
Abstract
Adolescent idiopathic scoliosis (AIS) is often associated with unbalanced posture and proprioceptive deficits and is particularly prone to progression during puberty. However, limited research has addressed early intervention for mild curves (10-20 degrees). This study aims to examine the effects of a soft bracing intervention using the Posture Correction Girdle (PCG) on 3D postural balance and proprioception in adolescents with early-stage scoliosis. Cobb angles were measured with the X-ray Imaging before and after a 2-h wear trial with the girdle to assess immediate curve reduction. Postural angles were visualized using 3D body scanning. Proprioception was assessed using a motion capture system, focusing on trunk, neck, elbow, and knee movements under the eye-open and eye-closed condition. Data were analyzed using descriptive statistics, t-tests, and Pearson’s correlation and partial Mantel tests to examine postural balance and proprioceptive outcomes. Results indicated significant improvements in postural balance in the frontal and sagittal planes, and proprioception in the dominant-side elbow. However, other proprioceptive measures showed limited changes, with responses differing by spinal curvature. Strong correlations emerged between proprioceptive function and postural angles in the thoracic and lumbar regions. These findings suggest that soft bracing can enhance postural control for mild AIS, though individual variability in responses highlights the need for personalized bracing strategies. This study supports soft bracing as a promising therapeutic option, underscoring the importance of individualized assessment to optimize brace design and effectiveness in early-onset scoliosis management.
Introduction
Scoliosis is a multifaceted spinal disorder characterized by a Cobb angle greater than 10 degrees, encompassing both lateral curvature and potential axial rotation of the vertebrae. 1 When this curvature manifests without a known cause, it is classified as idiopathic scoliosis. 2 The risk of curve progression is most pronounced during puberty, with studies indicating varying probabilities of worsening angles as the curvature increases. 3 The management strategies of idiopathic scoliosis range from periodic monitoring for milder curves to the application of orthotic devices and specialized exercises for more pronounced deformities. 4 Conservative bracing treatment is recommended for children with AIS who have curves between 20 and 40° before reaching skeletal maturity. 5 The mechanical principle of braces is to provide external corrective forces to address the complex 3D spinal deformity. Braces can be categorized into different concepts, including rigid braces, soft braces, and nighttime braces, which have been described and compared for their effectiveness. The success rates of various bracing options are as follows: rigid full-time braces (16–23 hours/day) achieved a success rate of 73.2%, nighttime braces 78.7%, and soft braces 62.4%. In comparison, the success rate of observation alone was only 50%. 6 However, achieving high compliance with rigid braces can be particularly challenging for teenagers due to discomfort. As a result, soft braces have become a more favorable and practical option in recent years. For curvatures within the mild curves range (10 to 20°), there is a notable lack of research to guide early intervention, and the potential role of soft bracing in this context remains largely unexplored.
Contributing factors to the development of scoliosis are diverse, including rapid growth, hormonal fluctuations, and muscular imbalances during puberty.7,8 A genetic component is also suggested by the familial occurrences seen in some patients with AIS. 9 Emerging research implicates functional abnormalities in the central nervous system, such as deficits in proprioception, which is vital for maintaining spinal alignment and balance. 10 These proprioceptive impairments may disrupt an individual’s ability to coordinate body posture and movement.11–13 Recent meta-analyses corroborate the presence of proprioceptive deficiencies in AIS patients, as demonstrated by their increased repositioning errors. 14
Individuals with AIS often exhibit body asymmetry, such as a rib hump, uneven shoulders, tilted pelvis, and different leg lengths due to the unbalanced loading on both sides of the trunk caused by the spinal curvature.15,16 This curvature also results in the misalignment of the head, shoulders, and pelvis, shifting the center of gravity. 17 Inadequate postural control can exacerbate discomfort and further distort the trunk in those with AIS. Studies have shown that asymmetrical posture and unstable postural contribute not only to spinal curvature but also to associated pain.18,19 An imbalanced load on the spine, stemming from poor posture, may promote uneven spinal growth and vertebral anomalies. Those with improper postural habits are at an increased risk of falls, particularly when handling heavy objects without sufficient trunk stability. 20 Such incidents can aggravate scoliosis progression, placing uneven stress on specific spinal regions and leading to unpredictable load distribution. As scoliosis advances, the equilibrium between skeletal structure and muscular support is progressively undermined, potentially creating a detrimental cycle of poor posture and increasing curvature, especially in individuals who have not yet reached skeletal maturity. 21
Adding to the complexity of AIS management is the challenge of accurately assessing spinal proprioception. While it is recognized that some AIS patients exhibit proprioceptive deficits in peripheral joints, the proprioceptive function of the deformed spine itself has been less studied. Traditional assessments have focused on single-plane evaluations, which may not fully capture the three-dimensional nature of spinal proprioception. A recent study sought to address this gap by developing a novel three-dimensional spinal proprioception assessment using motion analysis. This assessment involved three trunk repositioning tests: flexion-extension, lateral-flexion, and axial-rotation, with three-dimensional kinematics serving as the outcome measures. The reliability of these tests was analyzed, revealing that the trunk flexion-extension repositioning test exhibited the highest reliability, making it a potentially valuable clinical tool for evaluating spinal proprioceptive acuity in AIS patients. 22 These findings underscore the importance of reliable and multidimensional proprioceptive assessments in the management of AIS and support the need for further research into the role of proprioception in scoliosis progression and treatment.
