Using prospectively collected data from 195 consecutive patients with hepatocellular carcinoma who underwent chemolipiodolization at the Eastern Hepatobiliary Surgery Hospital between 2013 and 2016, we established a prognostic model based on hepatocellular carcinoma enhancement patterns on computed tomography scans to predict the outcome of transarterial chemoembolization. Furthermore, a histopathology analysis was performed on 108 different patients undergoing resection between 2014 and 2016 to identify whether there was a correlation between enhancement pattern and microvessel density.
Results:
The prognostic model classified hepatocellular carcinoma into 3 types: type I, which reached peak enhancement during the arterial phase and had a high mean microvessel density (101.5 vessels/0.74 mm2); type II, which reached peak enhancement during the portal venous or delayed phase and had an intermediate microvessel density (53.6 vessels/0.74 mm2); and type III, in which the tumor was insignificantly enhanced and had a low microvessel density (21.1 vessels/0.74 mm2). For type I, II, and III hepatocellular carcinoma, the post-transarterial chemoembolization 1-year tumor complete necrosis rates were 13.7%, 36.5%, and 0%, respectively (P < .001), and the 3-year overall survival rates were 14.1%, 38.6%, and 0%, respectively (P < .001).
Conclusion:
Our results indicate that hepatocellular carcinoma type is an independent predictor of complete necrosis and overall survival
Keywords
Introduction
Transarterial chemoembolization (TACE) is the most commonly used treatment for patients with intermediate-stage hepatocellular carcinoma (HCC) according to the Barcelona Clinic Liver Cancer (BCLC) classification. 1,2 It has been shown to benefit survival by downstaging unresectable or nontransplantable HCC. 3 -6 However, reported survival rates vary significantly from 24% to 55% at 3-year post-TACE treatment. 7 -10 Multiple factors, including tumor load, liver function, drugs and emulsion types used for TACE, and tumor response to TACE, have been proposed to be associated with patient survival. 11 -13 It is therefore difficult to predict which subgroup of patients with HCC will benefit most from this procedure. Moreover, a standard regimen, concerning patient selection and the treatment schedule, type of chemotherapy, or embolizing agent used, remains to be elucidated. 14,15
Lipiodol is commonly used for TACE as a drug-carrying, tumor-seeking, and vascular-embolizing agent. 11,16,17 The degree of lipiodol retention has been associated with tumor response and used as a positive prognostic predictor for TACE. 18,19 Complete lipiodol retention may cause tumor complete necrosis (CN) and prolong patient survival. 15,20 -22 Unfortunately, the degree of lipiodol retention can only be evaluated following TACE treatment, and accurate prognostic predictors available for use prior to TACE treatment remain unknown.
Since TACE involves not only embolizing tumor capillaries, but also enhancing the exposure time of malignant tumor cells to chemotherapeutic agents, tumor vascularity is important to the outcome of TACE treatment. 3,23 A previous study reported that vascularity changed with tumor size and differentiation. 24 Changes in vascularity could affect vascular permeability as well as the speed and viscosity of blood flow, which will impact the absorption or washout of chemotherapeutic agents in the tumor. 25,26 Tumors with hypervascularity can achieve CN with optimal lipiodol retention after only one session of TACE. 18,27,28 Several studies have demonstrated that this type of tumor vascularity showed tumor enhancement and attenuation on functional computed tomography (CT) scans. 29 -31 Whether vascularity features on CT scans can be used to predict the outcome of TACE treatment has not been reported. 32
To provide radiologic–pathologic evidence for this issue, we established a prognostic model based on the enhancement patterns of HCC on CT scans to predict the outcome of a cohort of patients undergoing TACE. Furthermore, we performed a histopathology analysis on a separate cohort of patients undergoing resection to identify correlations between enhancement pattern and microvessel density (MVD) or maximum microvessel diameter (MMVD) to explain TACE treatment outcomes.
