
Abstract
Research to assess and inform health policy is an essential component of the policymaking process to advance equity in public health practice. This study investigated health disparities during the COVID-19 pandemic (2020–2022) in older adult institutional settings in Philadelphia, PA, to inform policy initiatives, interventions, and infrastructure development. We first explored the changing patterns of nursing staffing levels (total direct care staff and registered nurses [RNs]) measured by hours per resident per day (HPRD) before and after COVID-19. Our findings revealed that HPRD levels consistently fell below the Centers for Medicare and Medicaid Services recommended standards from 2018 to 2022, with notable declines observed starting from 2021. Results from multilevel modeling showed significant declines in HPRD for total direct care nursing staff in nursing homes located in zip codes with a high proportion of Black residents (≥40%). In contrast, HPRD for RNs significantly declined in nursing homes located in zip codes with a lower proportion of Black residents (<40%). Moreover, higher reported direct care HPRD and RN HPRD were associated with any reported COVID-19 cases only within zip codes with a low proportion of Black residents. These findings indicate the need for additional policies to address these observed patterns in staffing levels. Our study provides a foundation for future policy reviews utilizing a conceptual framework that is health equity-centric for local and state health departments program and units intended for institutional care settings for older adults.
Introduction
Staffing levels in nursing homes (NHs), as measured by various indicators (e.g., count/ratio of staffing, staff shortage, staff time), have been a prevailing topic of interest as the number of NH residents with multiple comorbidities (e.g., cardiovascular disease, dementia) and functional limitations is increasing (Bakerjian et al., 2021). Staffing levels have been shown to be associated with a safe and higher quality of care for NH residents (Bakerjian et al., 2021; Shin et al., 2021; Spilsbury et al., 2011). Specifically, Spilsbury et al. (2011) concluded that total nurse staffing levels (i.e., registered nurse [RN] and nursing assistant [NA]) are associated with all NH quality care indicators.
During the COVID-19 pandemic, staffing shortages in NHs presented a major public health challenge (Bakerjian et al., 2021). Previous studies in the United States have addressed the relationship between nursing staff shortage and COVID-19 infection. States from the East and Midwest regions were more likely to report staffing shortages among licensed nurses (RN and licensed practical nurse [LPN]) as well as certified nursing assistant (CNA) in May 2020, during the COVID-19 pandemic (Xu et al., 2020). Moreover, NHs with at least one COVID-19 resident case were more likely to report shortages in nursing staff, nurse aides, clinical staff and other staff compared to NHs without COVID-19 resident case (Xu et al., 2020). With regard to health disparities as measured by staff ratio, studies have shown that NHs without African American residents compared to those with more than 50% of African American residents had a lower ratio of RNs (Travers et al., 2023).
Staffing levels in NHs are usually calculated using hours per resident day (HPRD). This index measures the total number of hours of care provided to a resident each day within an NH (Harrington et al., 2020). A study from the Centers for Medicare and Medicaid Services (CMS) in 2001 found the minimum staffing levels to provide safe and quality care in NHs should be 0.75 HPRD for RNs, 0.55 HPRD for licensed vocational nurses (LVNs)/LPNs, and 2.8 HPRD for CNAs, resulting in a total of 4.1 HPRD for total direct care staffs (Harrington et al., 2020). Multiple recent studies have found that a lower nursing staff HPRD is correlated with a higher likelihood of COVID-19 infections. In California, NHs that had RN nursing time below the CMS recommended minimum standard of 0.75 HPRD were more likely to have COVID-19 resident infections than nursing homes with higher RN nursing time (Harrington et al., 2020). NHs in Florida with at least one COVID-19 case reported lower direct care staff HPRD than those without any COVID-19 positive cases (Wang et al., 2021). In Connecticut, a 20-min increase in RN HPRD was significantly correlated with a 22% reduction in COVID-19 resident cases (Li et al., 2020). Mattingly et al. (2021) found that NHs in Maryland with fewer CNA HPRD or more licensed beds had a higher risk of large COVID-19 outbreaks (resident COVID-19 cases exceeding 10% of licensed beds) from January to July 2020. They also observed health disparities, noting that NHs with a higher percentage of Black residents were more likely to have large COVID-19 outbreaks (Mattingly et al., 2021).
While prior studies have found the relationship between reduced NH HPRD and the increased risk of COVID-19 infections within some states, there has been limited research that has explored whether this relationship may vary across geographic areas within a particular location, such as large metropolitan areas. For example, Philadelphia, the largest city in Pennsylvania, had disparate COVID-19 infection rates across its zip codes in 2020 (Goldstein et al., 2022) and the highest poverty rate in the United States in 2021 (Pew, 2023). Higher COVID-19 infection rates have been observed in financially disadvantaged zip codes or zip codes of metropolitan areas with predominantly Black/African American or Hispanic residents compared to financially advantaged zip codes or zip codes with predominantly White or Asian residents (Bilal et al., 2022; Goldstein et al., 2022; Ramprasad et al., 2022). These racial health disparities in HPRD across NHs might be reflective of historical and current systemic inequities observed within the zip codes or neighborhoods where the NHs are located. Evidence of this observation would further support the intersection of various systems of influence (e.g., neighborhood, sociohistorical events, and NH) on an older adult's health, particularly within a nursing home, as suggested by the NIH/NIA Health Disparities Research Framework (Hill et al., 2015). Indeed, prior research has supported that the sociodemographic characteristics of the zip code or neighborhood where an NH is located are associated with NH outcomes (i.e., COVID-19 infection rates and quality of care; Khairat et al., 2021).