In light of the association between AIS, postural challenges, and deficits in proprioception, this study is designed to examine the impact and interplay between three-dimensional postural balance and proprioception in adolescents with early-stage scoliosis who undergo a brief soft bracing intervention. Utilizing the Posture Correction Girdle (PCG), an orthotic device developed by Liu et al., 23 as the means for soft bracing treatment, it is hypothesized that the PCG soft bracing intervention can enhance proprioceptive function by providing external corrective forces that stimulate proprioceptive feedback mechanisms. This improvement in proprioception is expected to facilitate better coordination of posture and movement, contributing to improved three-dimensional body control in adolescents with early-stage scoliosis. This investigation will contribute to the body of knowledge on conservative management approaches and their potential to address the underlying issues of posture and proprioception in the context of AIS. Furthermore, by exploring the textile engineering aspects of the PCG, this study focuses on innovative textile applications.
The design and material properties of the girdle are crucial for ensuring comfort, flexibility, and effectiveness, highlighting the importance of advanced textile solutions in medical applications.
Material and methods
PCG design and materials used
The PCG is a tight-fitting, vest-like undergarment that covers the torso from the shoulders to the pelvis.23–25 It is constructed primarily from warp-knitted fabrics such as tricot, satinette, and powernet due to their strength and excellent recovery properties. The main components include the base garment, semi-rigid resin bones, a waistband, shoulder straps, and internal pocket lining (see Figure 1). This design helps maintain proper body balance, prevent poor posture, and relieve postural strain. Additionally, ethylene-vinyl acetate (EVA) foam pads can be inserted into the pocket linings to create corrective pressure points tailored to individual treatment, aiming to achieve neuromuscular registration of the new corrected position. Typically, 2 to 3 EVA foam pads are inserted to target the apex of the spinal curve. The tension of the straps is adjusted by a professional to exert additional corrective forces as required for each case. Since the PCG is a type of soft brace, it allows for greater freedom of movement in daily life. The unbalanced tightness of muscles and ligaments can be stretched and relaxed to form a new balance between antagonistic muscle groups, helping to control body position effectively. Features of PCG.
Subject recruitment and the soft-bracing treatment
A total of 10 participants average aged at 12 were included in the study. The average height was 157.6 ± 5.79 cm, with an average weight of 44.99 ± 5.86 kg, resulting in a mean BMI of 18.09 ± 2.35 kg/m2. The Cobb angle at the main curvature averaged 15.71 ± 2.6°. In terms of curve type, 7 subjects presented with an S curve, while 3 subjects had a C curve. The curve apex ranged from T7 to L5, and the Risser sign, indicating skeletal maturity, ranged from grade 0 to 3. They were required to be diagnosed with early scoliosis characterized by a Cobb’s angle between 10 and 20 degrees measured on a recent (<3 months) full spine radiographic image; premenstrual or less than 1 year post-menarchal, able to communicate effectively in either English or Chinese (Cantonese dialect), and physically and mentally capable of completing the entire treatment; have a Risser grade of no more than 3 on the iliac crests and no contraindications for X-ray exposure, recent trauma, mental disorders, or skin allergies; and have not received previous surgical or orthotic treatment for AIS. Participants were recruited after confirming eligibility based on the inclusion criteria and the collection of informed consent. This study was approved by the Human Subjects Ethics Sub-committee of The Hong Kong Polytechnic University in accordance with the Declaration of Helsinki (Approval No.: HSEARS20210824003). Participants took a fitting process of PCG. The vest-like undergarment features a 3-zipper design at the center front, allowing the girdle to cover a larger range of waist circumferences with the same size. EVA padding is strategically inserted into pockets inside the vest-based undergarment to provide corrective force to the spinal curve. The waistband is stretchable, from one side to the other, and the straps wrap around the shoulders, crossing at the back and attaching to the sides of the body. The free-end design of the shoulder straps and waistband creates an “imbalanced” corrective force, with markings offering better control and clearer references for tension adjustment. Moreover, the selected powernet enhances dimensional stability, durability, pilling resistance, and overall comfort of the girdle. The fitting is fine-tuned using postural alignment with plumb line to adjust the corrective components (EVA padding, waistband, and shoulder straps) until optimal alignment is reached. The fitting process is complete once the body trunk achieves the desired alignment. X-ray measurements (in-brace) are then taken after wearing the brace for 2 hours. If the Cobb angle improves by more than 5 degrees, we recommend including the subject in our wear trials and subsequent experiments.