Material and Methods
Patients and Study Design
For this study, the clinical diagnosis of HCC was based on the criteria of the American Association for the Study of Liver Diseases. 1,33 Biopsy was considered for tumors with atypical imaging features. The study was approved by the Institutional Ethics Committee of the Eastern Hepatobiliary Surgery Hospital (EHBH). Informed consent was obtained from all patients to use their data.
Between July 2013 and July 2016, the data from consecutive patients who received abdominal contrast-enhanced CT scans and underwent chemolipiodolization as first-line treatment for HCC were prospectively collected at the EHBH. The therapeutic selection of TACE was largely based on the BCLC staging system. 33,34 All of these patients had unresectable tumors due to late-stage, unfavorable tumor location, or insufficient liver function. The inclusion criteria were (1) Grade 0-1 based on Eastern Cooperative Oncology Group performance status; (2) BCLC stage B, C, or late-stage A tumors; and (3) Child-Pugh liver function scores in class A or B5-7. Patients who received other anti-HCC treatments following TACE, including resection, percutaneous ablation, sorafenib, or radiotherapy, or who refused to take part in the study or were lost to follow-up were excluded. Eligible patients comprising the chemolipiodolization cohort were used to establish a CT-based prognostic model.
Between February 2014 and December 2016, based on our previously reported surgical indications, 35 we prospectively collected data from consecutive patients at the EHBH who received preoperative abdominal contrast-enhanced CT scans and underwent hepatectomy as first-line treatment for HCC. Hepatocellular carcinoma was histologically classified using the Edmondson-Steiner classification. 36 These patients comprised the surgical cohort, which was used to investigate the radiologic–pathologic correlation between CT-based model type and tumor vascularity. The median follow-up for these patients was 16 months (range: 3.1-36 months).
Characteristics of HCC Blood Supply on CT scans
Computed tomography examination was performed with a multislice spiral CT scanner (GE Optima 64, USA). Following the injection of 300 mg/mL of nonionic contrast medium (Omnipaque, Bayer Schering Pharma, leverkusen, Germany) at a rate of 2.5 to 3.00 mL/s, the image data for the arterial, portal venous, and delayed phases were obtained between 15-30 seconds, 50-60 seconds, and 2-3 minutes, respectively. 37 The CT scanning parameters were 120 kV, 270-300 mA, 5 mm layer thickness, and 5 mm outline space. The detector array was 128 × 0.625 mm. Moreover, the acquisition matrix size was 512 × 512 (time interval: 5 seconds) at a speed and dose of 3 mL/s and 1.2 to 1.5 mL/kg, respectively. Computed tomography scans were obtained through the picture archiving and communication system. Computed tomography values during the 4 phases were measured using Rad Works, version 5.1. Hepatocellular carcinoma was classified according to patterns of contrast enhancement and attenuation during different phases of the CT scan.
Transarterial Chemolipiodolization
Chemolipiodolization was performed by 2 interventional oncologists who had experience performing over 1000 TACEs for HCC. The TACE procedure involved the infusion of epirubicin (40 mg; Pharmorubicin, Pfizer, New York, USA) and lipiodol (6-18 mL; Guerbet Laboratories, Aulnay-sous-Bois, France) emulsion through the segmental and subsegmental hepatic arteries by a superselective technique. The dose of lipiodol depended on whether it could fill the tumor completely, as indicated by stagnant flow of lipiodol in the artery on digital subtraction angiography (Advantx TC; GE, Fairfield, Connecticut, USA). The emulsification procedure was standardized and employed using the “pushing and pulling technique,” which involves the preparation of stable emulsion microdroplets by pushing and pulling both compounds approximately 20 times through a 3-way stopcock between two 10 mL syringes. 11,23 Patients were examined again with a CT scan 1 month following each TACE treatment. Repeat TACE was considered 1.5 months later if CN was not achieved and if patients could tolerate another TACE treatment and had liver function within Child-Pugh class A or had a score of B5-7. 38
Assessment of Tumor Necrosis Following TACE
Using the criteria of the modified Response Evaluation Criteria in Solid Tumors (mRECIST), the degree of tumor necrosis, lipiodol retention, and tumor progression following TACE were recorded and compared. 39 The results were defined as complete response (CR) or CN, partial response (PR), progressive disease (PD), or stable disease (SD). Partial response, PD, and SD were regarded as incomplete necrosis.