The aims of this article are to analyze the changing patterns of nursing HPRD in Philadelphia before and after the COVID-19 period in geographic zip code areas with predominantly Black populations (≥40%) and to examine the impact of COVID-19 cases and sociodemographic characteristics on NH HPRD.
Method
Data Sources
A dataset incorporating public data was developed from three different sources: (a) the Centers for Medicare and Medicaid Services (CMS); (b) the Long-Term Care Community Coalition (LTCCC); and (c) the American Community Survey (ACS). Using CMS data, 48 federally certified NHs across 25 Philadelphia zip codes were identified. The number of NHs within each zip code varied from 1 to 5. The federal nursing home provider number assigned to each NH was used to merge the variables selected from each of the three datasets. The LTCCC aggregates the HPRD data across the four quarters within a given year. Thus, the merged data was organized to be consistent with this format.
Measures
The staffing levels in NHs were measured by HPRD, which has been shown to be a significant indicator of NH quality and safety (e.g., Spilsbury et al., 2011). HPRD is estimated by dividing a nursing home's daily staff hours by the number of NH residents. Two parameters or variables pertaining to HPRD were retrieved from the LTCCC data and included in this analysis. The first parameter was total direct care staff that refers to the daily hours of RNs, LPNs, and CNAs directly involved in resident care. In 2001, CMS published a congressionally mandated report on nursing staff that recommended a minimum standard of 4.1 hr of total direct care nursing time per resident per day (Centers for Medicare & Medicaid Services, 2001). Specifically, Pennsylvania had a minimum standard of 2.7 HPRD before the adjustment that increased to 2.87 HPRD starting July 1, 2023 (IntelyCare, n.d.).
The second parameter was the total number of RN direct care staff. The CMS recommended a minimum standard of 0.75 hr for RNs in 2001 (Centers for Medicare & Medicaid Services, 2001).
NH resident COVID-19 positive cases were retrieved from CMS (March 2023; data from May 2020 to December 2022). Resident COVID-19 cases were recoded as a dichotomized variable with 0 (no reported cases) and 1 (had at least one reported case). We included sociodemographic characteristics of the zip code where the NH is located to explore the potential influence of these characteristics on NH staffing levels, which has been conceptualized by the NIH/NIA Health Disparities Research Framework (Hill et al., 2015). Specifically, the current study included the proportion of Black residents (<40% vs. ≥40%, which aligns with the U.S. census estimate of approximately 40% of Black residents across Philadelphia county; U.S. Census Bureau, n.d.) income inequity as measured by the Gini index (Ceriani & Verme, 2012; Lerman & Yitzhaki, 1984), and average age were retrieved from the ACS (November 2022; data from 2016 to 2020). The Gini index and average age variables were mean-centered to better interpret the result.
Statistical Analysis
Descriptive statistical analysis was initially conducted to explore changes in HPRD (total direct care and RN) by the proportion of Black residents in each NH zip code from the first quarter of 2018 (2 years prior to the COVID-19 pandemic) through the fourth quarter of 2022. For both the total direct care and RN HPRDs, geometric means were calculated for each quarter.
Using a stratified variable categorizing the zip code proportion of Black residents (<40% vs. ≥40%), multilevel models (MLMs) were developed to examine the factors (i.e., linear time, NH resident COVID-19 positive cases, Gini index, and age) associated with NH HPRD from the second quarter of 2020 through the fourth quarter of 2022. The total direct care and RN HPRDs were log-transformed to adjust for skewed data to avoid violating the normality assumption. First, two unconditional MLMs with a random intercept and random slope were conducted to examine the variance of total direct care and RN HPRDs. Second, models that added linear time and NH resident COVID cases as predictors were introduced to examine the impact of COVID-19 infection on HPRDs. Lastly, two other MLMs were developed to include possible demographic covariates (i.e., Gini index, and age).
Results
Pattern Trends in Direct Care Staff HPRD
As shown in Figure 1, direct care staff HPRD in NHs across the Philadelphia zip code were consistently below the CMS recommendation of 4.1 HPRD prior and during COVID-19, but above the Pennsylvania standard of 2.7 HPRD (see Figure 1). NHs in zip codes with a high proportion of Black residents reported fewer direct staff HPRD after the outbreak of COVID-19 than those in zip codes with a lower proportion of Black residents. Beginning in the third quarter of 2021, the magnitude of the disparities in direct staff HPRD increases for all subsequent quarters (Figure 1).
