
Abstract
Background:
Diabetic retinopathy (DR) is a leading cause of blindness; however, many patients with type 2 diabetes (T2DM) are not up to date with screening guidelines. This study explored the impact of teleretinal screening bulk orders on the DR screening completion rate.
Methods:
In this randomized controlled trial, eligible patients with T2DM due for DR screening were randomly assigned to receive a teleretinal screening bulk order at one of four monthly time points, following a stepped-wedge design. Teleretinal screening bulk orders are placed by a centralized provider for a defined patient cohort. They include a retinal fundus photo order and an associated electronic patient education message. Logistic regression at the patient-month level, with errors clustered at the patient level, was used to evaluate the effect of bulk orders on DR screening completion rate. Two-stage least squares was used to evaluate the effects of opening the message, using random assignment as an instrument.
Results:
A total of 5,665 eligible patients were identified for this study. At six months from the first bulk order, the overall DR screening completion rate was 17.5% (n = 994). Receiving a bulk order increased odds of completing screening (odds ratio [OR]: 1.78; confidence interval [CI] 95%: 1.49, 2.14; p < 0.001). 2,763 patients (48.7%) opened the electronic patient message. Opening the message increased completion rates by 8.5% (95% CI; 6.0%, 11.1%; p < 0.001) and retinal fundus photo appointments scheduled by 19.1% (95% CI; 16.8%, 21.3%; p < 0.001).
Conclusion:
Teleretinal screening bulk orders were associated with a significant increase in DR screening. Population-level interventions should be implemented to improve diabetes preventative care.
Introduction
Diabetic retinopathy (DR) is the leading cause of blindness in working-aged adults.1–2 The American Diabetes Association recommends an initial eye exam in all people with type 2 diabetes (T2DM) shortly after diagnosis and then annually for those with minimal DR and every 1–2 years for those with no DR. 3 Detecting DR early allows for vision-saving treatment. Despite this, less than half of patients with T2DM are up to date with recommended screening guidelines. 4 Barriers to completing recommended screening include lack of patient knowledge, constraints on providers’ time, inadequate referral rates, and limited access to care.5–7
DR teleretinal screening programs have been implemented in several single-center institutions, showing efficacy in increasing access to care.6,8–12 Teleretinal screening uses specialized retinal cameras to capture images of the back of the eye, which are then sent to an optometrist or ophthalmologist to review. In our large multipayer academic health care system, retinal fundus cameras are available at multiple outpatient sites colocated in primary care and endocrinology clinics. Patients can self-schedule retinal screening appointments through their electronic health record (EHR) patient portal once a retinal fundus photo order is placed by a physician. However, even with a teleretinal screening system in place, overall screening adherence at our institution has remained below the National Committee for Quality Assurance’s targets for the Healthcare Effectiveness Data and Information Set measurement. 13
Preventative screening and chronic disease management in the United States often involves individual physicians placing orders during a patient encounter. Competing constraints on physician time, lack of knowledge by patients, and issues securing appointments result in significant barriers.14,15 Proactive population-based approaches are needed to ensure patients receive recommended care. 16 Strategies that allow for asynchronous care in collaboration with the outpatient provider have shown to be effective in increasing screening rates for colorectal cancer.17,18 This suggests an opportunity to implement similar screening programs for preventative diabetes care.
In this quality improvement (QI) trial, a population-based EHR intervention was implemented using teleretinal screening bulk orders. “Bulk orders” are defined protocols used by our Office of Population Health and Accountable Care (OPHAC) and Quality Improvement (QI) team to place health screening orders in bulk alongside automated electronic patient messages for defined patient populations. Bulk orders have been utilized in other outpatient applications; however, this intervention focused on their use in improving preventative diabetes care. This study aimed to determine the impact of teleretinal screening bulk orders on the annual DR screening completion rates for empaneled adult patients with T2DM.
Methods
STUDY DESIGN
This stepped wedge randomized controlled QI trial was conducted from February 2022 to October 2022 in a large, integrated academic health system with an existing teleretinal screening program. From January 2019 to August 2021, six teleretinal screening locations colocated in outpatient primary care and endocrinology clinics opened. In January 2022, a direct scheduling mechanism was launched that allowed patients who had an active retinal fundus photo order placed by a provider to self-schedule an appointment in their EHR patient portal. Eligible patients due for DR screening in February 2022 were identified by our OPHAC. Simple randomization into one of four monthly teleretinal screening bulk orders (April–July 2022) following a stepped-wedge design was done on all eligible patients (Fig. 1). The treatment group was defined as patients who had received a bulk order, and the control group was defined as patients who had not yet received a bulk order. Randomization into four groups ensured scheduling availability for retinal fundus photo appointments within 4 weeks of receiving a bulk order. All eligible patients received a bulk order and transitioned from the control group to the treatment group.