Data collection

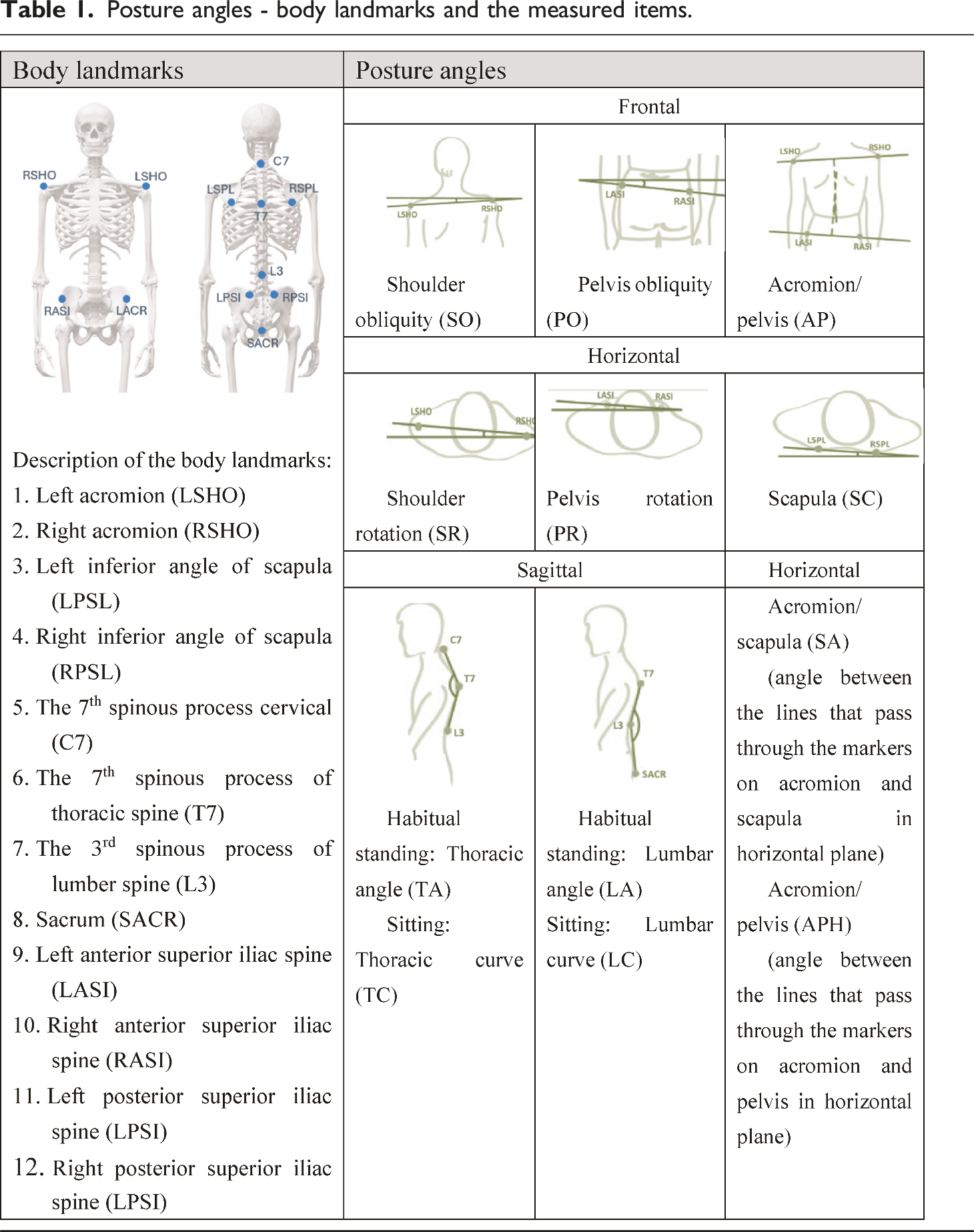
Posture angles - body landmarks and the measured items.

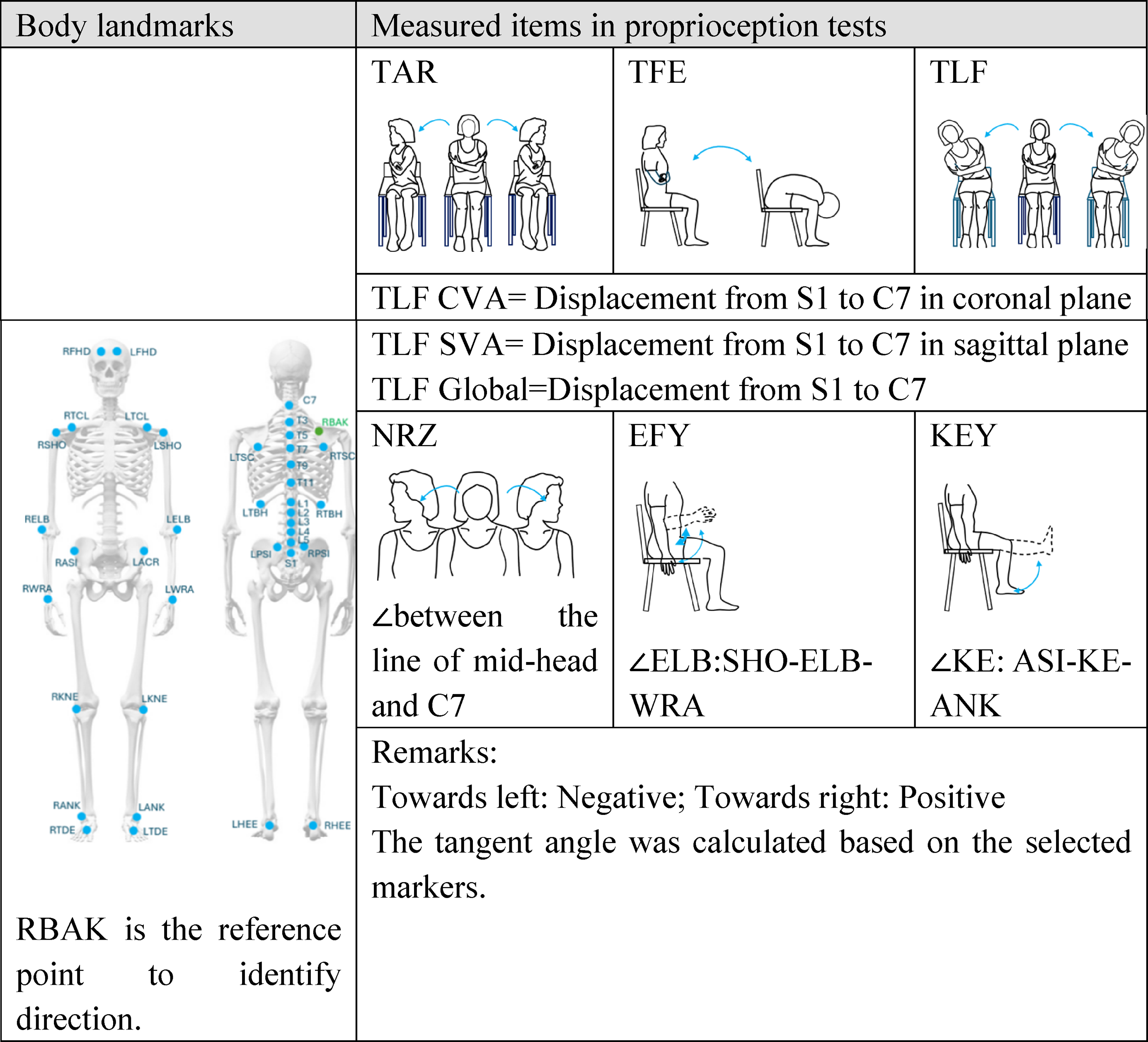
Proprioception experiment - body landmarks and the measured items.

Statistical analysis
Demographic data were summarized using descriptive statistics. The normality of postural and proprioception data distributions across different groups was assessed using the Kolmogorov-Smirnov or Shapiro-Wilk test. Normally distributed continuous variables were analyzed with an independent samples t-test, while non-normally distributed variables were evaluated using the Mann-Whitney U test, performed in SPSS statistical software (IBM SPSS Statistics Version 26.0, Chicago, IL). The null hypothesis of equal means was rejected at a 5% significance level (Type I error probability). Pairwise comparisons were conducted to assess the within-group correlations of proprioception and indices of inter-side asymmetry using Pearson’s correlation analysis. Additionally, to evaluate the association between postural balance and proprioceptive outcomes while accounting for the potential confounding effect of spinal curvature, partial Mantel tests were employed to explore correlations among postural balance in different planes and proprioceptive outcomes, using R software (version 4.3.3).
Results
Postural angle assessment
After the 2-h wear trial, the Cobb angle at the main curvature was generally reduced (i.e. averaged 10.98 ± 4.13°). The paired t-test results of the postural angle assessment are summarized in Figure 2, where smaller values denote a more balanced posture. The results demonstrated significant differences in several postural parameters between pre-wear and post-wear trials, indicating a notable effect of the girdle intervention on postural alignment. Specifically, significant changes were observed in the frontal, horizontal, and sagittal planes. In the frontal plane, Shoulder Obliquity (SO) decreased from 2.29 ± 0.72° to 1.19 ± 0.68°, with a mean change of 1.04° (p = .0008, Cohen’s