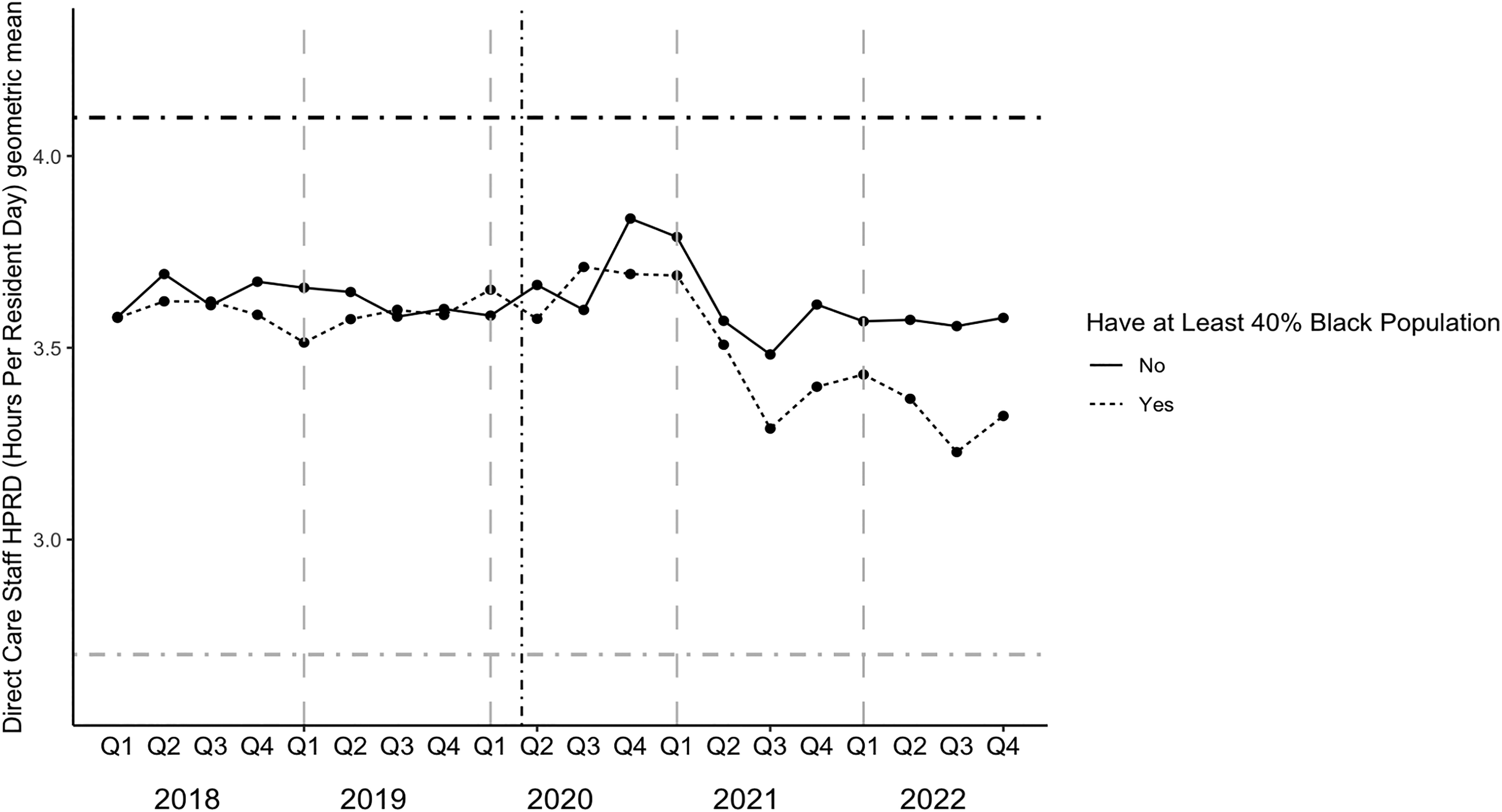
Direct Care Staff HPRD Pattern Trends in Nursing Homes Stratified by Philadelphia Zip Codes With High (>40% Black Community Residents) Versus Low (≤40% Black Community Residents) From 2018 to 2022. Note. The black horizontal dash-dotted line indicates the CMS standard of 4.1 hr recommended. The grey horizontal dash-dotted line indicates the Pennsylvania standard of 2.7 hr recommended before 07 January 2023. The black vertical dash-dotted line indicates the start of the COVID-19 pandemic in March 2020.
