
Abstract
Purpose/Objective:
Reproducible patient positioning remains one of the major challenges in modern radiation therapy. Recently, optical surface scanners have been introduced into clinical practice in addition to well-established positioning systems, such as room laser and skin marks. The aim of this prospective study was to evaluate setup errors of the optical surface scanner Catalyst HD (C-RAD AB) in different anatomic regions.
Material/Methods:
Between October 2016 and June 2017 a total of 1902 treatment sessions in 110 patients were evaluated. The workflow of this study included conventional setup procedures using laser-based positioning with skin marks and an additional registration of the 3-dimensional (3D) deviations detected by the Catalyst system. The deviations of the surface-based method were then compared to the corrections of cone beam computed tomography alignment which was considered as gold standard. A practical Catalyst setup error was calculated between the translational deviations of the surface scanner and the laser positioning. Two one-sided t tests for equivalence were used for statistical analysis.
Results:
Data analysis revealed total deviations of 0.09 mm ± 2.03 mm for the lateral axis, 0.07 mm ± 3.21 mm for the longitudinal axis, and 0.44 mm ± 3.08 mm vertical axis for the Catalyst system, compared to −0.06 ± 3.54 mm lateral, 0.53 ± 3.47 mm longitudinal, and 0.19 ± 3.49 mm vertical for the laser positioning compared to cone beam computed tomography. The lowest positional deviations were found in the cranial region, and larger deviations occurred in the thoracic and abdominal sites. A statistical comparison using 2 one-sided t tests showed a general concordance of the 2 methods (P ≤ 0.036), excluding the vertical direction of the abdominal region (P = 0.198).
Conclusion:
The optical surface scanner Catalyst HD is a reliable and feasible patient positioning system without any additional radiation exposure. From the head to the thoracic and abdominal region, a decrease in accuracy was observed within a comparable range for Catalyst and laser-assisted positioning.
Introduction
In modern radiation oncology, the term “image-guided radiation therapy (IGRT)” refers to the use of various imaging methods to correct possible setup errors in patient position. In fact, the reproducibility of patient setup and organ motion management remains one of the major challenges in the daily clinical activities of radiation therapy. 1 Technological improvements of recent years, including the introduction of cone beam computed tomography (CBCT), have significantly improved precise dose delivery to the tumor and minimized uncertainties. Image-guided technology is not only used to better assess the position of the target during the treatment; advanced IGRT techniques enable clinicians to perform dose escalation to tumor volumes near surrounding sensitive organs at risk, and this approach was the cornerstone of stereotactic radiotherapy. 2,3 In addition, the implementation of daily IGRT can minimize setup margins for treatment planning volumes, which can potentially reduce side effects by maintaining high local tumor control rates. 4 -6
However, the correct initial positioning of the patient remains a crucial issue for accurate IGRT protocols. In cases of major deviations in the patient’s treatment position, even a precise IGRT realignment cannot perfectly compensate for substantial anatomical divergences. Excluding CBCT, a number of other IGRT techniques are currently available, such as fiducial markers inside the target volume monitored by portal imaging, ultrasound systems, or electromagnetic online verification with microprobes in the patient’s body. More recently, newly developed optical surface positioning systems have been introduced into clinical practice. 7,8 Optical systems have been investigated over a long period of time, but it was only after the development of powerful central processing units that these tools could be further developed into accurate, high-resolution sensors. 8 Nowadays, surface-based systems enable a continuous and touchless optical surface scanning of the patients’ external surfaces and are a helpful tool for accurate patient positioning in 6 degrees of freedom without any additional radiation exposure. Furthermore, many commercial systems offer other features, including visual user assistance in the identification of positioning deviations, intrafractional motion control, and automated respiratory gating, especially in the context of deep inspiration breath hold. 9
As an example, optical tracking systems like AlignRT (Vision RT Ltd, London, United Kingdom) used as positioning system could show to be more accurate than laser positioning in patients with whole breast or chest wall irradiation. 10,11
In this study, the Catalyst HD optical surface scanner produced by C-RAD (Uppsala, Sweden) was analyzed for patient positioning and compared to the clinical gold standard consisting of manual positioning using skin marks and CBCT.