d = 1.567), indicating improved shoulder alignment. Pelvis Obliquity (PO) also decreased significantly from 1.44 ± 0.58° to 0.73 ± 0.38°, with a mean change of 0.70° (p = .0044, Cohen’s d = 1.193), suggesting better pelvic alignment. Similarly, Acromion/Pelvis (AP) orientation decreased from 2.33 ± 1.63° to 0.66 ± 0.64°, with a mean change of 1.67° (p = .0071, Cohen’s d = 1.097), indicating enhanced alignment between the acromion and pelvis. In the horizontal plane, Shoulder Rotation (SR) decreased from 3.26 ± 1.94° to 1.82 ± 0.83°, with a mean change of 1.43° (p = .0325, Cohen’s d = 0.799), demonstrating significant improvement in shoulder rotation. Scapula (SC) orientation also showed a significant decrease from 2.29 ± 1.15° to 1.47 ± 1.04°, with a mean change of 0.81° (p = .0380, Cohen’s d = 0.768), suggesting enhanced scapular alignment. In the sagittal plane, Thoracic Curve (TC) increased from 152.43 ± 3.62° to 160.3 ± 4.37°, with a mean change of −7.82° (p = .0007, Cohen’s d = 1.594), indicating a significant increase in thoracic curvature post-intervention. Lumbar Curve (LC) also increased significantly from 150.50 ± 6.32° to 157.8 ± 4.70°, with a mean change of −7.34° (p = .0007, Cohen’s d = 1.581), suggesting an increase in lumbar curvature. Additionally, Thoracic Angle (TA) in the sitting position increased from 157.16 ± 7.59° to 160.8 ± 4.68°, with a mean change of −3.68° (p = .0144, Cohen’s d = 0.956), indicating enhanced thoracic extension. In contrast, Pelvis Rotation (PR) (p = .8869) and Scapula/Acromion (SA) orientation (p = .1895) showed no statistically significant differences, suggesting that the intervention had limited or no effect on these aspects. The Acromion/Pelvis in horizontal plane (APH) (p = .1097) and Lumbar Angle (LA) (p = .0769) also did not demonstrate statistically significant changes. Postural angle changes pre and post wear trial in frontal, horizontal and sagittal plane. ***: p < .001 (very highly significant) **: p < .01 (highly significant) *: p < .05 (significant).