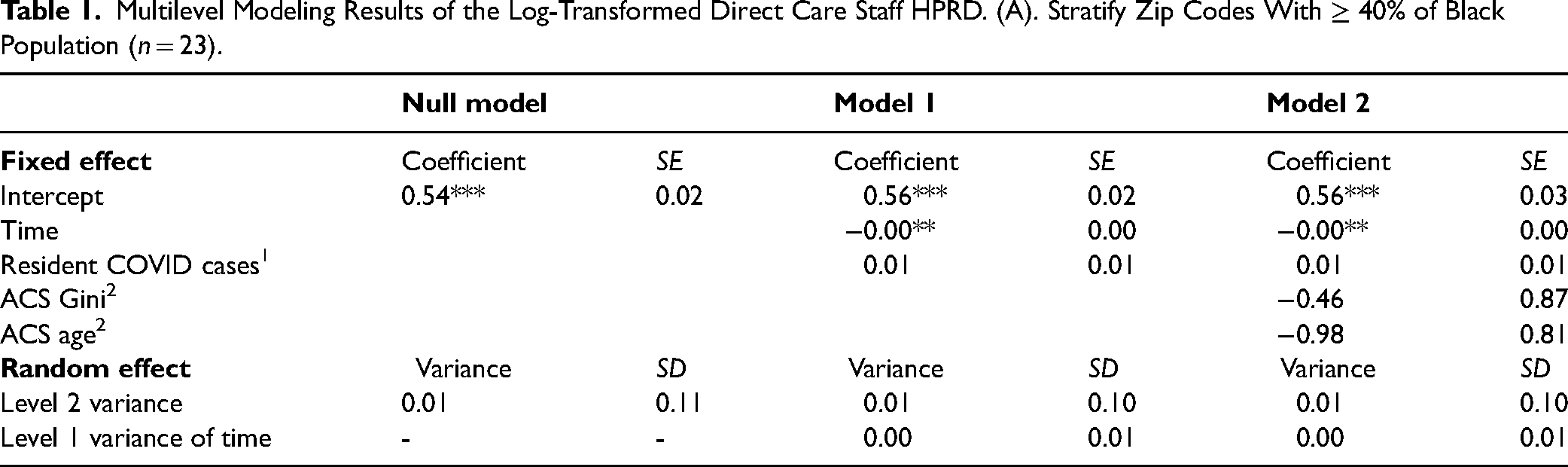
The MLM model in Table 1A revealed that direct staff HPRD significantly declined over time for NHs located in zip codes with a high proportion of Black residents (p < .01), even after adjusting for Gini index and age. Table 1B shows the MLM results of NHs located in the zip codes with a low proportion of Black residents (<40%). The fully adjusted MLM models indicated that for those NHs with at least one resident COVID-19 positive case, they were more likely to have higher direct care staff HPRD (p < .01) compared to NHs with no resident cases. However, time (measured in quarters) was not a significant predictor of HPRD for NHs with a low proportion of Black residents.
Multilevel Modeling Results of the Log-Transformed Direct Care Staff HPRD. (A). Stratify Zip Codes With ≥ 40% of Black Population (n = 23).
(B). Stratify Zip Codes With < 40% of Black Population (n = 25).
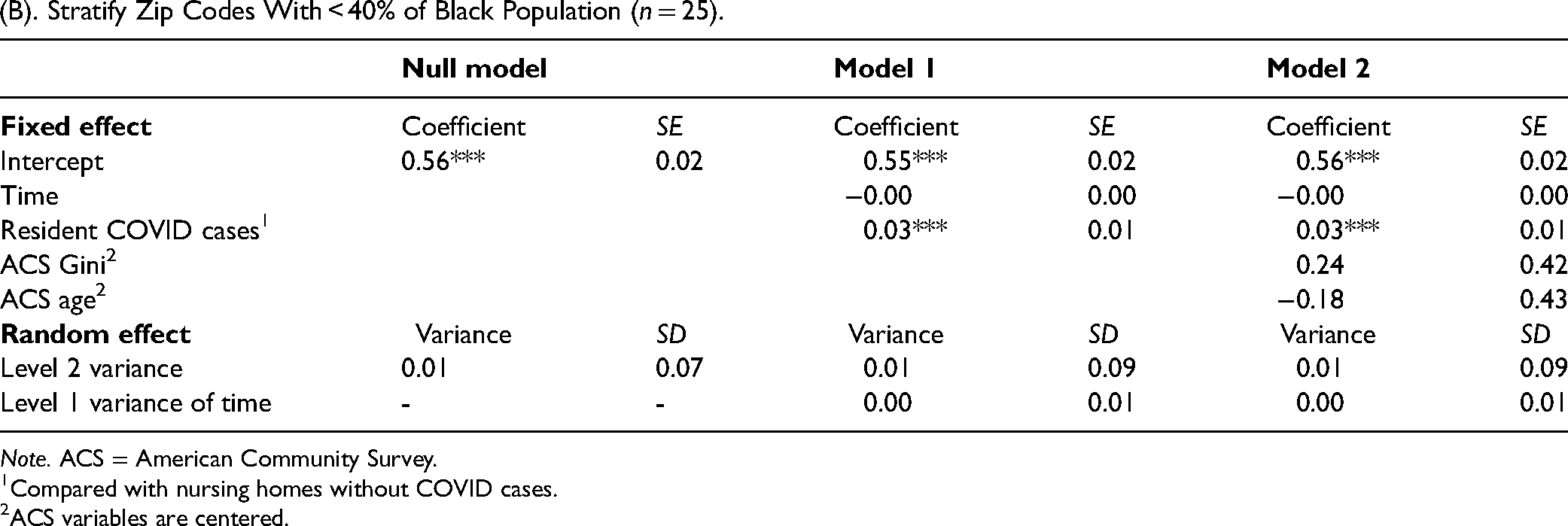
Note. ACS = American Community Survey.
Compared with nursing homes without COVID cases.
ACS variables are centered.
Pattern Trends in RN HPRD
Across all Philadelphia zip codes, RN HPRD was lower than the CMS recommendation of 0.75 hr, which was recommended in 2001 (see Figure 2). NHs in zip codes with a high proportion of Black residents reported less RN HPRD both before and after COVID-19 than those in zip codes with a lower proportion of Black residents. Beginning in the fourth quarter of 2020, RN HPRD was consistently reduced across all zip codes (Figure 2).