Material and Methods
This study was designed as a prospective observational study and data collection was performed between October 2016 and June 2017. The study was approved by the local ethics committee of the University Hospital, LMU Munich (No. 352-16 ex 09/2016) and registered at German Clinical Trials Register (DRKS-ID: DRKS00011407). Written informed consent was obtained from all patients.
Optical Scanner System Catalyst HD
The optical surface scanner Catalyst HD from C-RAD consists of 3 ceiling-mounted scanner units and the associated c4D-software. The scanners in the linac room are arranged at an angle of around 120° to each other in order to enable a continuous detection of the surface even if the gantry is rotating around the patient (Figure 1). During the scan, the device emits visible light with a wavelength of 405 nm (blue) and reprojections are captured by integrated charge-coupled device cameras. The comparison of the surface scan with an initially acquired reference scan is based on the principles of photogrammetry through optical triangulation and is carried out via a nonrigid iterative closest point algorithm in 6 degrees of freedom (lateral, longitudinal, vertical, rotation, roll, and pitch). The scan field size is 800 mm × 1300 mm × 700 mm with a maximum frame rate of 200 Hz. The camera settings include an editable integration time and gain factor as well as specific presets (concerning tolerances and averaging times) for different treatment sections.

The 3 Catalyst HD scanners in the treatment room. The scanners are arranged at an angle of 120° to each other in order to enable a continuous detection of the surface even if the gantry is rotating around the patient.
In addition, the system also features integrated light-emitting diode (LED) projectors for projecting positional deviations onto the patient’s surface to assist in patient positioning. For different deviations, different colored light (green: 528 nm, red: 624 nm) is used to visualize the reference position on the patient surface. An example is shown in Figure 2.

Positional deviations projected onto the patients’ surface (screenshot of Catalyst software c4D [C-Rad AB). Local deviations outside the tolerance limits compared to the reference scan are marked in red.
Workflow
During the first treatment session, the patient was initially aligned using a CBCT scan (X-ray volume imaging by Elekta AB, Stockholm, Sweden) as a gold standard. Subsequently, the isocenter was marked using skin marks via the positioning lasers. In addition, a reference surface scan for repeatable patient setup during the course of the following fractions was created using the Catalyst scanner, which took less than an additional minute.
According to the study protocol, during the following treatment sessions, the patients were first positioned via the room laser and skin marks. Thereafter, a Catalyst surface scan was carried out and the shift values in regard to the optimal treatment position (Catalyst reference scan) were recorded. Finally, a CBCT was acquired, in which deviations were regarded as gold standard. The final alignment of the patient prior to dose delivery was always carried out on the basis of the CBCT. Cone beam computed tomography registration was done automatically or in a standardized manner following specific IGRT standard operating procedures to reduce interuser deviations. Nevertheless, the deviations recorded for laser-based and catalyst-based positioning were correlated with the CBCT of the same treatment session, and interuser deviations would therefore be of minor importance. The daily workflow is depicted in Figure 3. If new skin marks were needed during the treatment course, a new Catalyst reference scan was created.