Proprioceptive measurements: outcome
The results of wearing a girdle on proprioceptive measurements related to neck rotation, knee extension, elbow flexion, and other body parameters were shown in Figure 3. Larger values of the parameters indicate a greater repositioning error between eyes-open and eyes-closed conditions. For the EFY on dominant side, the mean value decreased from 4.448 ± 1.757° to 2.360 ± 1.620°, with a mean change of 2.088° (p = .021), indicating a significant reduction in the degree of elbow flexion required to perceive proprioceptive cues on the dominant side. while the paired t-test for EFY non-dominant side did not reach statistical significance (p = .089), suggesting that the girdle effect may not be as pronounced on the non-dominant side. The mean value of trunk repositioning error after flexion-extension in coronal plane (TFEC) decreased from 4.357 ± 1.335 mm to 2.894 ± 2.642 mm, with a mean change of 1.464 mm (p = .045), suggesting improved alignment and potentially enhanced proprioceptive control in the thoracic region. Other parameters did not show statistically significant changes. For example, neck rotation of the spinal convex direction (NRZV) increased slightly from 2.970 ± 1.455° to 3.396 ± 2.010°, with a mean change of 0.426° (p = 1), indicating no significant effect. Similarly, knee flexion-extension on dominant side (KEYD) showed an increase in mean value from 2.318 ± 1.321° to 2.908 ± 1.703°, with a mean change of −0.589° (p = .473), indicating no significant improvement in proprioceptive control. Other spinal parameters, such as trunk flexion-extension in global coordination (TFEG) and trunk axial rotation in coronal plane (TARC), also showed changes that were not statistically significant, indicating that the girdle had a limited effect on these proprioceptive aspects. Cervical, joints, and spinal proprioceptive measurements. Remark: ***: p < .001 (very highly significant) **: p < .01 (highly significant) *: p < .05 (significant).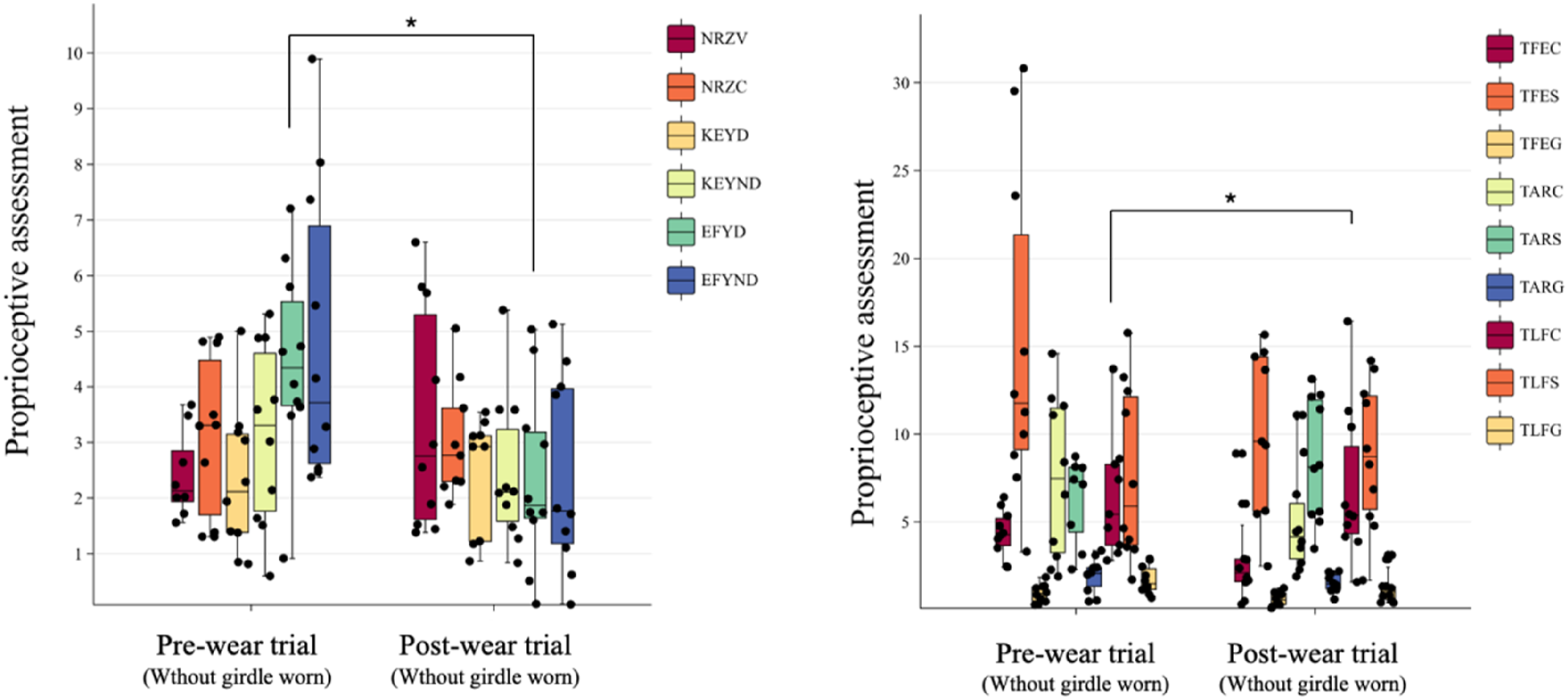
The inter-side asymmetric index of proprioceptive outcomes before and after girdle worn.