Investigation of the Association Between the HCC CT-Based Prognostic Model and Histopathological Examination
In the surgical cohort, MVD and MMVD were evaluated in surgically resected HCC specimens by immunohistochemical staining of CD34 as recommended by previous reports and detailed in Supplementary Patients and Methods. 40,41 The associations between CT-based prognostic model type and MVD or MMVD were analyzed.
Follow-Up
Patients were followed up 1 month after therapy and then once every 2 months within the first year and once every 3 months thereafter. For patients who underwent TACE, a contrast-enhanced CT was performed at 1 month of follow-up and then once every 3 months or earlier when clinically indicated. The end points of this study were time to progression and overall survival after TACE treatment. Time to progression was defined as the interval between the first session of TACE and tumor progression assessed with mRECIST criteria, with lipiodol diffusion or the appearance of new enhancement areas within the tumor apparent on CT scan. Overall survival was defined as the interval between the first session of TACE and the patient’s death or last follow-up. The detailed follow-up program is presented in Supplementary Patients and Methods.
Statistical Analysis
All data are presented as the percentage or number of patients or mean with standard deviation. Categorical variables were compared using χ2 or Fisher exact tests, and continuous variables were compared using the Student t test or Kruskal-Wallis test. The association between 2 variables was analyzed using Pearson correlation coefficient and linear regression. Multivariate analysis was performed using nonconditional logistic regression. Overall survival was estimated by the Kaplan-Meier method. Survival curves were statistically compared using the log-rank test. Factors with P < .10 were selected for Cox proportional hazards model analysis. Statistical analysis was carried out using PASW Statistics for Windows, version 17.0 (SPSS, Inc, Chicago, Illinois). A value of P < .05 was considered statistically significant.
Results
Clinicopathological Characteristics
During the study period, data from 226 consecutive patients with HCC who received TACE as first-line treatment were prospectively collected. Of these patients, 195 met the inclusion criteria and were enrolled, constituting the TACE cohort. A total of 108 consecutive patients who received hepatectomy for HCC were also enrolled within the surgical cohort (Supplementary Figure 1). The clinicopathological characteristics of the 2 cohorts are shown in Supplementary Table 1.
Characteristics of Tumor Blood Supply and the CT-Based Prognostic Model
Based on the tumor blood supply observed on CT scans, the data from 303 patients enrolled in the TACE and surgical cohorts were used to establish an HCC prognostic model. For 196 patients with a solitary tumor, the blood supply varied considerably with different patterns of enhancement and attenuation. However, in 107 patients with multifocal tumors, the CT features of the nodules showed similar patterns of enhancement and attenuation with a homogeneity of 91.6% (98/107 patients, Supplementary Figure 2). Consequently, the CT-based prognostic model was largely determined by the characteristics of the largest nodule in patients with multiple HCCs (Supplementary Tables 2 and 3).
As shown in Table 1, patients with HCC were classified into 3 types. Briefly, type I HCC (n = 117) had a time to peak enhancement of CT values within the arterial phase (ie, 15-30 seconds after injection of the contrast agent), which corresponded to fast enhancement and quick attenuation. Type II HCC (n = 63) had a time to peak enhancement within the portal venous or delayed phases (60-180 seconds after injection), which corresponded to slow and continuous enhancement. Type III HCC (n = 15) had an insignificantly enhanced tumor with CT values at the baseline level with variation < 10. For the 108 patients in the surgical cohort, the CT values for type I, II, and III HCC were 75, 22, and 11, respectively (Table 2).