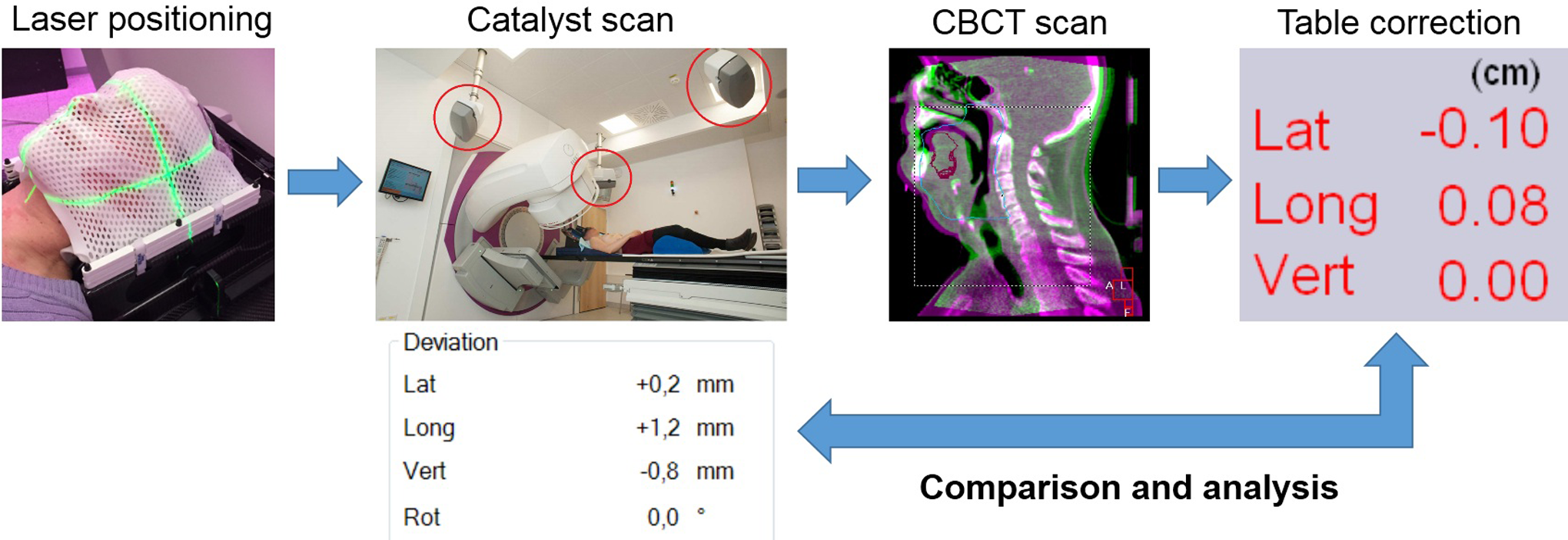
Daily workflow.
Statistics
The shift values determined by the Catalyst system and the CBCT in regard to laser-based positioning were recorded in 3 spatial levels for each treatment fraction. Treatment fractions where no CBCT was acquired were excluded from the analysis. Furthermore, in order to compare the systems, the deviation of the Catalyst measurements to the CBCT was determined using the following formula:

The measurements were analyzed with regard to the distribution of values, common tendencies, standard deviations, ranges, and deviations overall and reported separately according to treatment regions. In order to statistically compare the 2 methods, the equivalence was tested via 2 one-sided t tests. This test was used to analyze whether the difference in the deviations was within a certain range (head: 0.5 mm; thorax: 1.0 mm; abdomen: 1.5 mm; extremities: 2.0 mm). Hypothesis testing was also performed separately for the different treatment regions. The significance level was set as α = 0.05. Statistical testing was performed using SPSS (IBM Corp. Released 2016. IBM SPSS Statistics for Windows, Version 24.0. Armonk, New York: IBM Corp.) and XLSTAT (XLSTAT: Data Analysis and Statistical Solution for Microsoft Excel. Addinsoft, Paris, France) for the 2 one-sided t tests.
Results
A total of 1902 treatment fractions of 110 patients (66 males, 44 females) were recorded between October 2016 and July 2017. The average patient age was 65 years (range: 31-93). The most common tumor sites included 16 lung tumors, 15 prostate cancers, 14 intracranial tumors, 14 soft tissue sarcomas, and 14 head and neck tumors. For further analyses, the fractions were subdivided into the 4 treatment regions: head, thorax, abdomen, and extremities. In total, data from 689 fractions of the head region, 460 fractions of the thorax, 630 fractions of the abdomen, and 123 fractions of the extremities were evaluated.