The partial Mantel test analysis identified several significant relationships between proprioceptive outcomes at the neck, knee, elbow, and trunk and posture parameters, as illustrated in Figure 4. A color gradient represents Pearson’s correlation coefficients, with edge width corresponding to the partial Mantel’s r statistic for the respective distance correlations, and edge color indicating statistical significance. Specifically, significant correlations were found between NRZ and PR (r = 0.463, p = .048) and SA (r = 0.533, p = .008), indicating that pelvic and scapular alignment are closely associated with NRZ. EFY showed no significant correlations with posture parameters, with the highest association being with SA (r = 0.295, p = .102). KEY also did not show significant correlations, with the strongest association observed with TC (r = 0.312, p = .097). TAR was significantly correlated with SC (r = 0.563, p = .002) and SO (r = 0.342, p = .025), indicating that scapular positioning and shoulder alignment influence TAR. TFE showed significant positive correlations with SA (r = 0.350, p = .049) and APH (r = 0.487, p = .019), suggesting that scapular and acromial alignment influence thoracic flexion-extension. TLF was significantly correlated with LA (r = 0.492, p = .007), while the strongest non-significant association was observed with PR (r = 0.666, p = .051), indicating that lumbar alignment is linked to TLF. Pairwise comparisons of posture parameters which use color gradient to represent Pearson’s correlation coefficients. Proprioceptive outcomes at EFY, KEY, NRZ, TAR, TFE, and TLF in relation to each posture parameter using partial Mantel tests. Width of edges = Mantel’s r statistic for respective distance correlations. Color of edges = statistical significance.
Correlations of postural balance with proprioception and inter-side asymmetry index
The correlation between the index of the inter-side asymmetry and imbalance in body angle is depicted in a correlation heatmap shown in Figure 5. It was observed that NR has a negative correlation with TC (r = −0.74, p < .05), KEY has a negative correlation with TA (r = −0.70, p < .05) and LA (r = −0.79, p < .01), while EFY has a positive correlation with LA (r = 0.75, p < .05). These results suggest that as the TC increases, which means a straighter back, the NRZ and KEY tend to increase in asymmetric movement. Similarly, increases in TA and LA, which reflect more balanced body angles, are associated with increased symmetric movement in terms of the NRZ and KEY. Conversely, EFY shows the opposite tendency, with increased inter-side asymmetry associated with higher LA values. Correlation between the index of the inter-side asymmetry for proprioception with NRZ, KEY, and EFY, and spinal proprioception. Color gradient represents Pearson’s correlation coefficients.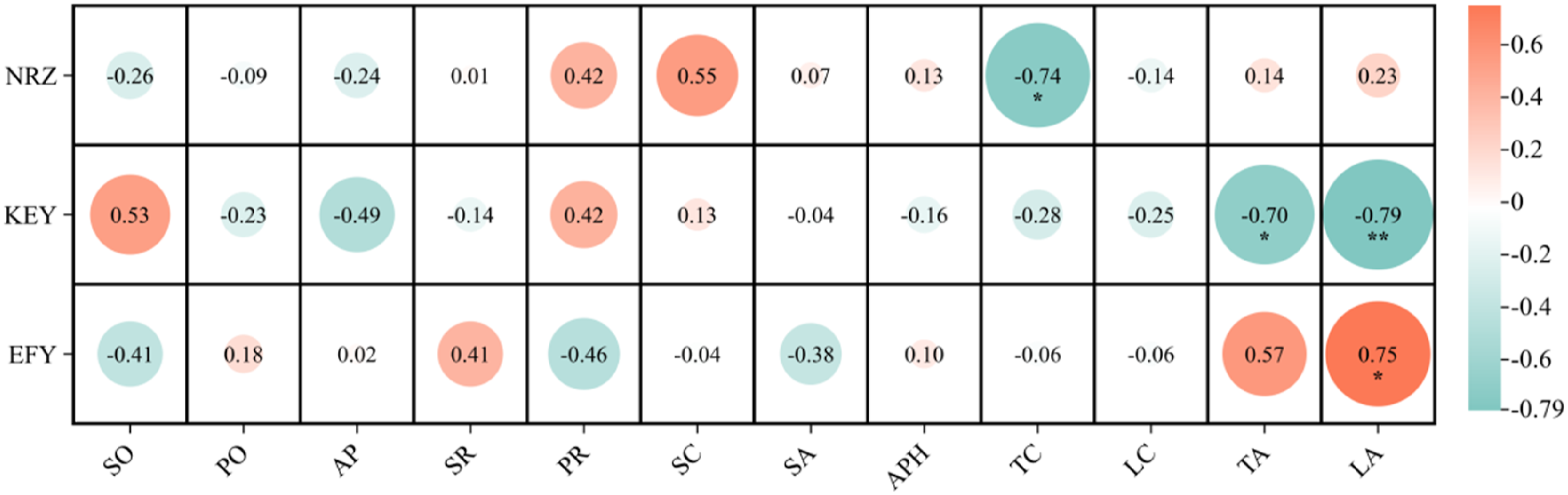
Discussion
It has been well-documented that scoliosis often leads to compensatory postures that adapt to spinal deformities.15,26 These manifestations typically include asymmetric body posture, shoulder and pelvic unevenness, and hunching. 27 These symptoms often result from altered postural alignment and a shifted perception of the body’s midline due to postural adaptation to trunk imbalance. However, little research has focused on the postural angle correction by bracing and its relationship with proprioceptive outcomes. Hence, the primary aim of this study was to investigate the immediate effectiveness of a PCG on 3D posture balance and proprioception in adolescents with early scoliosis. Additionally, we sought to explore the relationship between posture parameters and proprioceptive outcomes following short-term soft bracing treatment.
To address the aforementioned inquiries, this study utilized 3D body-scanned geometric models and 3D motion capture trajectories, which were established as highly accurate methods in 3D postural and motion analysis. 28 The validated repositioning error test protocol for measuring proprioceptive outcomes in patients with AIS was employed in this study. 22 The results revealed a general reduction in postural imbalance among participants following a short-term soft bracing treatment. Furthermore, significant improvements were observed between pre-treatment and post-treatment with the girdle. Consistent with existing literature, our findings suggest that the PCG can ameliorate postural imbalance in adolescents with AIS during habitual standing and sitting. 29