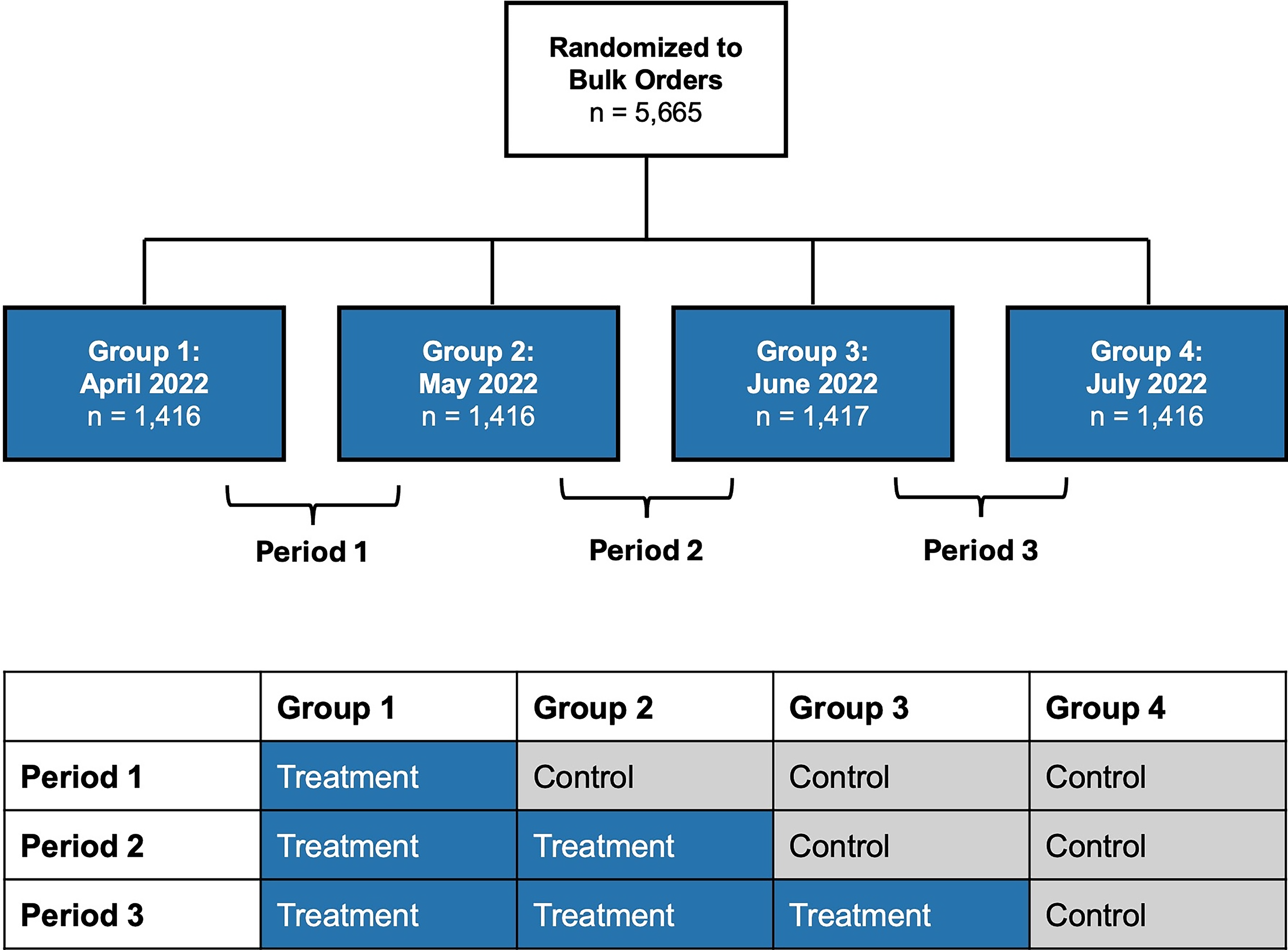
A stepped-wedge design simple randomization was used to randomize all eligible patients into one of four bulk order groups. Periods were defined as the time between each bulk order group. A stepped-wedge design was used; patients transitioned from the control group to the treatment group as they received a teleretinal screening bulk order.
Teleretinal screening bulk orders included orders for a retinal fundus photo and an associated electronic patient education message with information about DR screening recommendations, locations of the retinal cameras, how to schedule a retinal fundus photo appointment through the patient portal, and how to notify their provider if screening was completed outside the health system. Bulk orders were placed by a centralized provider associated with the Department of Medicine Quality Program. The DR screening care gap was automatically closed within our health system’s EHR after patients’ retinal fundus photos were read and finalized by an optometrist or ophthalmologist, and the results were reviewed by the patients’ attributed providers.
PATIENT POPULATION
The OPHAC at our institution manages a diabetes dashboard that incorporates EHR data, billing data, and claims data, which was used to identify eligible patients. Patients with T2DM, aged 18–70, due for DR screening, who had an active patient portal, and had an attributed primary care provider were included. Patients were excluded if they had a history of DR, an active referral to ophthalmology, an active retinal fundus photo order, an ophthalmology appointment within the last year, or had opted out of receiving messages (Fig. 2).