Clinical Characteristics for the 3 Types of HCC in the TACE Cohort.a
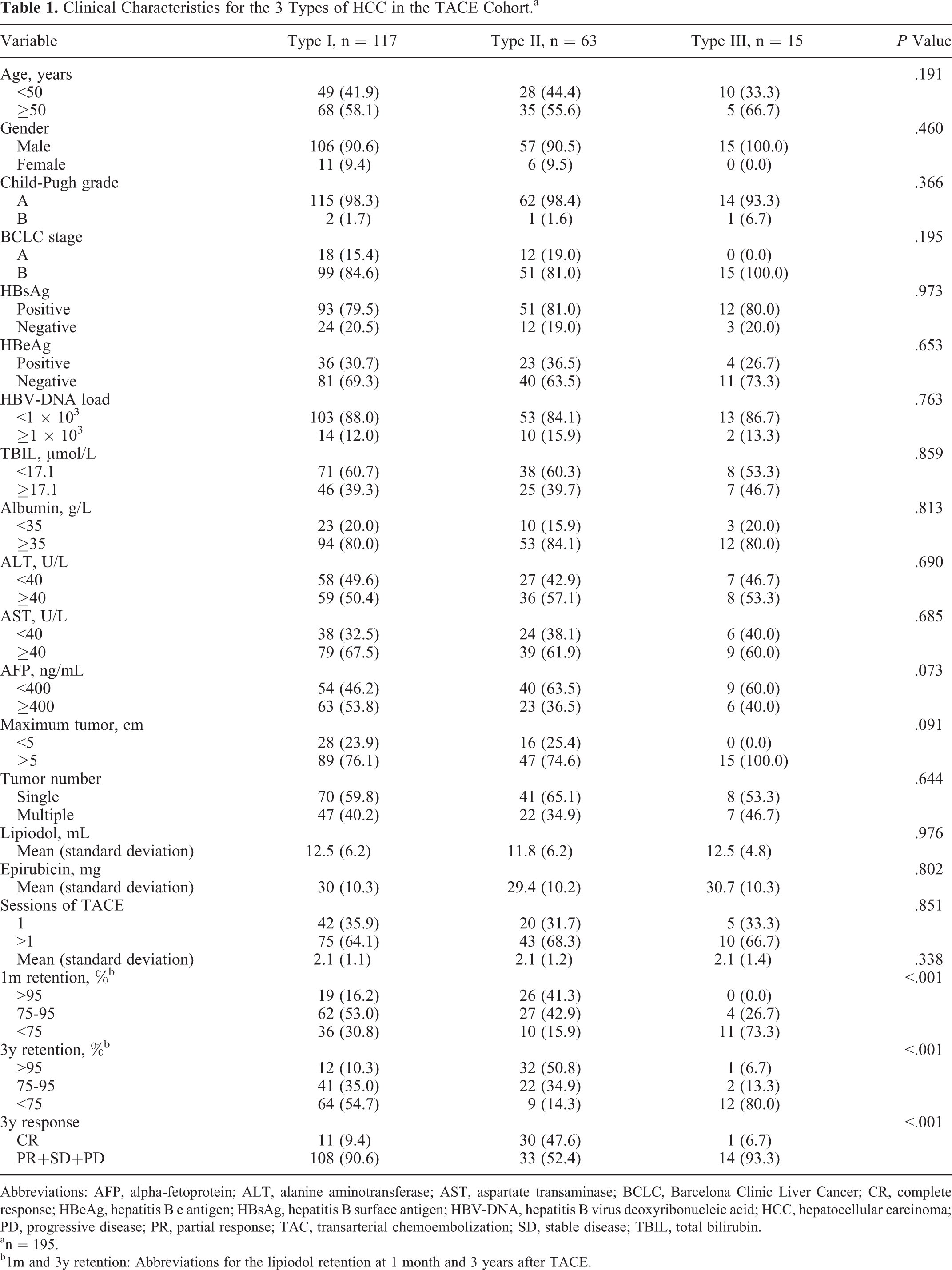
Abbreviations: AFP, alpha-fetoprotein; ALT, alanine aminotransferase; AST, aspartate transaminase; BCLC, Barcelona Clinic Liver Cancer; CR, complete response; HBeAg, hepatitis B e antigen; HBsAg, hepatitis B surface antigen; HBV-DNA, hepatitis B virus deoxyribonucleic acid; HCC, hepatocellular carcinoma; PD, progressive disease; PR, partial response; TAC, transarterial chemoembolization; SD, stable disease; TBIL, total bilirubin.
an = 195.
b1m and 3y retention: Abbreviations for the lipiodol retention at 1 month and 3 years after TACE.