For all treatment regions evaluated together, the mean deviation recorded by the Catalyst system was 0.09 ± 2.03 mm in the lateral axis, 0.07 ± 3.21 mm in the longitudinal, and 0.44 ± 3.08 mm in the vertical direction. In contrast, the deviation of the laser-based positioning in regard to the CBCT was −0.06 ± 3.54 mm lateral, 0.53 ± 3.47 mm longitudinal, and 0.19 ± 3.49 mm vertical. As a result, the practical Catalyst error according to the given formula above including all data samples was in mean 0.15 ± 4.21 mm in the lateral direction, −0.46 ± 4.47 mm in the longitudinal, and 0.25 ± 4.54 mm in the vertical axis. The distribution of the divergences is described in Figure 4. A detailed comparison between the 2 methods regarding each treatment region is shown in Table 1 and Figure 5. Overall, both methods showed similar results within a comparable range and with appropriate clinical accuracy. From the head to the thoracic and the abdominal region, an increase in the average deviation and decrease in the precision was observed for both, the Catalyst as well as the laser-based positioning. We observed an increase in mean values and standard deviations from the head (eg, δCatalyst long 0.17 ± 2.11 mm/δLaser long 0.29 ± 1.89 mm) toward the abdominal region (δCatalyst long 1.99 ± 5.25 mm/δLaser long 1.56 ± 4.18 mm). Statistical equivalence testing confirmed this and showed a concordance between the 2 methods within the predefined test limits (P < 0.036; Table 2). One exception was the vertical axis of the abdominal region (P = 0.198), where the absolute Catalyst deviations were slightly closer to the CBCT correction value as compared to the laser-based positioning (mean of −0.59 mm vs 0.68 mm).

Histograms showing distributions of Catalyst and laser deviations along all 3 spatial directions.
Catalyst and Spatial Laser Deviations Sorted by Region.

Abbreviations: CI, confidence interval; SD, standard deviation; lat., lateral; long., longitudinal; vert., vertical.

Catalyst and laser deviations sorted by region along the 3 directions.
Two One-Sided t Tests for Equivalence Results (P Value) Sorted by Region and Spatial Axes.

Abbreviation: CI, confidence interval.
Discussion
Different optical systems have been evaluated for patient positioning in phantom studies or in different clinical settings. 12 -22 Concerning the general strengths and weaknesses of optical systems, in most of these experiences, similar conclusions were reported. In addition to the lack of ionizing radiation, optical systems reach their maximum potential in terms of reliability, especially in regions with a fixed tumor to surface correlation.
Although the Catalyst system is currently used for patient positioning in several radiation oncology departments, there is limited evidence of its actual reliability and accuracy in daily clinical practice. In a recent retrospective study, Stanley et al evaluated approximately 6000 fractions. 23 The patients were initially positioned either via skin marks and spatial lasers or via the Catalyst system. The authors reported an average vector deviation of 5 to 6 mm for Catalyst and 9 to 14 mm for room lasers, depending on the anatomic district. The authors concluded that Catalyst was a reliable alternative to conventional positioning via skin marks and room lasers and was able to further optimize initial patient positioning. One drawback is the retrospective design of this study. In contrast to the present prospective study, patient alignment was performed either by the optical system or by the laser-based system and compared retrospectively to CBCT scans. One of the strengths of the present analysis is that we followed a standardized workflow and compared the optical scan of the same treatment session to the laser-based positioning in order to avoid intrafractional uncertainties.
Recently, the positioning accuracy using absolute median values of Catalyst and laser positioning for patients with rectal cancer has been compared: A significant difference was only observed in the lateral direction for the benefit of the Catalyst system with a median positioning accuracy of 1.3 cm versus 2.0 cm for the laser, and longitudinal and vertical direction did not show any performance differences between the 2 methods. 24
An early study of our department retrospectively compared the Catalyst system to spatial laser positioning. 25 A total of 154 treatment fractions of about 25 patients treated in the region of the thorax, abdomen, and pelvis were retrospectively evaluated. Positioning using skin marks resulted in deviations of 0.0 ± 2.1 mm laterally, −0.4 ± 2.4 mm longitudinally, and 1.1 ± 2.6 mm vertically. The error calculated for the Catalyst was −0.1 ± 2.1 mm lateral, −1.8 ± 5.4 mm longitudinal, and 1.4 ± 3.2 mm vertical. A statistical analysis showed only one significant difference between the 2 methods in the longitudinal axis of the pelvic area. In our setting, we were able to reproduce the good precision of the laser-based positioning and obtained deviations of similar proportions for both systems. Despite the very similar design of the study, the standardized workflow, the larger cohort of patients, and the greater number of analyzed fractions could result in better results.