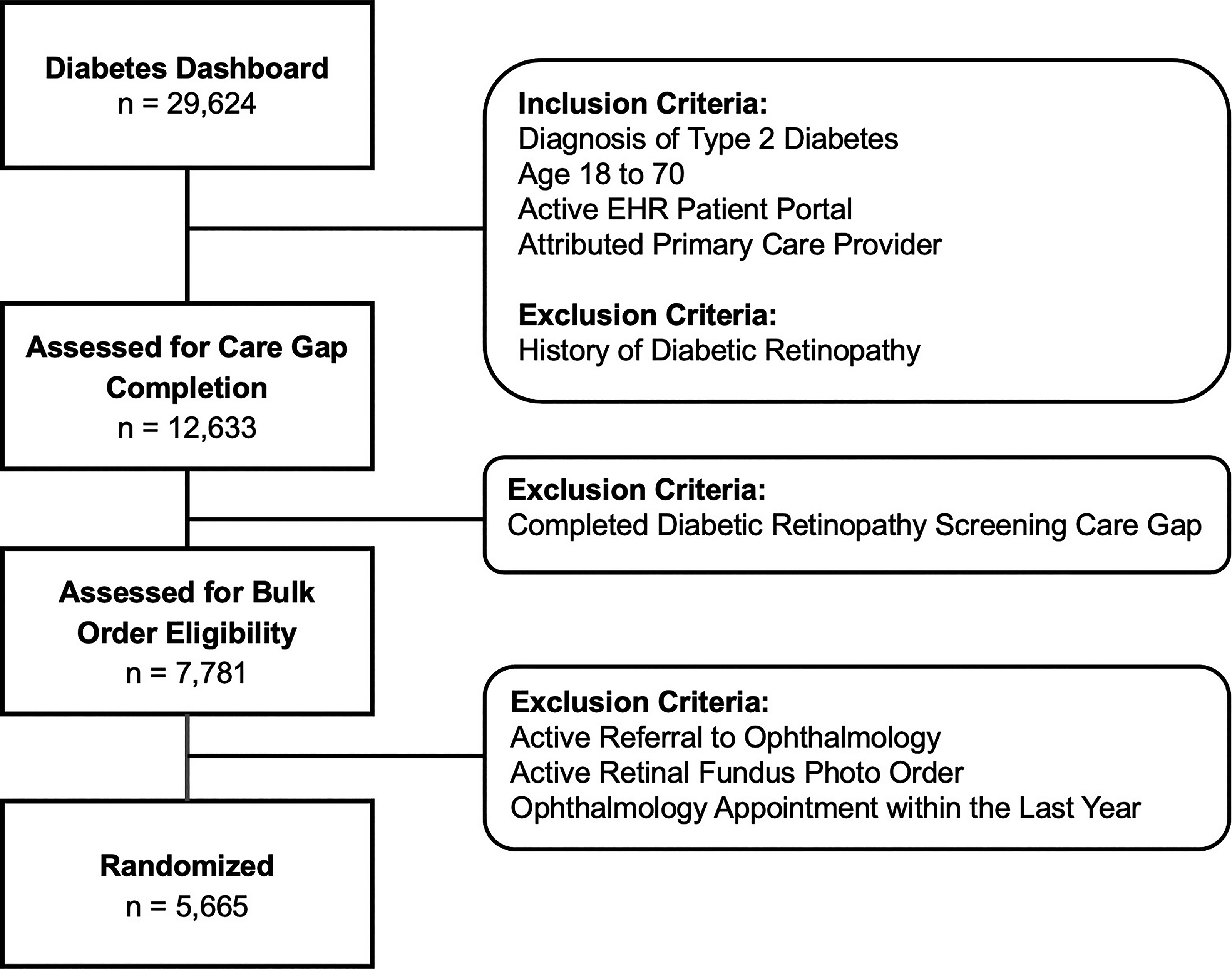
Flow diagram for study participants.
OUTCOMES AND VARIABLES
The primary outcome measure was overall annual DR screening completion rate through care gap closure within the EHR Health Maintenance portal. Care gap completion was defined either within our health system (completed retinal fundus photo or dilated eye exam) or at an outside facility (provider marks the care gap as complete after review of outside records or based on patient reporting of eye exam completion within the last year).
Secondary outcome measures included rates of associated electronic patient message opening, scheduled retinal fundus photo appointments, and completed retinal fundus photo appointments. Other study variables included age, sex, race, ethnicity, attributed provider clinic, insurance type, A1c, and social vulnerability index. All measures were obtained from reports created using the diabetes dashboard by our OPHAC team. Reports were generated monthly, and a final study endpoint of October 2022, 6 months after the first bulk order date, was used.
STATISTICAL ANALYSIS
Descriptive statistics were used to summarize patient characteristics by random assignment. Logistic regression was performed at the patient-month level to evaluate the effect of the bulk order intervention on completion of annual DR screening. The primary model terms were intervention status (bulk order vs. control) and time period (April vs. May vs. June vs. July). Models adjusted for age, sex, race, ethnicity, payor, last hemoglobin A1c, and social vulnerability index (SVI). Inferences were performed using cluster-robust standard errors at the patient level to account for repeated assessment of each patient. A two-sided significance level of 0.05 was used. The primary analysis followed the intention-to-treat principle. Secondary analyses of the effects of opening the message were performed using two-stage least squares, utilizing random assignment as an instrumental variable. Kaplan–Meier curves were used to assess time to message opening and appointment scheduling. Analyses were performed using SAS v. 9.4 (SAS Institute Inc., Cary, NC).