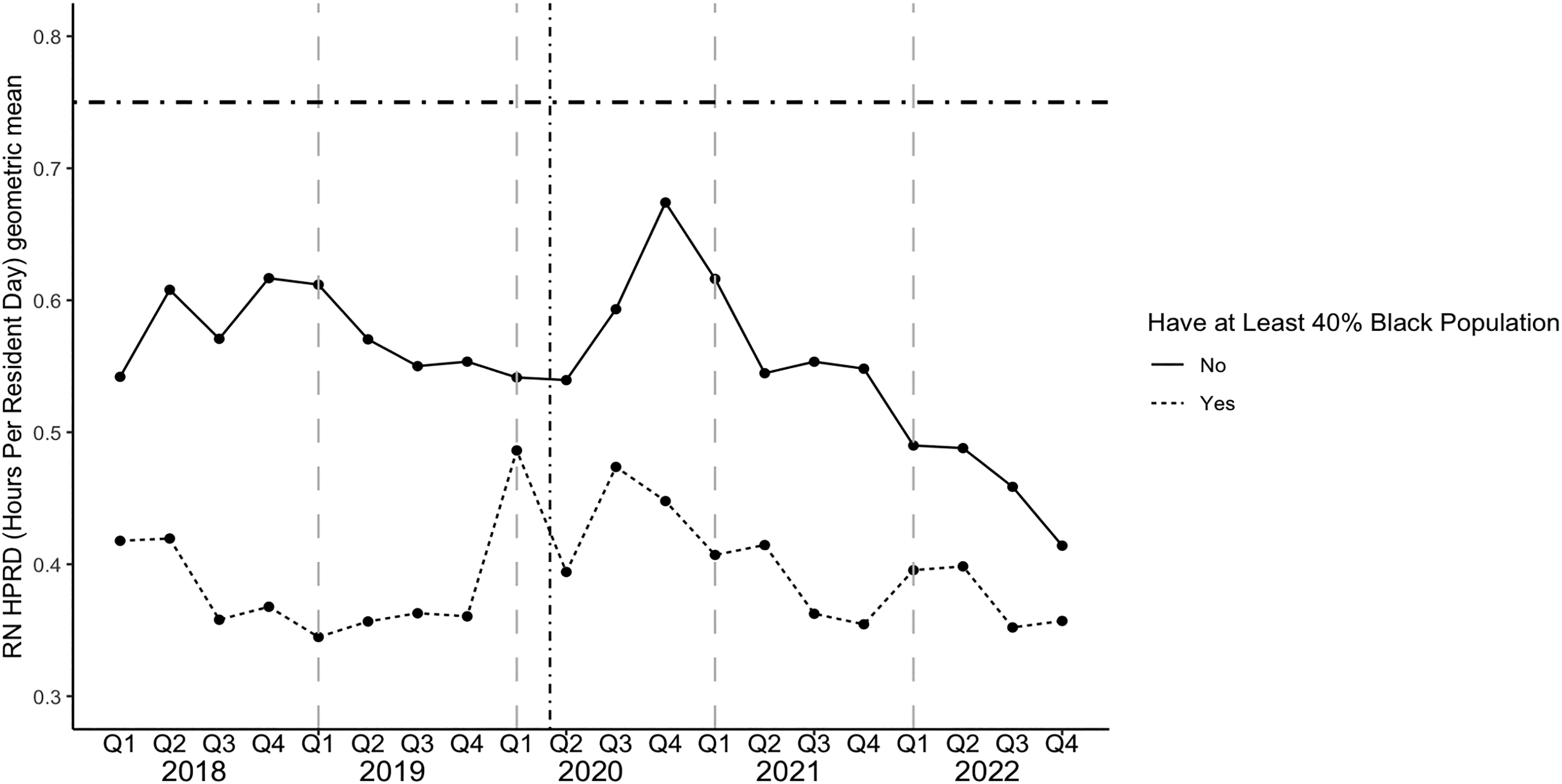
RN HPRD Pattern Trends in Nursing Homes stratified by Philadelphia Zip Codes With High (>40% Black community residents) Versus Low (≤40% Black Community Residents) From 2018 to 2022. Note. The horizontal dash-dotted line indicates the CMS standard of 0.75 hr. The vertical dash-dotted line indicates the start of the COVID-19 pandemic in March 2020.
Table 2 summarizes the MLM results predicting RN HPRD. In zip code locations with a high proportion of Black residents (≥40%), there were no significant associations between linear time or resident COVID-19 cases and RN HRPD. The results were consistent after adjusting for Gini index and age. The MLM model indicated RN HPRD significantly decreased over time (p < .01) in those zip codes that had a lower proportion of Black residents (<40%). NHs with at least one resident COVID-19 positive case were more likely to have higher RN HPRD (p < .01) compared to NHs with no resident case, even after adjusting for the Gini index and age.
Multilevel Modeling Results of the Log-Transformed RN HPRD. (A) Stratify zip Codes With ≥ 40% of Black Population (n = 23).