Clinicopathological Characteristics for the 3 Types of HCC in the Surgical Cohort.a

Abbreviations: AFP, alpha-fetoprotein; ALT, alanine aminotransferase; AST, aspartate transaminase; BCLC, Barcelona Clinic Liver Cancer; HBeAg, hepatitis B e antigen; HBsAg, hepatitis B surface antigen; HBV-DNA, hepatitis B virus deoxyribonucleic acid; HCC, hepatocellular carcinoma; MVD, microvessel density; MMVD, maximum microvessel diameter; TBIL, total bilirubin.
an = 108.
bMVD-CD34-400 and MVD-CD34-200: Abbreviations for MVD analyzed by anti-CD34 at high power field of ×400 and ×200.
Association of CT-Based Prognostic Model Type With Pathologically Identified Vascular Features
The surgical cohort was used to investigate the association between the CT-based prognostic model and histopathological findings. As shown in Figure 1B and Table 2, type I HCC had the highest mean MVD (101.5 [33.1] vessels / 0.74 mm2), largest mean MMVD (27.5 [12.2] µm), and smallest intercapillary distance. Moreover, type III HCC had the lowest MVD (21.1 [6.4] vessels/0.74 mm2), smallest MMVD (3.6 [3.0] µm), and largest intercapillary distance. Further analysis showed that MVD and MMVD were significantly associated with tumor enhancement and attenuation on CT scans (Supplementary Figure 3).

The CT prognosis model of the three types of HCC. (A) The CT value enhancement of the three types. (B) Immumohistochemical staining of CD34. (C) Lipiodol retention of the three types of HCC.
Association of CT-Based Prognostic Model Type With Tumor Response to TACE
As shown in Table 1 and Figure 1C, 414 TACE sessions were performed for 195 patients in the TACE cohort, which resulted in 42 (21.5%) CR, 36 (18.5%) PR, 34 (17.4%) SD, and 83 (42.6%) PD outcomes. Moreover, intratumoral lipiodol filling and washout were different between the 3 HCC types.
After a single session of TACE, the CN rate was 13.7% (16/117 patients) in type I HCC, 36.5% (23/63 patients) in type II HCC, and 0% (0/15 patients) in type III HCC, indicating that type II HCC had the highest CN rate at 1 month following the initial TACE treatment (Figure 2A, P < .001). After 3 years, the CN rate was 9.4% (11/117 patients) in type I HCC, 47.6% (30/63 patients) in type II HCC, and 6.7% (1/15 patients) in type III HCC, demonstrating that type II HCC had the highest CN rate (Figure 2B, P < .001). Univariate analysis showed that CT-based prognostic model type, serum alpha-fetoprotein (AFP) level, and tumor size were significant factors of CN (P < .10, Table 3). Multivariate analysis indicated tumor size and prognostic model type were both independent predictors of CN (P < .05, Table 3).

The prognosis associated with the three types and HCC. (A) The CN rate of the three types of HCC after a single session of TACE. (B) The CN rate of the three types of HCC after 3 years. (C) The unprogression rates of the three types of HCC. (D) The survival rates of the three types of HCC.
Univariate and Multivariate Analysis for Independent Factors Associated With CN in the TACE Cohort.a

Abbreviations: AFP, alpha-fetoprotein; ALT, alanine aminotransferase; AST, aspartate transaminase; BCLC, Barcelona Clinic Liver Cancer; CI, confidence interval; CN, complete necrosis; CT, computed tomography; HBeAg, hepatitis B e antigen; HBsAg, hepatitis B surface antigen; HBV-DNA, hepatitis B virus deoxyribonucleic acid; ICN, incomplete necrosis; OR, odds ratio; TACE, transarterial chemoembolization; TBIL, total bilirubin.
an = 195.