ETHICS STATEMENT
Our study was designed to meet Standards for QI Reporting Excellence criteria. The University of California, Los Angeles Institutional Review Board determined that this QI intervention did not meet the definition of human subjects research as defined by federal regulations for human subject protections 45 CFR 46.102(I); therefore, neither certification of exemption nor Institutional Review Board (IRB) approval was required.
Results
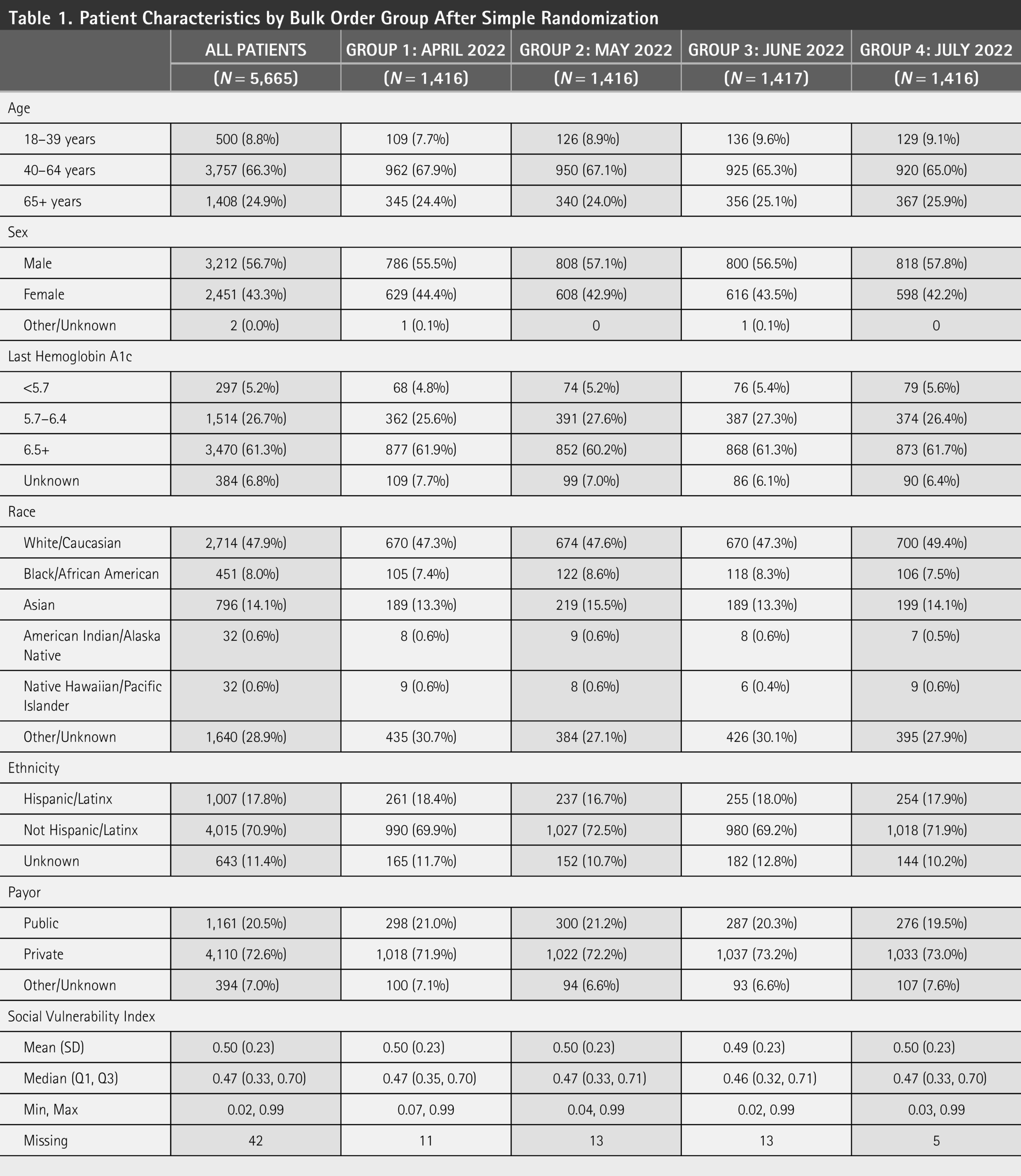
There were 5,665 patients (2,451 women [44.3%]; 3,757 aged 40–64 [66.3%], and 3,470 with last recorded hemoglobin A1c ≥6.5% [61.3%]; Table 1). Patients were predominantly White (n = 2,714; 47.9%), not Hispanic (n = 4,015; 70.9%), and had private insurance (n = 4,110; 72.6%). Baseline patient characteristics were similar in all four bulk order groups.