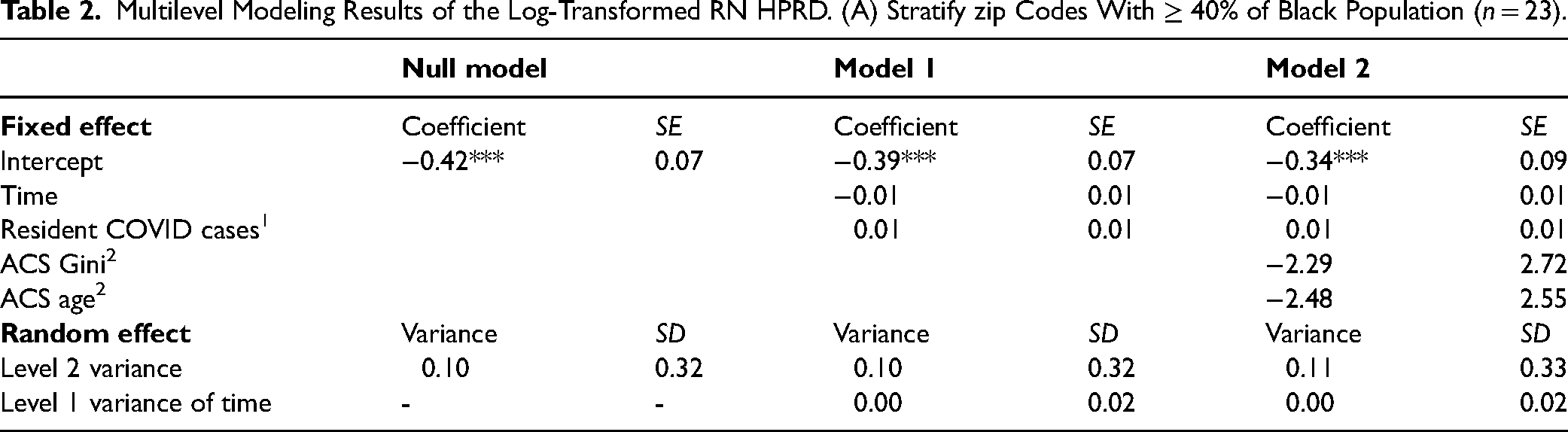
(B). Stratify Zip Codes With < 40% of Black Population (n = 25).
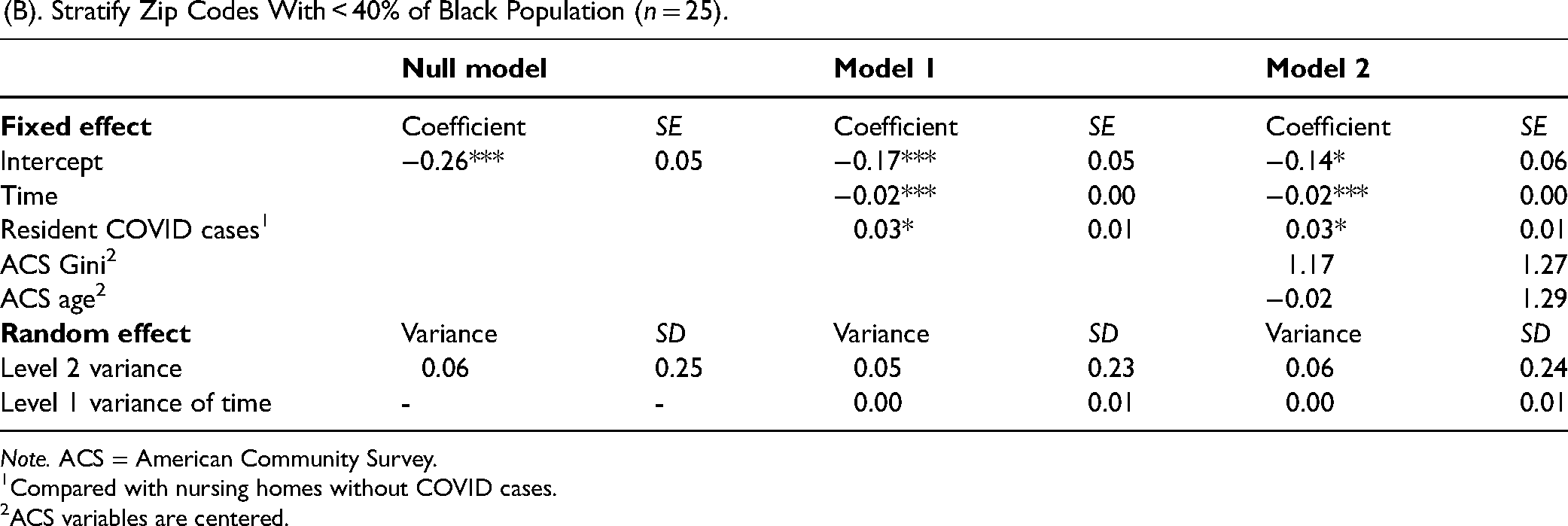
Note. ACS = American Community Survey.
Compared with nursing homes without COVID cases.
ACS variables are centered.