In a recent clinical report by Crop et al, the Catalyst system was compared to positioning by spatial laser and a mega voltage computed tomography (MVCT) using TomoTherapy (Accuray, Sunnyvale, California). 26 The study included mainly patients with breast cancer. Interuser dependent MVCT deviations as well as intrafractional patient movements were measured in order to include the human factor as well as the timing component in the system’s evaluation. The authors concluded that Catalyst was superior to the spatial laser in terms of positioning capabilities and was not significantly inferior to the MVCT. Specifically, the shorter time interval between scan and repositioning was described as a major advantage of the optical system, since the largest increase in random patient movements was recorded within the first 5 minutes after positioning. Similarly, the interuser dependent variation in manual MVCT matching was seen as an important factor influencing accuracy.
More recently, Ma et al used an Optical Surface Management System in breast cancer radiotherapy for interfractional patient positioning measurements compared to CBCT. As a conclusion, the 2 systems did not show any difference for all 3 possible spatial axes. 27
Stieler et al evaluated a direct comparison between the Catalyst system and patient positioning using CBCT. 28 In the clinical part of the study, 224 fractions of 13 patients with treatments of the head/neck, thorax, and abdomen were evaluated. The authors reported deviations of the Catalyst system of 0.7 ± 2.8 mm lateral, −1.3 ± 4.0 mm longitudinal, and 1.5 ± 3.6 mm vertical across all regions. Overall, a good correlation between the results of the 2 methods, especially in the case of tumor entities with a fixed tumor-to-surface relationship, was described. However, it also emphasizes the dependence of the results on the correct camera settings for good image quality.
With regard to this study, patient positioning using Catalyst was reliable in all clinical situations. Compared to laser positioning which is a more or less focusing on several target points, an advantage of this surface scanner is the observation of a larger body surface area in form of a 3D image (Figure 2). Together with optical LED reprojection, it can highlight body areas that exceed position tolerance limits compared to a reference image in real time which facilitates patient positioning in everyday clinical workflow. Additionally, no skin marks are necessary for using surface scanning, which is more patient-friendly and saves time for skin marks drawing/redrawing for the clinical staff. Although surface scanning is unlikely to replace X-ray imaging if the target volume is not close to the surface, the data presented here indicate sufficient accuracy for daily use. In our setup, patient positioning using Catalyst achieved at least the same precision as positioning using spatial laser. The relatively high precision of laser-based positioning through well-trained staff has already been highlighted in a previous study of our institution. 25 The highest precision of the optical system was achieved in scans of the head area, which is presumably due to the relatively narrow tumour to surface correlation and obviously due to the rigid fixation with immobilizing masks. The positioning accuracy in the thoracic and abdominal areas decreased compared to the head area but remained comparable to laser-based positioning with average deviations within the range of a few millimetres. As already assumed by other authors, breathing movements and the resulting motion of internal organs, as well as the symmetric body shape along the longitudinal axis, might be responsible for the deviations of the optical system in comparison to CBCT. 29 Likewise, the variable position of internal organs due to different levels of bladder/bowel fillings can influence external surface positioning and can thus be regarded as an influencing factor for the precision of the optical systems. 17,30,31
Conclusion
In conclusion, the optical surface system Catalyst HD is a reliable and feasible patient positioning system without any additional radiation exposure. From the head to the thoracic and abdominal region, an increase in the average deviation and a decrease in precision were observed within a comparable range for Catalyst and laser-assisted positioning based on the used gold standard (CBCT).
Footnotes
Authors’ Note
G.C. and D.R. contributed equally to this study. G.C. performed data extraction, the statistical analysis, and drafted the manuscript. D.R. supervised and helped with statistical analysis and to write the manuscript. S.S., M.P., M.N., U.G. reviewed the manuscript. S.C. and A.F. helped to finalize the manuscript. P.F. and M.R. planned and organized the technical settings. C.B. and S.C. designed and supervised the study. All authors read and approved the final manuscript. The study was approved by the local ethics committee of the University Hospital, LMU Munich (No. 352-16 ex 09/2016) and registered at German Clinical Trials Register (DRKS-ID: DRKS00011407). Written informed consent was obtained for all patients.
Acknowledgments
The authors would like to thank C-RAD for their assistance during this project.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: C. B., P. F. received research grants and M. R., S. C. speaker honoraria from C-RAD.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for research with the Catalyst System has been received from C-RAD. C-RAD was not involved and had no influence on the study design, the collection, analysis or interpretation of data, on the writing of the manuscript, or the decision to submit the manuscript for publication.