Patient Characteristics by Bulk Order Group After Simple Randomization
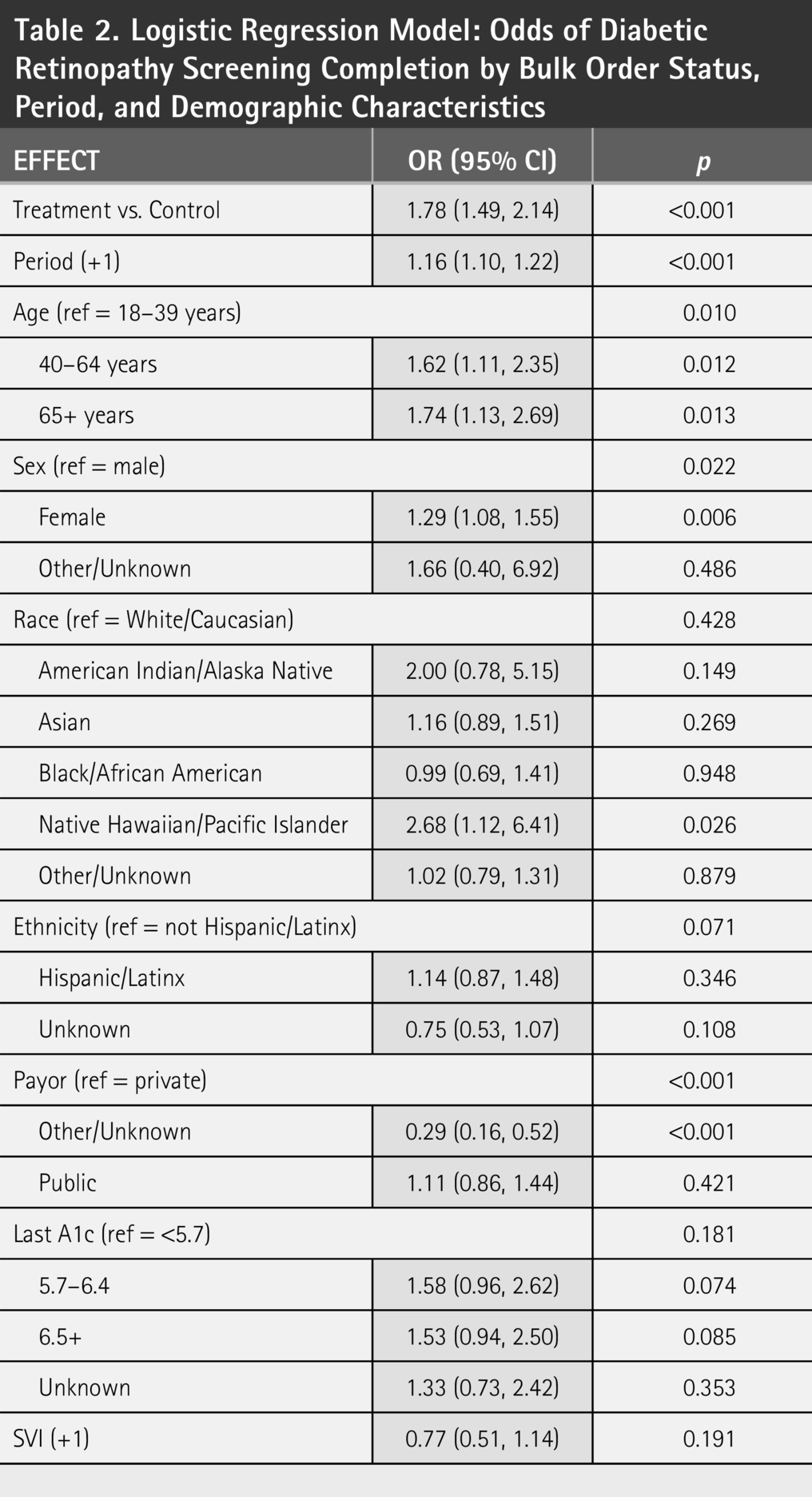
Receiving a bulk order was associated with increased DR screening completion with an odds ratio of 1.78 (1.49, 2.14; Table 2 and Fig. 3). At the end of the study, which was 6 months after the first bulk order date, the screening completion rate for all patients was 17.5% (n = 994). A little less than half (48.7%) of patients (n = 2,763) opened the electronic patient message associated with the bulk order. The median days from when the messages were sent to opening was 0.1 days (Q1 0.0 and Q3 2.0; Fig. 4). In total, 13.6% of patients (n = 775) scheduled an appointment for a retinal fundus photo. Of appointments scheduled, 578 appointments (74.5%) were completed at the end of the study. In total, 13.0% of appointments (n = 101) were scheduled within 24 h of receiving the teleretinal screening bulk order (Fig. 5). The median number of days until scheduled retinal fundus appointment from receiving the bulk order was 79 days (Q1 42.5, Q3 108.0). Opening of the electronic message was associated with an increase in DR completion rate of 8.5% (95% CI: 6.0%, 11.1%; p < 0.001) and in scheduled retinal fundus photo appointments of 19.1% (95% CI: 16.8%, 21.3%; p < 0.001).