Association of CT-Based Prognostic Model Type With Patient Prognosis Following TACE
As shown in Figure 2C, the 1-, 2-, and 3-year disease progression rates following TACE treatment were 77.8%, 85.6%, and 91.7%, respectively, for type I HCC; 52.4%, 62.5%, and 68.8%, respectively, for type II HCC; and 93.3%, 93.3%, and 100.0%, respectively, for type III HCC. Thus, patients with type II HCC had a significantly lower 3-year disease progression rate than patients with type I or III HCC (P < .001 for type I and III HCC). Moreover, patients with type II HCC had significantly better survival rates than those with type I or III HCC following TACE. Univariate and multivariate analyses suggest that prognostic model type could be an independent predictor of survival following TACE treatment (Table 4).
Univariate and Multivariate Analysis for Independent Factors Associated With Patient’s Survival in the TACE Cohort.a

Abbreviations: AFP, alpha-fetoprotein; ALT, alanine aminotransferase; AST, aspartate transaminase; BCLC, Barcelona Clinic Liver Cancer; CT, computed tomography; HBeAg, hepatitis B e antigen; HBsAg, hepatitis B surface antigen; HBV-DNA, hepatitis B virus deoxyribonucleic acid; TACE, transarterial chemoembolization; TBIL, total bilirubin.
an = 195.
Discussion
Based on the enhancement and attenuation characteristics of the tumor blood supply observed with functional CT scans and histopathological confirmation of resected specimens, HCC could be classified into 3 types. Computed tomography-based prognostic model type was closely and independently associated with patient survival following TACE.
Type I HCC, which was characterized by a high MVD and large MMVD, had good intratumoral lipiodol deposition that subsided over time. Patients with type I HCC had a low CN rate following TACE and experienced tumor regrowth with lipiodol diffusion. Type II HCC, which was characterized by moderate MVD and MMVD, had good lipiodol deposition within the tumor. Therefore, patients with type II HCC had a high CN rate and prolonged survival. Type III HCC, which was characterized by a low MVD and small MMVD, had little intratumoral lipiodol deposition. Patients with type III HCC had significantly poorer survival.
The outcome of patients with HCC following TACE has been reported to be largely affected by interactions between embolic materials and tumor vasculature. 11 These interactions, which are affected by the compatibility of embolic particle size and vascular diameter, not only affect the location of embolization within the artery but also change blood flow within the tumor locally. Decreased blood flow and, subsequently, increased blood viscosity result in different absorption rates of embolic agents into the HCC, leading to different effects of chemotherapeutic agents on tumor cells. 17 Large embolic agents affect large proximal hepatic arteries, leading to temporary arterial embolization and rapid development of arterial collaterals, 27 whereas small agents traverse the peribiliary plexus to the portal veins, resulting in a distal and permanent vascular occlusion. 42 Smaller embolic substances (ie, 100-200 µm) that could be effectively trapped in an HCC have therefore been used to embolize the peripheral site of the hepatic artery. 43,44 In our study, when an emulsion of lipiodol and epirubicin was used as an embolic agent, lipiodol embolized tumor microvessels clinically. Using the same lipiodol emulsion, features of tumor vascularity can determine patient outcome following TACE treatment.