Discussion
This study observed that HPRD of total direct care nursing staff and that of direct care RN staff in NHs across Philadelphia zip codes changed from 2018 (prior to the COVID-19 pandemic) to 2022 (2 years into the COVID-19 pandemic). To authors’ knowledge, this is the first paper to explore the intersection among different systems (i.e., neighborhood, public health event and NHs). Our results showed that the HPRD for direct care staff in NHs across the Philadelphia zip code consistently fell below the CMS recommended standard of 4.1 HPRD prior and during COVID-19. Furthermore, there was a decrease in direct care staff HPRD after the outbreak of COVID-19 in 2021, in contrast to the relatively stable levels observed before the pandemic. We also found that HPRD for RNs in the Philadelphia area was lower than the CMS standard of 0.75 hr (recommended prior to September 2023). It is also important to note that, on September 1, 2023, CMS proposed a suggestion of lowering the minimum standard of total direct staff to 3.48 HPRD and of RNs to 0.55 HPRD (Centers for Medicare & Medicaid Services, 2023). It is still unclear how these potential changes on CMS standards could change staffing levels in Philadelphia NHs.
Our observations indicate that both direct care and RN HPRDs consistently fell below the CMS recommended standard before and after COVID-19, which align with some prior studies. For example, a study by Hawk et al. (2022) concluded that only 25% of skilled NHs met the CMS standard of 4.1 hr for direct care staff HPRD, and 41% met the standard of 0.75 hr for RN HPRD in 2019. Despite the observed increases in HPRD for some NH staff, HPRD still remained below the CMS standards (Hawk et al., 2022). However, given the significant relationship between nursing staff HPRD and quality of care in NHs, adequate staffing levels are still needed to improve NH quality (Shin et al., 2021; Spilsbury et al., 2011).
During the COVID-19 pandemic (2020 to 2022), a significant decline in direct care staff HPRD occurred in NHs located in Philadelphia zip codes with a high proportion of Black residents (≥40%). Notably, no significant change with time in RN HPRD was found during this period for NHs located in zip codes with a high proportion of Black residents. Instead, our descriptive analyses show that RN HPRD in NHs located in these zip codes with a high proportion of Black residents were consistently lower at each time point compared to those in zip codes with a lower proportion of Black residents. Interestingly, this finding is similar to prior work showing an association between the proportion of Blacks/African American nursing home residents and a lower ratio of RNs (Travers et al., 2023). One possible reason for this racial disparity is income. Areas with a high proportion of Black residents in Philadelphia are more likely to have a lower level of household income (Reardon et al., 2015). Future research could investigate whether NHs with lower RN HPRD levels are located in zip codes among the poorest in Philadelphia.
Our research expanded beyond previous findings on RNs and identified a significant decline in direct care staff HPRD specifically in NHs located in zip codes with a high proportion of Black residents. It is important to note that our study focused on the residential demographics of zip code where the NH is located rather than demographics of NH residents. This observation might provide some initial support for an intersection between the neighborhood/zip code and NH environment (Hill et al., 2015). Historical and prevailing systemic inequities and racism with respect to income, wealth, education, housing quality, and health resources in metropolitan areas with predominantly Black residents may likely transfer to resources available in NHs located in these areas (Chatters et al., 2020). As such, the older Black residents who require NH care may transit into NHs within their community and consequently experience prevailing inequities that impede the quality of their care in these facilities. The concept of “double jeopardy” further suggests that these racial inequities coupled with the inequities relevant to aging (e.g., quality of healthcare) increases the risk for poor health outcomes within older Black adults (Chatters et al., 2020).
Within NHs located in zip codes with a low (<40%) proportion of Black residents, a significant decline in RN HPRD was observed during the COVID-19 pandemic but no significant changes were found for direct care HPRD. Higher reported direct care HPRD and RN HPRD were associated with any reported COVID-19 cases within zip codes with a low proportion of Black residents. It is possible that NHs with a low proportion of Black residents were initially able to leverage more NH staff, particularly with higher skill levels of care from their RNs, as suggested by HPRD levels. As such, these NHs may have been able to manage COVID-19 cases within the facility. However, the observed decline in RN HPRD (starting in quarter 4 of 2020) may likely reflect the significant levels of staff burnout and attrition due to stress and moral distress. Despite these challenges, NH staff are expected to maintain their level of care for residents through creative methods given their limited resources. The efforts could include promoting new protocols, mandating staffing levels, and adding skilled nursing staffs (Wickersham, 2022). The COVID-19 pandemic is likely to have escalated these efforts for NH staff, particularly RNs, and created a predicament that is unsustainable and will likely increase NH staff turnover as well as long-term staff shortages (Nursing Home Commission, 2020). Additional research, however, is warranted to further monitor this pattern of decline, particularly for RN HPRD, as this would further support the “Herculean effort” and need to address the potential consequence of safety issues and poor quality of care of residents associated with low RN HPRD (Federal Register, 2023). Moreover, future research should investigate whether enhancing the representation of Black, Indigenous, and People of Color (BIPOC) nursing staff may reduce the health and quality of care disparities we have observed in U.S. NHs.