Logistic Regression Model: Odds of Diabetic Retinopathy Screening Completion by Bulk Order Status, Period, and Demographic Characteristics
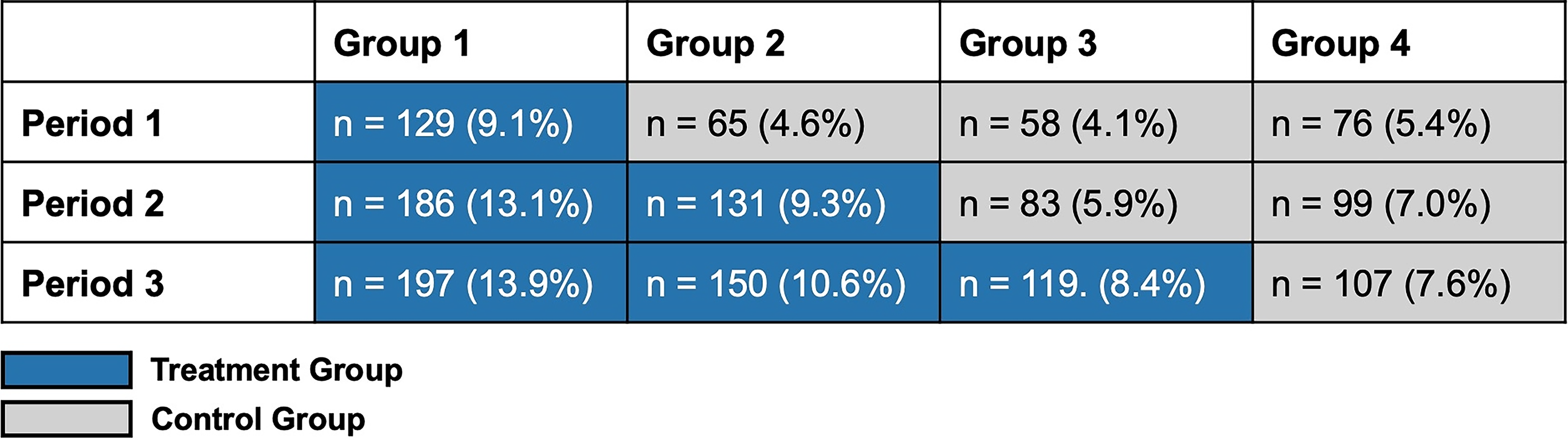
DR screening completion by bulk order group and period. The figure shows DR screening completion rate by bulk order group and period. n = number of patients in the bulk order group that have completed DR screening. DR, diabetic retinopathy.
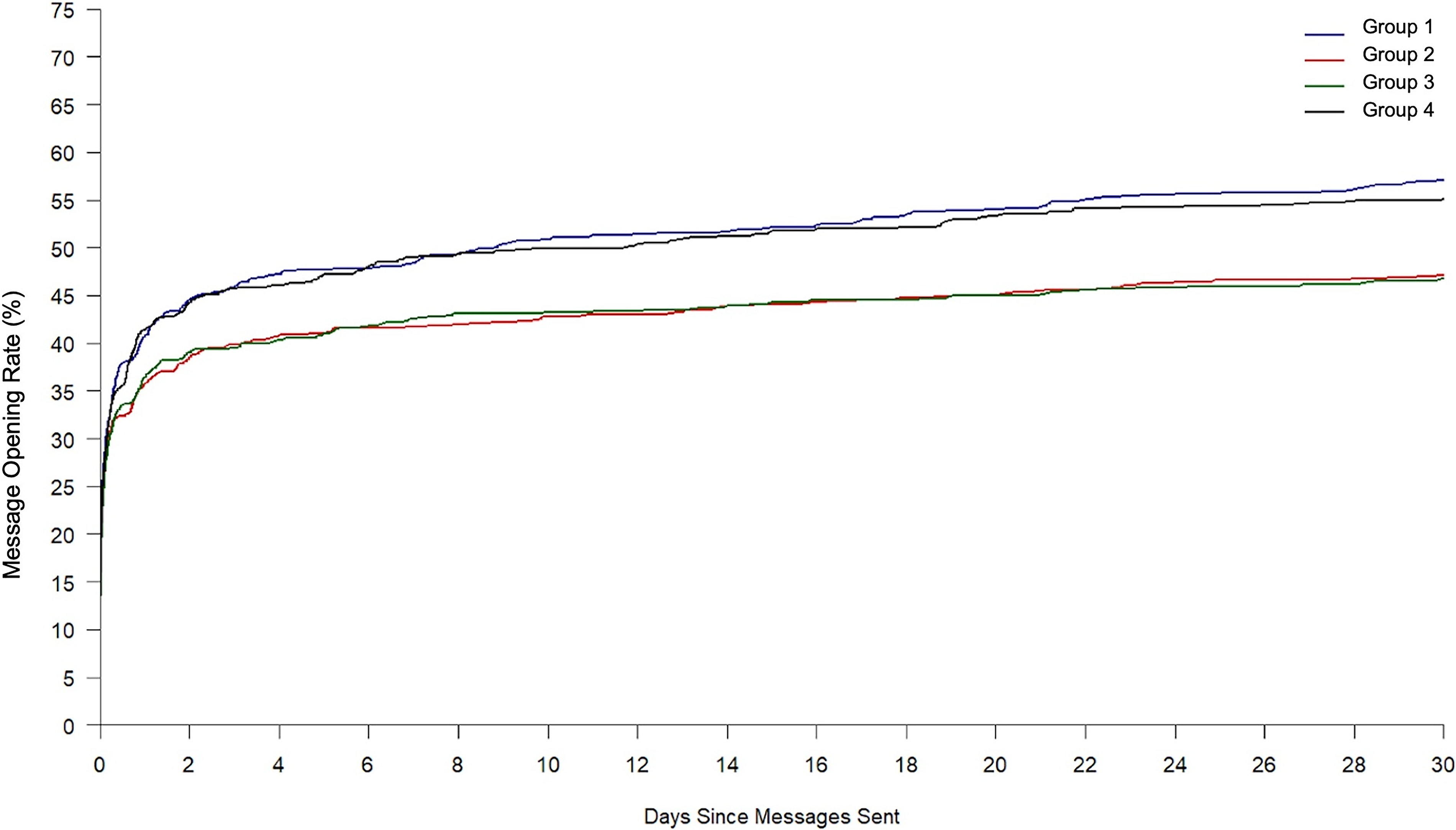
Patient message open rate by bulk order group Kaplan–Meier curves for rates of electronic patient message opening according to bulk order group, with the interval in days since the bulk order message was sent.