Microvessel density is important for delivering chemotherapeutic agents into tumors; however, few studies have provided direct evidence for a relationship between MVD and tumor vascular embolization. 45 A high MVD has been shown to be associated with large tumor size and hypervascularity, 46 -48 which are features associated with good lipiodol retention following TACE. 49 However, our results were different from these previous findings. Type I HCC with a high MVD was associated with MMVD larger than that of the lipiodol emulsion (10-100 µm), which enables lipiodol to enter the vessels and easily permeate or diffuse. 47 However, in this context, ample blood flow washed out intratumoral lipiodol within a few months following TACE. Compared to HCC with a moderate MVD, HCC with a high MVD could not achieve optimal tumor CN following TACE. This may relate to the observation that tumors with high vascularity failed to achieve long-term CN following TACE treatment. Furthermore, in type II HCC with a moderate MVD, which was usually accompanied by a smaller MMVD, the diameter of the lipiodol emulsion was similar to those of the capillaries. In type II HCC, lipiodol did not enter the tumor capillaries as easily as it entered those in type I HCC; however, it was still optimally deposited in the tumor, which resulted in long-term therapeutic effects and a higher rate of CN. In type III HCC with the lowest MVD, which was usually associated with the smallest MMVD, the diameter of the lipiodol emulsion was much greater than those of the capillaries. Therefore, it was difficult for lipiodol to enter the vascular network, which negatively affected the outcome of chemolipiodolization.
Previous studies have reported that the enhancement and attenuation of HCC on functional CT scans may be related to MVD status. A high MVD was associated with increased peak enhancement and quick attenuation. 24,45,49 These results were consistent with our findings in type I HCC. However, this study also found different results from those in the literature. Specifically, type III HCC with the lowest MVD presented almost no enhancement. Moreover, type II HCC with a moderate MVD presented enhancement in the arterial phase, although at a relatively lower rate, and almost no attenuation in the late phase. This may be attributed to different tumor features, including portal vein blood supply, capillary permeability, or arterioportal communication (peribiliary plexa). 42
Multiple factors, such as tumor load and liver function, have been shown to correlate with patient survival. In this study, neither albumin nor bilirubin, 2 predictors of the hepatoma arterial-embolization prognostic score, was found to be an independent factor in univariable and multivariable analyses. 12 These findings did not exclude liver function from being an important predictor for survival following TACE, but indicated that, in the context of patients with good liver function, tumor vascularity—a trait assessed in this study using CT scans—was the most important predictor for survival.
Our study had some limitations. The feasibility of using our prognostic model for predicting HCC outcome following alternative TACE treatments remains to be determined. Although this study provided some evidence for a correlation between tumor vascularity and lipiodol uptake, the mechanisms of lipiodol uptake and its long-lasting intratumoral retention remain to be explored. A separate HCC cohort of patients who underwent liver resection was also included in our study since pre- and post-TACE tumor specimens were of limited availability in our clinic. Post-TACE tumors usually had massive necrosis and significant vascular proliferation. Consequently, it was difficult to determine changes in tumor vascularity in patients treated with TACE following surgery or with TACE alone.
In summary, the CT-based prognostic model for HCC proposed in this study reflects HCC characteristics and could be a useful tool for predicting the survival of patients with HCC following chemolipiodolization treatment. Patients with type II HCC are likely to achieve better survival outcomes compared to those with type I or III HCC following chemolipiodolization treatment.
Supplemental Material
Supplemental Material, Supporting_information_for_online_publication_only - A Pretreatment CT Model Predicts Survival Following Chemolipiodolization in Patients With Hepatocellular Carcinoma
Supplemental Material, Supporting_information_for_online_publication_only for A Pretreatment CT Model Predicts Survival Following Chemolipiodolization in Patients With Hepatocellular Carcinoma by Yijun Zhang, Shuping Qu, Wanwan Yi, Jian Zhai, Xiaobing Zhang, Lixin Wei, Wan Yee Lau, Mengchao Wu, Feng Shen, Hengwei Fan and Dong Wu in Technology in Cancer Research & Treatment
Footnotes
Authors’ Note
Our study was approved by the Ethical committee of biomedicine research, second military medical university (approval no. EHBHKY2012-002-12). All patients provided written informed consent prior to enrollment in the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: This study was supported by grants of the State Key Project on Infectious Diseases of China (2012ZX10002-016 to F.S.), National Natural Science Foundation of China (81672718 to F.S.), and Shanghai Hospital Development Program (SHDC12013111, 12014210 to D.W.).
Supplemental Material
Supplemental material for this article is available online.
Abbreviations
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.