Specifically, in the frontal plane, significant improvements in SO, PO, and AP balance were observed with the use of the PCG. This improvement may be attributed to the elastic straps and multi-point pressure correction system provided by the inserted padding, which corrected lateral spine curvatures and altered individual postural patterns. Additionally, significant differences were found in shoulder rotation and scapular rotation under different brace conditions, indicating correction of upper back rotation but less noticeable derotation in the lower back. In the sagittal plane, there was a significant decrease in the back angles of TC and TA during habitual standing after wearing the PCG, with TA showing consistent significant effects, expect TA. These results suggest that the PCG aids in improving imbalance issues and straightening back angles. These results tie well with previous studies wherein bracing that provided with a laterodorsal force can push the spine forward and straighten it in the coronal and sagittal planes by using MRI scan. 30
For the proprioceptive outcomes, significant differences were found at the elbow and trunk between pre- and post-bracing treatment. Inconclusive evidence suggests that proprioception may play a role in the pathogenesis of AIS. 31 Compared with previous results, this study found that the cervical spine repositioning error on the concave side increased slightly, from 2.41° to 3.39°, while the convex side showed a small decrease, from 3.12° to 3.02°. These findings are in line with previous studies, which indicate that AIS participants generally exhibit larger repositioning errors compared to healthy controls for the neck, elbow, and knee joint angles. Specifically, it reports a pooled mean difference of 1.27°, suggesting that AIS participants have a significantly poorer ability to reposition their neck joint compared to healthy individuals. 14 For the knee joint repositioning error, results show that the dominant side showed a slight increase in error, from 2.31° to 2.47°, while the non-dominant side decreased from 3.13° to 2.44°. The previous studies suggest that AIS participants also exhibit a larger motion detection threshold in the knee joint, with a mean difference of 1.60°, indicating that AIS patients generally have a poorer ability to detect joint motion. Both our study and previous studies suggest that AIS patients experience poorer proprioception in the knee joint. However, our results indicate some improvement in proprioception (with decreased repositioning error on the non-dominant side).11–13 For the elbow joint repositioning error, this study found that the repositioning error decreased for both the dominant and non-dominant sides, with values changing from 4.45° to 2.36° (dominant) and from 4.84° to 2.41° (non-dominant). Previous studies similarly indicated that AIS participants had larger repositioning errors in the elbow joint compared to healthy controls, with data demonstrating significantly larger joint repositioning errors for AIS participants. This study shows improvement in both limbs for the elbow joint, whereas previous studies show that AIS patients generally perform worse than controls, without significant improvement reported. This discrepancy might indicate that our study highlights the PCG therapeutic effects that help improve proprioception.13,14 This suggests that the application of external corrective forces through the PCG is effective in restoring postural balance in mild scoliosis, possibly by providing proprioceptive input due to changes in brain processing, addressing unnatural loading, asymmetrical movements, and facilitating sensory feedback transmission caused by the activation of mechanoreceptors and neuromotor reorganization, as indicated in previous literature. 32 For EFY on dominant side, there was no statistically significant difference observed; however, the mean error on the non-dominant side was slightly larger compared to the dominant side. This finding aligns with previous studies measuring proprioception in AIS patients without a brace. The observed results may be influenced by the direction of spinal curvature, as the majority of participants in this study had a right thoracic convex curve. Previous research suggested that individuals with a convex curvature tended to overestimate elbow flexion, which could explain the reduced responsiveness to bracing in this cohort. 33
For the cervical spine and knee, no significant differences were observed, which may be attributed to three factors. Firstly, the mild curvature may not generate enough mechanical stress or changes in the spinal structure and surrounding muscles to significantly impact proprioceptive feedback. 33 This is consistent with research indicating that only Cobb angles greater than 40 degrees lead to significantly prolonged somatosensory evoked potential (SEP) latency, affecting posture. 34 Secondly, the duration of the bracing treatment may have been insufficient to produce substantial changes in muscle activation and spinal biomechanics, limiting its impact on proprioception. Thirdly, children with AIS may have adapted to altered muscle recruitment patterns to maintain postural stability, resulting in minimal differences before and after bracing treatment.