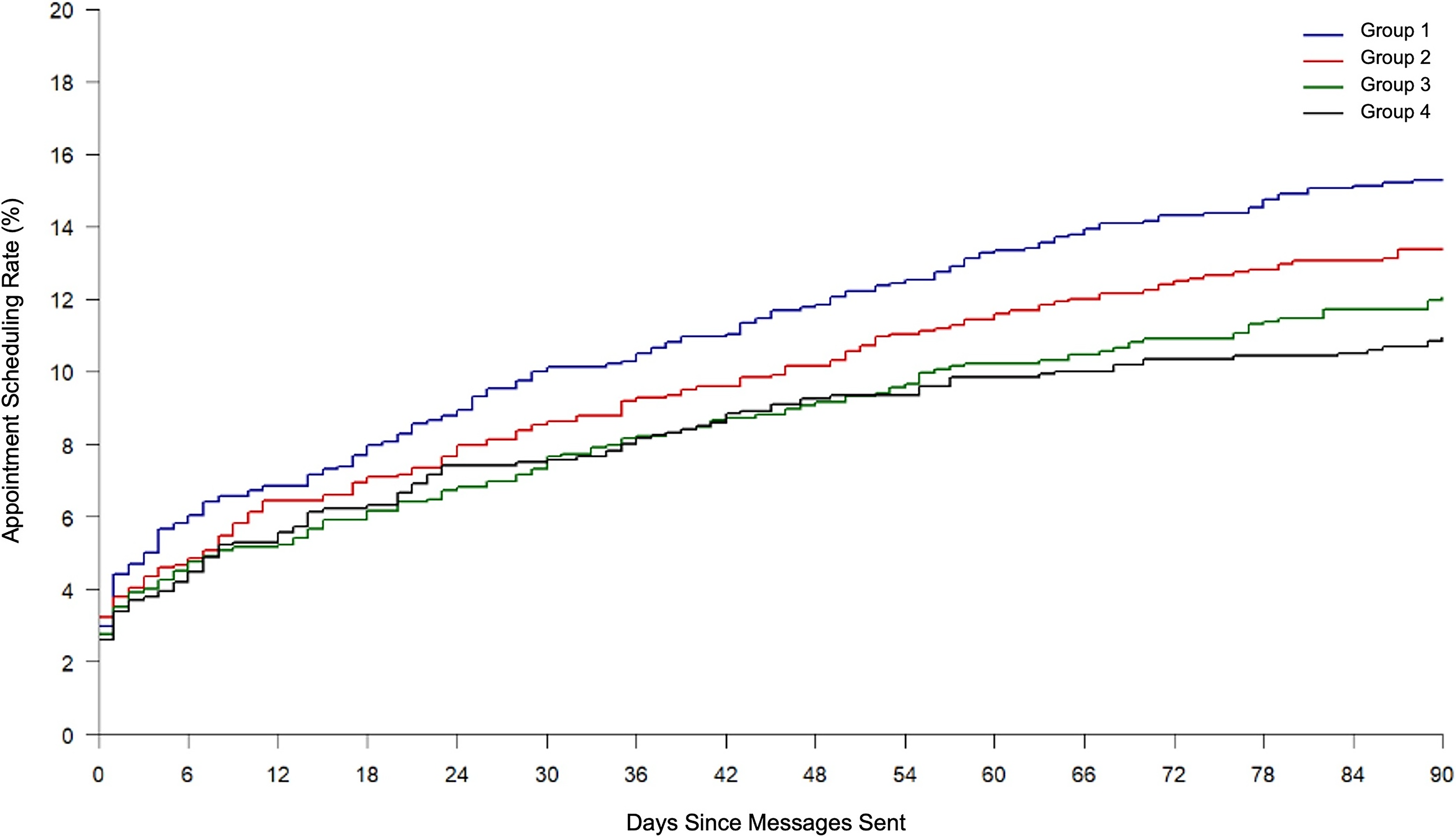
Retinal fundus photo appointment scheduling rate by bulk order group Kaplan–Meier curves for the percentage of patients who scheduled a retinal fundus appointment according to the bulk order group, with the interval in days since bulk order message was sent.
For patients who had an attributed provider in a clinic that was also a teleretinal screening site, the bulk order intervention was not more effective than patients seen at a clinic without a retinal camera; however, patients attributed to clinics with a retinal camera did have an increased odds of completing DR screening (OR: 1.43, 95% CI: 1.19–1.73, p < 0.001).