Limitations of the Study
The current study has limitations that should be considered. The study focused on the demographic characteristics of the zip code where NHs were located rather than the demographic characteristics of NHs residents (e.g., race of residents). This current study approach may limit the ability to make direct comparisons with other research examining the demographic characteristics of NHs residents and HPRD. However, the strength of our approach is that we explored the potential association between the neighborhood/zip code and NH environment. Our findings reflect that socioeconomic disparities between neighborhoods that vary by racial/ethnic composition (House & Williams, 2000) may be linked to the disparities in the quality of NH staffing care. Additionally, as this study focused on Philadelphia, PA, it included a small sample size of zip codes limiting the number of covariates. For future work on this topic, it may be beneficial to include potential meaningful covariates, such as NH characteristics (e.g., contracted or full-time NH staff; private or public provider). For example, contracted nursing staff is an important component of the medical workforce who can fill staffing vacancies (Bourbonniere et al., 2006). Specifically, there was a significant increase in average contract HPRD for RNs (300%), LPNs (376%), and NAs (414%) during COVID-19 (Zhang et al., 2023). Although contract staff in nursing homes was heightened during the COVID-19 pandemic, the total number of HPRD by all NH-employed staff (contracted and full-time) declined (Zhang et al., 2023). Prior research indicated that often, compared with full-time RNs, contract and part-time RNs provide a lower level of care quality because they lack knowledge about patients (Weech-Maldonado et al., 2004). Therefore, full-time nursing staff HPRD might need to be distinguished from contracted nursing staff HPRD.
Lastly, the current study's focus on Philadelphia may limit the generalizability of the current observations in other geographic areas across the state of PA and the United States. For example, Yang et al. (2021) found a greater increase in staffing shortages in rural nursing homes compared with nursing homes in urban areas during COVID-19. Since our research found significant disparities in the NH staffing quality within an urban area, it would be beneficial to expand our current study approach to explore whether disparate patterns of HPRD are also observed between NHs located in urban vs rural areas.
Conclusion
Staffing levels, as measured by HPRD, are pertinent to the safety and quality of care of NH residents (Federal Register, 2023; Harrington et al., 2020; Shin et al., 2021; Spilsbury et al., 2011). Thus, federal and state standards are essential to ensuring that NH providers are addressing the needs of residents. NH providers may be reluctant to meet federal minimal standards for nursing staff HPRD due to projected anticipated staffing cost increases (Federal Register, 2023). With states not encouraging both total direct staff HPRD and more specific individual staff HPRD (RN HPRD), there is an increased possibility that facilities would choose to hire more non-RN staff to meet the total direct staff requirements, given that the average salaries for these staff (e.g., NAs—$16.90/hr) tend to be approximately half the salaries of more skilled staff (e.g., RNs—$37.11/hr; Federal Register, 2023). Thus, it is necessary to establish individual staffing standards for RNs in NHs, in addition to total direct staff standards at the state level. Currently, the state of Pennsylvania does not have a clear minimum RN NH staff standard like several other U.S. states. Future research should extend our findings to include other individual staffing categories, such as LPNs.
To meet the RN HPRD CMS minimal recommendations, it is estimated that an urban area, such as Philadelphia, in the state of Pennsylvania, would need an increase of 3.2% in the number of RNs (Federal Register, 2023). Given our current findings of clear disparities in HPRD based on the racial residential composition across zip codes, additional research is warranted to estimate the proportions of RNs that will likely be needed to enhance the equity of RNs meeting this minimal CMS recommendation across zip codes. If states, such as Pennsylvania, attempt to meet the total direct care staff CMS recommendations, it is projected that over 10 years, there will be a savings of $2.55 billion in Medicare costs due to a reduced number of hospitalizations and emergency department visits (Federal Register, 2023). Pennsylvania has recently made promising adjustments to the state's minimum HPRD for NH direct care staff (e.g., 2.87 as of 07/01/2023 and planned adjustment of 3.2 in 07/01/2024) (IntelyCare, n.d.), which is an indication of the state recognizing the importance of NH staffing and quality of care. However, these state minimum standards are still below what is needed for safe and quality nursing care. The current study's findings provide additional support for U.S. states such as Pennsylvania to consider additional adjustments to the state HPRD standards, particularly setting a minimal state standard for RN HPRD.
It is also recommended that states such as Pennsylvania should strive to further increase their standard for HPRD given the evidence that a limited number of U.S. states that have incorporated high staffing standards showed higher levels of nursing HPRD, lower safety concerns, and better quality of care (IntelyCare, n.d.; Mueller et al., 2006). As the aging population is increasing in the United States, it is anticipated there will be an increase of older adults with functional limitations and complex health comorbidities requiring more supervised and skilled care of NHs (Bakerjian et al., 2021). As such, future adjustments to the HPRD federal and state standards will likely be necessary for the potential increasing demand for this type of care for the U.S. aging population. More importantly, increased efforts may be needed to monitor potential inequities in HPRD and quality of care based upon race/ethnicity, geographic location, and socioeconomics. This additional monitoring may be useful for incorporating strategies to facilitate equitable healthcare practices and outcomes, which can reduce observed aging and health disparities.
Supplemental Material
sj-docx-1-ppn-10.1177_15271544241270061 - Supplemental material for The Impact of the COVID-19 Pandemic on Staffing Levels in Philadelphia Nursing Homes: Disparities Based on the Racial Composition of Geographical Areas
Supplemental material, sj-docx-1-ppn-10.1177_15271544241270061 for The Impact of the COVID-19 Pandemic on Staffing Levels in Philadelphia Nursing Homes: Disparities Based on the Racial Composition of Geographical Areas by Junyan Tian, Alyssa A. Gamaldo, Kamesh Madduri, Carlos Tavares, Noble Maseru, David Saunders and Gary King in Policy, Politics, & Nursing Practice
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Pennsylvania Department of Health (Grant No. 4400023298).
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.