While the causes of AIS are multifactorial, hypotheses from previous studies suggest that alterations in the peripheral or central nervous system induce asymmetrical drive to the torso muscles.35,36 Shao et al. demonstrated that compared to non-AIS children, AIS children exhibited selective type I fiber atrophy within the paraspinal muscles on the concavity of the curve, which could contribute to spinal deformity. 37 This paraspinal muscle imbalance may act on vertebrae, influencing their growth rates differently across various parts of the vertebrae, potentially resulting in wedge-shaped deformities and initiating scoliosis. 38
Significant correlations were found among NRZ, TAR, TFE, TLF, and body postures, thus suggesting that increased spinal alignment may coincide with enhancements in proprioceptive function. As braces correct scoliotic curves and improve postural balance, they may also improve proprioceptive control to help AIS have a better postural control and reduce asymmetry, which potentially contributes to controlling the progression of spinal curvature in adolescents with mild AIS.
Nevertheless, there are inherent limitations in this study. First, the sample size is limited, which potentially influences the ability to detect significant associations. As a result, weak relationships are likely to go undetected. Second, the study focuses on the effectiveness of bracing on AIS children with mild curvature in terms of correcting postural angles and proprioception, rather than exploring the overall efficacy of bracing on AIS. Consequently, there is no control group in this study. In the future, we intend to include a control group with a prior standard bracing intervention to strengthen internal validity. Third, the study evaluates the immediate effects of a short-term, two-hour PCG trial, which is insufficient to reflect the long-term requirements and outcomes associated with AIS treatment. This short duration is designed as a preliminary, exploratory investigation to evaluate feasibility, comfort, and initial biomechanical responses, but it does not encompass the full therapeutic potential of the intervention. Future studies with prolonged wear durations and extended follow-up assessments over a nine-month period are necessary to evaluate the long-term effects of PCG, such as curve stabilization, enhanced proprioception, and sustained postural improvements.
Conclusion
This study provides insights into the immediate effects of using a soft brace on various aspects of postural balance and proprioception in adolescents in the early stages of scoliosis. Our findings reveal that children with AIS exhibit more pronounced body postural imbalances compared to before the treatment with the soft brace PCG, particularly evident in parameters within the frontal plane during habitual standing and the sagittal plane during sitting. Notably, the PCG shows effectiveness in correcting postural imbalance, highlighting its potential as a therapeutic intervention in managing AIS-related postural abnormalities. Wearing the girdle significantly improved proprioceptive control in elbow on the dominant side and trunk alignment, suggesting the effectiveness of external corrective forces in mild scoliosis. However, other proprioceptive parameters showed no significant changes, indicating the girdle’s limited influence in certain areas. The variability in responsiveness may be related to spinal curvature direction, highlighting the need for individualized bracing approaches. Notable correlations were found between proprioceptive function and body postural angles, including the thoracic and lumbar curves and angles during habitual standing and sitting. This suggests a significant relationship between postural correction and repositioning accuracy, emphasizing the importance of the comprehensive assessment of bracing on postural control and proprioception and the implications for the management of early-onset AIS.
Footnotes
Authors’ contributions
Pak-Yiu Liu and Jun Zhang contributed equally to this paper. Pak-Yiu Liu was responsible for preparing the postural correction girdle, collecting data, and drafting the initial manuscript. Jun Zhang was responsible for the data collection and analysis, and also contributed to the initial draft of the manuscript. Frances Ka Wing Wan and Brian Y. Chen designed the experiment protocols and wrote the MATLAB code for data processing. Hiu-Tung Yu labeled motion data and conducted preliminary data cleaning. Kenney Ki Lee Lau contributed to designing the experimental protocols. Kenneth Man Chee Cheung provided professional guidance on medical questions. Joanne Yip commented on and revised the manuscript, and also acquired funding for the project. All of the authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is funded by the Lee Hysan Foundation (Ref. No. R-ZH3Y).