Discussion
This work highlights how implementing bulk ordering as a population health protocol could enhance use of health systems’ teleretinal screening infrastructure to improve DR screening rates. After receiving a teleretinal screening bulk order, patients had 1.79 times the odds of completing their annual diabetic eye exam.
Many barriers to completion of DR screening are identified in the literature. The majority of patients who are diagnosed with diabetes are cared for within primary care. 19 Competing demands on primary care physicians make communicating the purpose and importance of DR screening a challenge. 20 Teleretinal screening bulk orders allow patients the opportunity to complete their annual diabetic eye exam without waiting to see their individual provider and then have them place an order. Of all patients, 775 (13.6%) self-scheduled an appointment for a retinal fundus photo after receiving the bulk order. Additionally, access to care is a significant barrier found by patients due to long wait times for ophthalmology appointments and poor service experiences when making appointments.21,22 Patients were able to self-schedule their retinal fundus photo appointments within their EHR patient portal. Thirteen percent of appointments (n = 101) were scheduled within 24 h of receiving the teleretinal screening bulk order, and the median number of days until the appointment was 79 days.
Lack of patient knowledge decreases rates of DR screening, as studies have shown that patients may deprioritize diabetic eye disease and the need for screening if they do not have visual symptoms.21,23–25 The electronic patient message associated with the teleretinal screening bulk order incorporated key patient education material about DR and the recommendation for regular eye exams for all patients with T2DM (Supplemental A). Opening the electronic patient message was associated with increased retinal fundus photo appointments scheduled and overall DR completion rates. This suggests the importance of patient education in addition to preventative orders.
Behavioral science literature on promoting vaccination demonstrates how patient communications can motivate individual behavior by providing a stimulus that will influence action on a subsequent process.26–28 This is an exciting area of research that can be tied with system-wide centralized bulk orders for a wide range of preventative screenings. Further studies looking at different patient messages about DR screening are needed to evaluate the effect of applying behavioral science to associated patient communications. Additionally, most patients opened the electronic messages within 24–48 h of receiving it. Behavioral science could be applied to determine if timed reminders could further increase patient engagement and completion rates. Future studies are needed to optimize the timing and format of patient communications.
Our study has many strengths. First, simple randomization successfully resulted in balanced bulk order groups, controlling for potential unmeasured confounders. No significant difference in completion rate was seen based on reported race, ethnicity, age, sex, or social vulnerability index. Second, our intervention has low operating cost with minimal personnel requirements. Finally, although teleretinal screening alone has been shown to improve access, this study confirms how population-level interventions such as bulk orders can further improve preventative DR screening using existing teleretinal screening infrastructure. 29
Generalizability of our findings may be limited as our study was conducted in a single health system in an urban setting with an existing teleretinal screening program. In our study, having an attributed provider at a clinic with a retinal fundus camera onsite significantly increased the odds of completing DR screening by 1.43, suggesting further expansion of retinal fundus cameras in clinics could increase completion rate. Further studies are needed to optimize number of teleretinal screening sites for the size and population of specific health systems. Our findings may be more applicable to patient populations with high rates of activated EHR patient portals as limiting the study to patients who had an active patient portal may have introduced a selection bias. Recorded diagnoses for T2DM and DR relied on insurance claims and clinician documentation which may represent an under-estimation of these conditions. Additionally, if patients completed their annual DR screening outside of our health system and did not notify their outpatient provider, this could result in misclassification of the outcome, biasing our result toward the null.
With increasing barriers to access to care, demands on physician time, and lack of patient awareness, population health initiatives combined with teleretinal screening programs are critical for the care of patients with diabetes. Improving DR screening rates is essential in detecting disease early and reducing the burden of vision loss due to DR. Our findings demonstrate how system level outreach through teleretinal screening bulk orders can successfully increase DR screening rates. Further studies to determine if automated reminders, alternative patient communication methods such as text messages, and utilization of behavioral science in the language of patient messages can further enhance the efficacy of bulk orders. Our research emphasizes the important potential of telehealth and population health initiatives in preventative diabetes care.
Ethics Statement
The University of California, Los Angeles Institutional Review Board determined that this QI intervention did not meet the definition of human subjects research as defined by federal regulations for human subject protections 45 CFR 46.102(I); therefore, certification of exemption nor IRB approval was required.
Data Availability Statement
Deidentified datasets that support the findings of this study are stored in a secure server and are available upon reasonable request from the corresponding author (S.W.T.).
Authors’ Contributions
Conceptualization and study design: S.W.T., M.F., M.H., S.V., and S.L. Data collection and curation: S.W.T. and S.L. Formal analysis: S.V., S.W.T., and S.L. Visualization: S.W.T. and S.V. Writing—original draft: S.W.T., S.L., and S.V. Writing—review and editing: All authors.
Footnotes
Acknowledgments
The authors would like to acknowledge the UCLA Diabetes Steering Committee for their support in this project.
Author Disclosure Statement
The authors have no conflicting interests to report.
Funding Information
This research did not receive any specific grants from funding agencies in the public, commercial, or not-for-profit sectors.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.